How often should you have your teeth cleaned? For most healthy adults, professional dental cleanings are recommended every six months. However, individuals with a history of periodontal disease, systemic health conditions, or high caries risk may require cleanings every three to four months to maintain optimal oral health.
Clinical Summary:
Professional dental prophylaxis frequency should be individualized based on clinical risk assessments rather than a universal timeline. While biannual visits suffice for patients with excellent oral hygiene and no underlying conditions, high-risk profiles necessitate accelerated recall schedules to prevent irreversible attachment loss and systemic inflammation. A comprehensive evaluation by a dental professional determines the precise interval required to disrupt biofilm maturation, manage calculus accumulation, and preserve long-term dentition.
Key Takeaways:
- Biannual cleanings (every six months) remain the baseline standard for patients with healthy gingiva and low decay risk.
- Patients with active periodontal disease or systemic conditions like diabetes require a three-to-four-month recall schedule.
- Professional prophylaxis removes hardened calculus that daily brushing and flossing cannot eliminate.
- Deep cleaning (scaling and root planing) is a distinct therapeutic procedure, not a routine preventive measure.
- Personalized risk assessment by a qualified dental professional determines your ideal cleaning frequency.
The Standard Recommendation: Is Every Six Months Still Accurate?
The traditional six-month cleaning interval serves as a reliable baseline for preventive care, though modern dentistry emphasizes personalized schedules based on individual clinical risk factors.
For decades, the standard advice echoed by dental professionals worldwide has been to schedule a routine dental cleaning and examination twice a year. This biannual recommendation has become deeply ingrained in public health consciousness and forms the structural basis for most preventive dental insurance plans. However, as clinical research evolves, the paradigm is shifting from a one-size-fits-all approach to a highly individualized model of care. Understanding the biological rationale behind these recommendations is essential for patients seeking to optimize their oral health.
Historical Context vs. Modern Clinical Evidence
The origin of the six-month dental visit is often traced back to early public health campaigns rather than rigorous scientific trials. While this interval has proven highly successful in reducing the overall prevalence of severe dental decay and tooth loss in the general population, modern evidence-based dentistry requires a more nuanced approach. According to Dr. Nguyen Van Cuong, a leading expert in comprehensive oral care, a rigid biannual schedule may over-treat patients with pristine oral hygiene while dangerously under-treating those with aggressive periodontal pathogens.
Recent clinical guidelines suggest that a patient’s recall interval should be dictated by their specific susceptibility to oral diseases[1]. For a young adult with no history of cavities, excellent salivary flow, and meticulous home care, a six-month interval provides ample opportunity for a clinician to monitor health and remove minor plaque accumulations. Conversely, a patient exhibiting early signs of gingival inflammation requires more frequent interventions to halt disease progression. This personalized approach is a cornerstone of modern General Dentistry, ensuring that preventive resources are allocated effectively based on biological need.
The Role of Plaque and Calculus Formation
To understand why professional cleanings are necessary, one must understand the lifecycle of dental biofilm. The human mouth is a complex ecosystem hosting hundreds of bacterial species. Within minutes of brushing, a proteinaceous pellicle forms over the enamel, providing an adhesive surface for primary bacterial colonizers. Over the next 24 to 48 hours, these bacteria multiply, forming a sticky, colorless matrix known as dental plaque.
If plaque is not mechanically disrupted through effective brushing and flossing, it begins to mineralize. Saliva contains high concentrations of calcium and phosphate ions, which precipitate into the plaque matrix, transforming it into calculus (commonly known as tartar). Calculus is highly porous and acts as a permanent reservoir for pathogenic bacteria. Once calculus forms, it bonds tightly to the microscopic irregularities of the tooth surface and cannot be removed by at-home oral hygiene tools.

The rate at which plaque mineralizes into calculus varies dramatically among individuals. Factors influencing this rate include salivary pH, dietary habits, and genetic predispositions. For some, calculus forms rapidly within a few weeks, necessitating more frequent professional intervention to prevent the underlying gingival tissue from becoming chronically inflamed. Professional cleanings utilize specialized instruments to safely fracture and remove these hardened deposits, resetting the biological clock on biofilm maturation.
Risk Factors Dictating Cleaning Frequency
Your ideal cleaning schedule is determined by a combination of periodontal health, systemic diseases, lifestyle habits, and the presence of complex dental restorations.
Determining how often you should have your teeth cleaned requires a comprehensive clinical risk assessment. Dental professionals evaluate a multitude of variables to categorize a patient’s risk profile as low, moderate, or high. This stratification directly informs the recommended recall interval, ensuring that therapeutic interventions occur before irreversible tissue damage transpires.
Periodontal Disease and Gingivitis
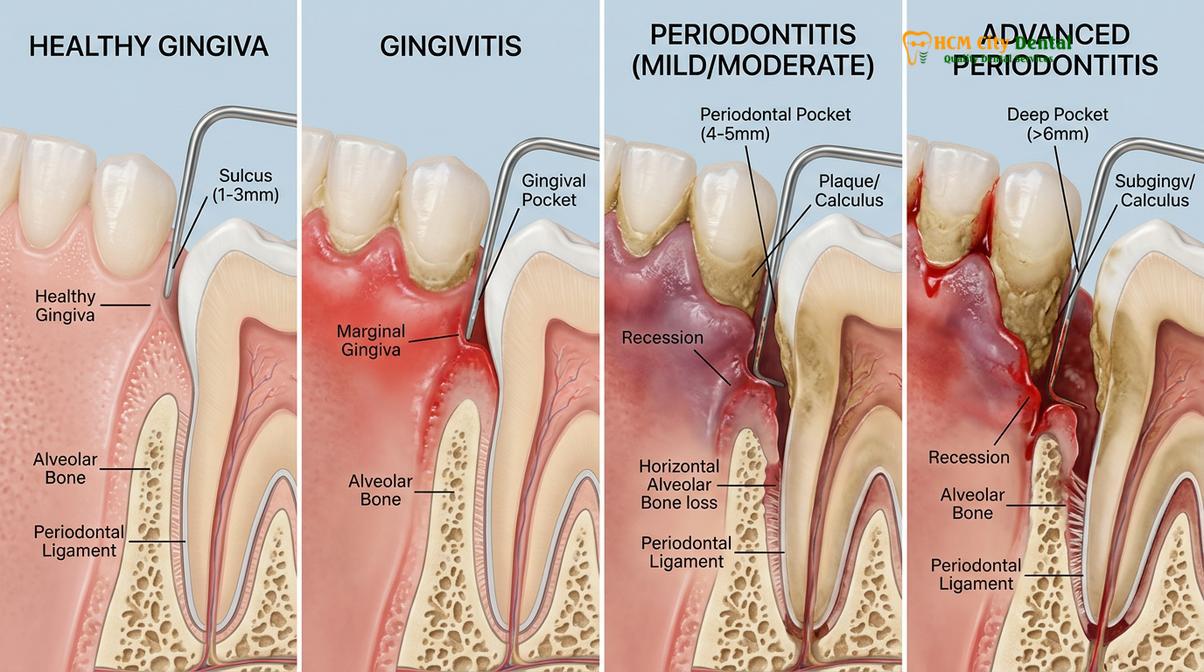
The most significant determinant of cleaning frequency is the health of the periodontium—the specialized tissues that surround and support the teeth. Gingivitis, the earliest stage of gum disease, is characterized by red, swollen gums that bleed easily upon probing or brushing. Because gingivitis is reversible, patients diagnosed with this condition are often placed on a three-to-four-month recall schedule to aggressively manage bacterial loads and allow the tissues to heal.
If gingivitis progresses to periodontitis, the inflammatory response begins to destroy the alveolar bone and periodontal ligaments. This creates deep periodontal pockets around the teeth, which serve as anaerobic incubators for highly destructive bacteria. Patients with a history of periodontitis are universally recommended to undergo periodontal maintenance therapy every three to four months[2]. This accelerated schedule is critical because it takes approximately 90 to 120 days for pathogenic bacteria to repopulate these deep pockets to destructive levels following a professional cleaning.
“Periodontal maintenance is not merely a routine cleaning; it is an ongoing therapeutic intervention designed to arrest bone loss and preserve the natural dentition in highly susceptible patients.”
Systemic Health Conditions
The oral cavity is not an isolated system; it is intimately connected to overall systemic health. A robust body of medical literature has established bidirectional relationships between chronic oral inflammation and various systemic diseases. Patients with specific medical conditions often require more frequent dental cleanings to manage these interconnected risks.
- Diabetes Mellitus: Diabetic patients, particularly those with poorly controlled blood glucose levels, are at a significantly higher risk for severe periodontal disease. Conversely, active gum infection can cause insulin resistance, making it harder to control blood sugar. Frequent cleanings help break this destructive cycle.
- Cardiovascular Disease: Oral bacteria can enter the bloodstream through inflamed gums, potentially contributing to the formation of arterial plaques and increasing the risk of endocarditis. Cardiologists frequently collaborate with dentists to ensure their patients maintain pristine oral hygiene.
- Pregnancy: Hormonal fluctuations during pregnancy exaggerate the gingival response to plaque, leading to “pregnancy gingivitis.” Maintaining a rigorous cleaning schedule during gestation is vital for maternal comfort and has been linked to better overall birth outcomes.
Orthodontic Appliances and Restorations
The physical landscape of the mouth also dictates cleaning frequency. Patients undergoing active orthodontic treatment with traditional brackets and wires face significant challenges in maintaining oral hygiene. These appliances create numerous plaque traps, dramatically increasing the risk of enamel decalcification and dental caries. Orthodontic patients are frequently advised to schedule cleanings every three to four months to mitigate these risks.
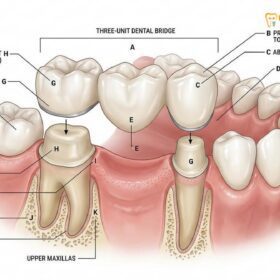
Similarly, patients with extensive dental restorations—such as a full dental bridge, multiple crowns, or dental implants—require meticulous professional maintenance. The margins where restorative materials meet natural tooth structure are highly susceptible to recurrent decay and plaque accumulation. Frequent professional monitoring ensures the longevity of these complex restorative investments.
The Clinical Workflow of a Professional Dental Cleaning
A professional dental cleaning involves a systematic process of diagnostic evaluation, ultrasonic scaling, precise hand instrumentation, and protective fluoride application to ensure comprehensive oral health.
A professional dental cleaning, clinically termed oral prophylaxis, is a highly structured medical procedure performed by a licensed dental hygienist or dentist. It is far more comprehensive than simply brushing and flossing. The workflow is designed to systematically evaluate oral health, remove pathogenic deposits, and fortify the teeth against future bacterial attacks.
Comprehensive Examination and Diagnostic Imaging
Before any physical cleaning begins, the clinician conducts a thorough review of the patient’s medical history, noting any changes in medications or systemic health that could impact dental care. This is followed by a comprehensive extraoral and intraoral examination, screening for oral cancer, temporomandibular joint (TMJ) disorders, and signs of mucosal pathology.
Diagnostic imaging, such as digital bitewing or periapical radiographs, may be prescribed based on the patient’s clinical needs. These images allow the dentist to visualize interproximal decay (cavities between the teeth), assess alveolar bone levels, and evaluate the health of tooth roots. Following the visual and radiographic assessment, the clinician performs periodontal probing. Using a calibrated instrument, they measure the depth of the gingival sulcus around each tooth. Healthy pockets typically measure 1 to 3 millimeters, while depths of 4 millimeters or greater indicate active inflammation or attachment loss.
Ultrasonic Scaling and Hand Instrumentation
The core therapeutic phase of the cleaning involves the meticulous removal of plaque and calculus. Modern dental practices typically utilize a combination of ultrasonic technology and traditional hand instrumentation to achieve optimal results[3].
The process usually begins with an ultrasonic scaler. This advanced device features a specialized metal tip that vibrates at high frequencies (typically between 25,000 and 30,000 cycles per second). The rapid vibration shatters the crystalline structure of calculus deposits. Simultaneously, the device emits a continuous stream of water, which serves a dual purpose: it cools the instrument tip and creates microscopic cavitation bubbles. When these bubbles implode, they generate shockwaves that disrupt bacterial cell walls and flush debris from the gingival sulcus.
Following ultrasonic scaling, the clinician utilizes precise hand instruments, such as curettes and scalers, to meticulously fine-tune the cleaning. Hand instrumentation allows for tactile sensitivity, enabling the practitioner to detect and remove microscopic remnants of calculus hidden beneath the gumline or nestled in complex root anatomies. This step is crucial for creating a perfectly smooth root surface, which discourages future bacterial adhesion.

Polishing and Fluoride Varnish Application
Once all hard deposits are removed, the teeth are polished to remove extrinsic stains caused by coffee, tea, tobacco, or certain foods. The clinician uses a slow-speed handpiece equipped with a soft rubber cup and a specialized prophylactic paste. This paste contains mild abrasives that gently buff the enamel, leaving it smooth and glossy. A smooth enamel surface is not only aesthetically pleasing but also biologically beneficial, as it makes it more difficult for new plaque to adhere.
The final step in the preventive workflow is often the application of a professional-grade fluoride varnish. Fluoride is a naturally occurring mineral that plays a critical role in enamel remineralization. When applied topically, it integrates into the hydroxyapatite structure of the tooth, converting it into fluorapatite—a compound that is significantly more resistant to acid attacks from cariogenic bacteria. This protective measure is especially beneficial for patients with a high risk of decay, exposed root surfaces, or dentin hypersensitivity.
Comparing Routine Prophylaxis vs. Deep Cleaning (Scaling and Root Planing)
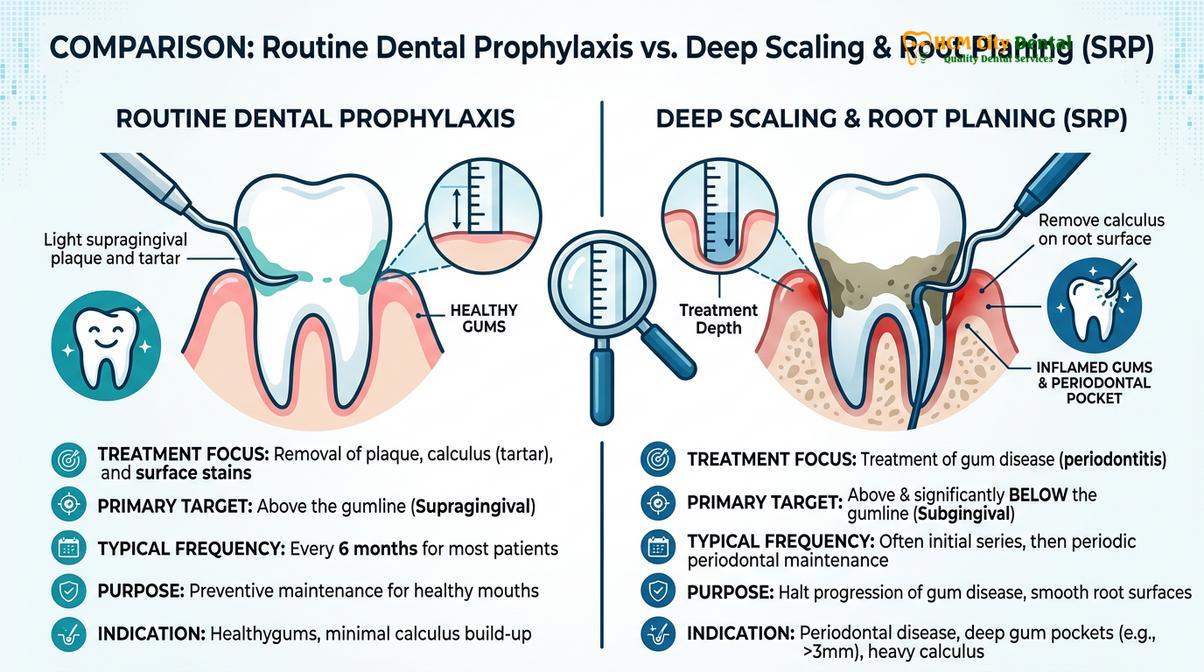
Routine prophylaxis focuses on preventive maintenance above the gumline, whereas deep cleaning is a therapeutic intervention designed to treat active periodontal disease beneath the gingival margins.
A common point of confusion among patients is the distinction between a standard dental cleaning and a “deep cleaning.” While both procedures aim to improve oral health, they serve entirely different clinical purposes, target different anatomical areas, and are prescribed based on distinct diagnostic criteria. Understanding this difference is vital for patients navigating their treatment options.
Indications for Standard Prophylaxis
A standard prophylaxis (often billed under the ADA code D1110) is a preventive procedure intended for patients who exhibit a generally healthy periodontium. The primary objective is to maintain health and prevent the onset of disease. During a routine prophylaxis, the clinician focuses on removing plaque, calculus, and stains from the supragingival environment—meaning the visible portions of the teeth above the gumline.
This procedure is appropriate for patients with localized, mild gingivitis, provided there is no evidence of clinical attachment loss or bone destruction. Because the instrumentation is primarily confined to the enamel surfaces and shallow, healthy sulci, a standard prophylaxis is typically comfortable and does not require the administration of local anesthesia.
When Deep Cleaning is Medically Necessary
When a patient is diagnosed with active periodontitis—characterized by periodontal pockets measuring 4 millimeters or deeper, bleeding upon probing, and radiographic evidence of bone loss—a standard prophylaxis is clinically insufficient. In fact, performing a superficial cleaning on a patient with deep periodontal pockets can be counterproductive, as it may cause the gingival tissue to tighten around the tooth, sealing aggressive bacteria deep within the pocket.
In these scenarios, a therapeutic procedure known as Scaling and Root Planing (SRP) is medically necessary[4]. SRP is a meticulous, non-surgical treatment designed to halt the progression of periodontal disease. The “scaling” component involves the thorough removal of calculus and bacterial toxins from deep beneath the gumline. The “root planing” component involves smoothing the rough surfaces of the tooth roots, removing necrotic cementum, and creating a biologically acceptable environment for the gingival tissues to reattach.
Because SRP involves extensive subgingival instrumentation in inflamed tissues, it is almost always performed under local anesthesia to ensure patient comfort. The procedure is often divided into multiple appointments, treating one or two quadrants of the mouth per visit. Following SRP, patients are transitioned to a rigorous periodontal maintenance schedule (typically every three to four months) to monitor healing and prevent disease recurrence.
| Clinical Parameter | Routine Prophylaxis (Standard Cleaning) | Scaling and Root Planing (Deep Cleaning) |
|---|---|---|
| Primary Objective | Preventive maintenance; maintaining existing health. | Therapeutic intervention; treating active disease. |
| Target Area | Supragingival (above the gumline) and shallow sulci. | Subgingival (deep beneath the gumline) and root surfaces. |
| Patient Profile | Healthy gums or mild, reversible gingivitis. | Active periodontitis, deep pockets, bone loss. |
| Anesthesia Requirement | Rarely required; generally painless. | Local anesthesia is standard for patient comfort. |
| Frequency | Typically every 6 months. | Followed by maintenance every 3-4 months. |
For general dentists seeking to expand their clinical repertoire and better understand the intersection of periodontal health and complex restorative or orthodontic movements, advanced education is highly beneficial. Exploring Orthodontic Courses for General Dentists can provide deeper insights into managing the unique periodontal challenges presented by malocclusion and appliance therapy.
When to See a Doctor (Important Clinical Considerations)
While adhering to a personalized cleaning schedule is the foundation of preventive care, certain acute symptoms require immediate clinical evaluation outside of your routine recall interval. Ignoring these warning signs can allow minor issues to rapidly escalate into severe infections, potentially requiring complex interventions such as wisdom teeth removal or endodontic therapy.
Clinical Red Flags: Seek immediate dental evaluation if you experience spontaneous gingival bleeding, persistent halitosis (bad breath) that does not resolve with brushing, sudden tooth mobility, localized swelling, or acute thermal sensitivity. These are hallmark signs of active infection or rapid periodontal breakdown.
It is crucial to understand that early-stage dental diseases are often asymptomatic. A patient may have active decay or progressive bone loss without experiencing any pain. This silent progression underscores the absolute necessity of professional diagnostic evaluations. If you are experiencing unexplained discomfort, consulting a Comprehensive Guide to Tooth Pain can provide initial context, but it cannot replace a definitive clinical diagnosis.
Clinical Case Review: A 45-year-old patient visited HCMC Dental Clinic in Ho Chi Minh City after avoiding dental care for five years due to anxiety. The patient reported no pain but noticed occasional bleeding when brushing. Upon comprehensive evaluation, Dr. Nguyen Van Cuong diagnosed moderate periodontitis with localized 5mm pockets. A standard cleaning would have been insufficient. Instead, a targeted Scaling and Root Planing protocol was initiated under local anesthesia. Following the therapy, the patient was placed on a strict 3-month periodontal maintenance schedule. Within six months, tissue inflammation resolved, pocket depths reduced to healthy 2-3mm levels, and the patient successfully retained their natural dentition without the need for surgical intervention.

“The absence of pain does not equate to the presence of health. Regular professional evaluations are the only definitive method to detect and intercept oral pathologies before they compromise the integrity of the dentition.”
Ultimately, the frequency of your dental cleanings should be a collaborative decision made between you and your dental provider. By prioritizing regular visits, adhering to meticulous home care, and responding promptly to clinical warning signs, you can maintain a healthy, functional, and aesthetic smile for a lifetime. For personalized recommendations and comprehensive diagnostic care, scheduling a consultation at a reputable facility like HCMC Dental Clinic ensures your treatment plan is tailored to your unique biological needs[5].
Frequently Asked Questions
How much does a professional teeth cleaning usually cost?
The cost of a professional teeth cleaning varies based on geographic location, clinic expertise, and whether you need routine prophylaxis or deep scaling. Most standard cleanings are highly affordable and often fully covered by preventive dental insurance plans. For uninsured patients, clinics typically offer transparent fee schedules. If advanced periodontal therapy is required, the investment will be higher due to the complexity and time involved.
Does getting your teeth cleaned hurt?
A routine professional teeth cleaning is generally painless for individuals with healthy gums and minimal calculus buildup. You may feel slight pressure or vibration from the ultrasonic scaler. If you suffer from dentin hypersensitivity or severe gingival inflammation, you might experience mild discomfort. In such cases, your dental hygienist or dentist can apply a topical numbing gel or local anesthetic to ensure a comfortable experience.
Can I skip professional cleanings if I brush and floss daily?
No, daily brushing and flossing cannot replace professional dental cleanings. While excellent home care removes soft plaque, it cannot remove calculus (tartar)—the hardened bacterial deposits that adhere firmly to enamel and root surfaces. Only professional dental instruments can safely fracture and remove calculus. Skipping professional cleanings allows these deposits to trigger chronic inflammation, eventually leading to irreversible periodontal disease and potential tooth loss.
How long does a standard dental cleaning take?
A standard routine dental cleaning typically takes between 30 to 60 minutes to complete. This timeframe allows the clinician to perform a comprehensive oral examination, conduct periodontal probing, remove plaque and calculus, polish the enamel, and apply fluoride. If it has been several years since your last visit, or if you have heavy tartar accumulation, the appointment may take longer or require a secondary visit.
Is it safe to have teeth cleaned during pregnancy?
Yes, it is entirely safe and highly recommended to have your teeth cleaned during pregnancy. Hormonal fluctuations during pregnancy can exaggerate the body’s inflammatory response to plaque, leading to pregnancy gingivitis. Routine cleanings help mitigate this risk. Obstetricians and dental professionals universally agree that maintaining optimal oral health during pregnancy is crucial for both maternal well-being and the systemic health of the developing baby.
References
- Journal of the American Dental Association. Evidence-based clinical recommendations on regular dental visits. (2013).
- Journal of Periodontology. The relationship between oral health and systemic disease: A clinical overview. (2020).
- International Journal of Dental Hygiene. Efficacy of ultrasonic scaling versus hand instrumentation in calculus removal. (2018).
- Clinical Oral Investigations. Periodontal maintenance therapy and long-term tooth retention. (2021).
- British Dental Journal. Patient compliance and clinical outcomes in individualized recall intervals. (2019).