The dental procedure apicoectomy, frequently referred to in clinical settings as root-end surgery, is a specialized microsurgical intervention designed to remove the infected tip of a tooth’s root and seal the surrounding canal. It is typically indicated when a standard non-surgical root canal treatment fails to resolve persistent periapical inflammation, offering a highly effective, conservative method to save the natural tooth from extraction.
Clinical Summary:
An apicoectomy is a highly effective endodontic microsurgery designed to salvage a natural tooth that has previously undergone root canal therapy but continues to exhibit signs of apical periodontitis. By surgically accessing the alveolar bone, resecting the infected root apex, and placing a biocompatible retrograde filling, clinicians can permanently eradicate the bacterial reservoir. This procedure offers a conservative, biologically sound alternative to tooth extraction and subsequent prosthetic replacement, boasting exceptionally high long-term success rates when performed with modern magnification, ultrasonic preparation, and advanced bioceramic materials.
Key Takeaways:
- An apicoectomy targets persistent bacterial infection at the root tip (apex) following an unsuccessful root canal treatment.
- The surgical workflow involves removing infected periapical tissue, resecting the terminal 3mm of the root, and placing a retrograde seal.
- It serves as a conservative, tooth-saving alternative to extraction and dental implant placement.
- Advanced 3D imaging (CBCT) and high-powered surgical microscopes significantly enhance the precision and predictability of the surgery.
- Post-operative recovery is generally straightforward, with minor localized swelling and discomfort resolving within a few days.
Understanding the Dental Procedure Apicoectomy
An apicoectomy is a targeted endodontic surgery that addresses persistent infection at the root apex by surgically resecting the root tip and sealing the canal retrogradely to preserve the natural tooth.
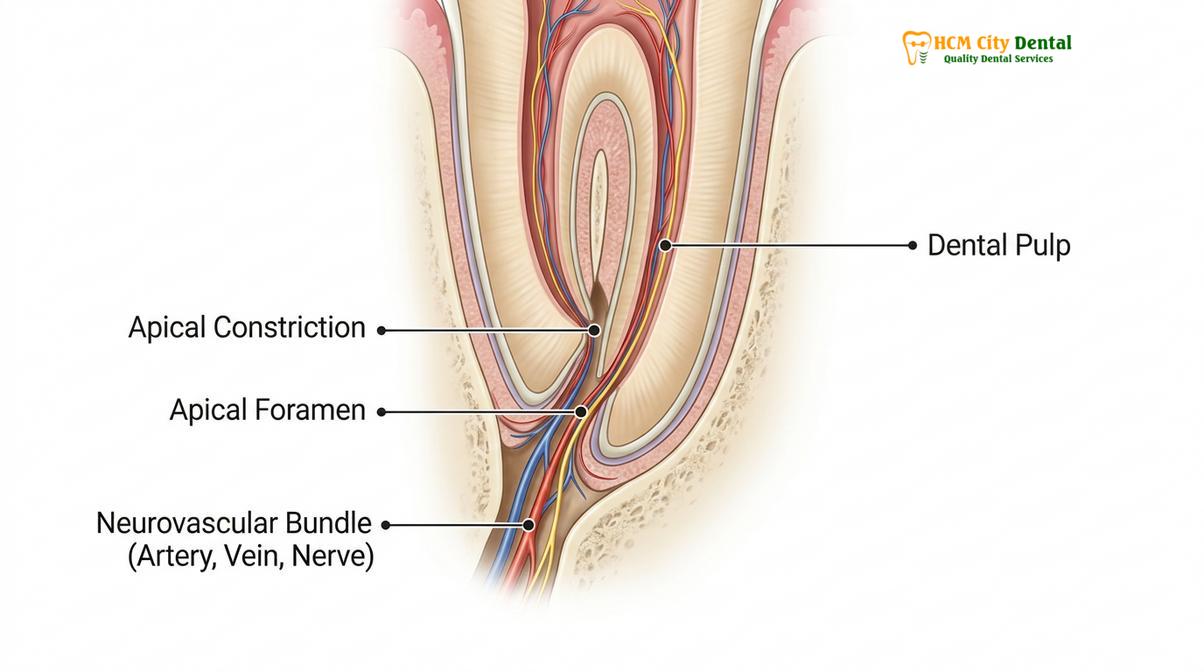
To fully comprehend the necessity and mechanics of the dental procedure apicoectomy, one must first understand the intricate anatomy of the human tooth and its surrounding structures. A tooth is not a solid block of enamel and dentin; rather, it houses a complex internal network known as the root canal system. This system contains the dental pulp—a vital tissue comprising nerves, blood vessels, and connective tissue. When this pulp becomes irreversibly inflamed or necrotic due to deep caries, trauma, or repeated restorative procedures, a standard root canal treatment is performed to clean, shape, and seal the internal space. However, the root canal system is rarely a simple, straight tube. It is a highly complex anatomical labyrinth, often featuring accessory canals, apical deltas, fins, isthmuses, and microscopic lateral branches that standard endodontic files and chemical irrigants cannot always fully debride. [1]
When microscopic bacteria manage to survive the initial root canal therapy and harbor in these inaccessible anatomical complexities, they can slowly leak toxins into the surrounding periapical tissues (the bone and ligaments surrounding the root tip). This chronic bacterial leakage triggers an immune response, leading to persistent inflammation, localized bone destruction, and the formation of a periapical cyst or granuloma. The term “apicoectomy” is derived from “apico,” referring to the apex or tip of the root, and “ectomy,” meaning surgical removal. Therefore, the procedure involves the surgical excision of the root’s terminal end, which is often the epicenter of the persistent infection.
In modern General Dentistry, the paradigm has shifted heavily toward the preservation of the natural dentition whenever clinically viable. While dental implants are excellent prosthetic replacements, nothing functions quite as perfectly as a natural tooth with its intact periodontal ligament, which provides crucial proprioceptive feedback during mastication. Dr. Nguyen Van Cuong, a leading advocate for conservative dental practices, frequently emphasizes that saving a structurally sound natural tooth through apical surgery is almost always preferable to extraction. The apicoectomy procedure allows the clinician to physically access the external surface of the root, directly visualize the source of the failure, and mechanically remove the infected tissue and the complex apical anatomy that harbors the biofilm.
The biological rationale behind the procedure is straightforward yet profound: by removing the apical 3 millimeters of the root, the surgeon eliminates approximately 98% of the apical ramifications and 93% of the lateral canals, which are the primary hiding spots for residual bacteria. Once this infected anatomical segment is removed, the surgeon can prepare a small cavity into the remaining root end and seal it with a biocompatible material. This retrograde seal acts as an impenetrable barrier, preventing any remaining bacteria within the main canal from escaping into the bone, thereby allowing the body’s immune system to clear the existing lesion and regenerate healthy bone tissue.
Clinical Indications: When is Root End Surgery Necessary?
Root end surgery is clinically indicated when non-surgical root canal retreatment is unfeasible, contraindicated, or has previously failed to eradicate periapical pathology and restore tissue health.
The decision to proceed with an apicoectomy is never made lightly; it requires a comprehensive clinical and radiographic evaluation to ensure that surgical intervention is the most appropriate course of action. The primary indication for this procedure is the presence of persistent or refractory periapical periodontitis following a technically adequate root canal treatment. In many cases, if a root canal fails, the first line of defense is a non-surgical retreatment, where the dentist re-enters the tooth from the top, removes the old filling material, disinfects the canals again, and places a new seal. However, there are numerous clinical scenarios where non-surgical retreatment is either impossible or carries an unacceptably high risk of damaging the tooth.
One of the most common indications for an apicoectomy is the presence of complex restorative work. If a tooth has been restored with a large, well-fitting post and core foundation and a highly aesthetic ceramic crown, attempting to remove these restorations to access the root canal can easily lead to a catastrophic vertical root fracture, rendering the tooth unsalvageable. In such instances, approaching the infection surgically from the root end bypasses the coronal restorations entirely, preserving the expensive and functional crown. [2] Furthermore, anatomical challenges such as severely curved roots, calcified (blocked) canals, or the presence of separated endodontic instruments (broken files) lodged tightly in the apical third of the canal often make non-surgical negotiation impossible. Apical surgery allows the clinician to bypass these internal blockages and address the infection directly at its source.
“The decision to perform an apicoectomy hinges on a meticulous risk-benefit analysis. Preserving the natural tooth architecture is paramount, but the structural integrity of the remaining root and the surrounding periodontium must be sufficient to support long-term function and withstand the forces of mastication.” – Dr. Nguyen Van Cuong.
Another critical indication is the presence of an extraradicular infection. Sometimes, bacteria form a resilient biofilm on the outer surface of the root apex, or specific microorganisms like Actinomyces israelii establish colonies within the periapical tissues themselves. Because these bacteria are located outside the confines of the root canal system, no amount of internal cleaning and shaping will resolve the infection. Surgical curettage (scraping) of the infected bone and resection of the root tip is the only definitive way to physically remove these extraradicular biofilms. Additionally, true periapical cysts, particularly those with high cholesterol crystal content, often do not respond to non-surgical therapy and require surgical enucleation to initiate healing.
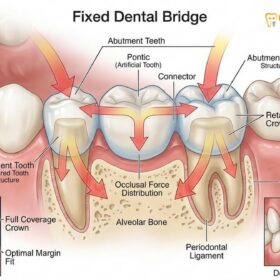
However, it is equally important to understand the contraindications for the procedure. An apicoectomy is not a panacea for all failing teeth. If a tooth has suffered a vertical root fracture, surgery will not save it; extraction is mandatory. Similarly, teeth with severe periodontal disease, characterized by extensive bone loss and significant mobility, are poor candidates for apical surgery, as the remaining bone support is insufficient to maintain the tooth long-term. In cases where the tooth cannot be saved, patients must consider extraction followed by prosthetic replacement, such as a dental implant or a fixed dental bridge, to restore the arch’s integrity and prevent the shifting of adjacent teeth.
Step-by-Step Clinical Workflow of an Apicoectomy
The surgical workflow involves precise flap design, osteotomy, root-end resection, ultrasonic preparation, and the placement of a biocompatible retrograde filling under high magnification.
The modern dental procedure apicoectomy is a highly refined microsurgical technique that relies heavily on advanced technology, specifically Cone-Beam Computed Tomography (CBCT) and the dental operating microscope. The workflow begins with a meticulous pre-operative assessment. A CBCT scan is considered the gold standard for surgical planning, providing a three-dimensional view of the tooth, the exact size and location of the periapical lesion, and its proximity to vital anatomical structures such as the maxillary sinus, the nasal floor, or the inferior alveolar nerve. This 3D mapping allows the surgeon to plan the exact surgical approach, minimizing risks and optimizing outcomes.
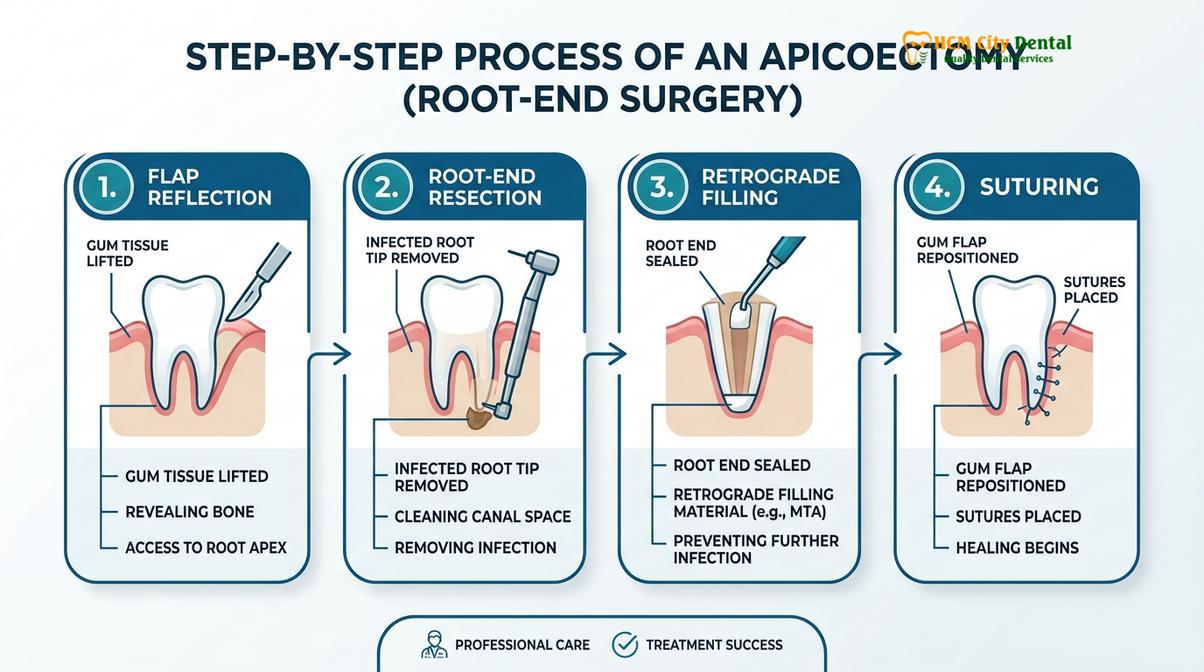
On the day of the surgery, the procedure commences with the administration of profound local anesthesia. The surgeon utilizes specialized anesthetic techniques, often incorporating a vasoconstrictor like epinephrine, not only to ensure the patient is completely pain-free but also to achieve excellent hemostasis (control of bleeding) at the surgical site. A blood-free surgical field is absolutely critical for the precise visualization required during microsurgery. Once the area is profoundly numb, the surgeon makes a precise incision in the gingival tissue (gums). The design of this incision—often a full-thickness mucoperiosteal flap—is carefully planned to preserve the aesthetic contours of the gums, particularly in the highly visible anterior (front) regions of the mouth.

Following the elevation of the gum tissue, the surgeon performs an osteotomy, which involves using a specialized surgical bur and copious sterile saline irrigation to create a small window in the cortical bone, thereby exposing the infected root apex. The infected periapical tissue, which often presents as a rubbery mass of inflammatory cells (granuloma) or a fluid-filled sac (cyst), is meticulously curetted (scraped) out of the bony crypt. This tissue is sometimes sent for histopathological examination to confirm the diagnosis. Once the root tip is clearly visible, the surgeon performs the root-end resection, removing approximately 3 millimeters of the apex at a shallow bevel (usually 0 to 10 degrees). This specific resection length is critical, as it eliminates the vast majority of the complex apical anatomy where bacteria hide. [3]
The next phase is the retrograde preparation. Using specialized, diamond-coated ultrasonic tips driven by high-frequency vibrations, the surgeon prepares a small, precise cavity into the resected root end, following the long axis of the canal to a depth of about 3 millimeters. Ultrasonic preparation is vastly superior to older methods using rotary burs, as it allows for better alignment, cleaner cavity walls, and a significantly reduced risk of micro-fracturing the root. After the cavity is cleaned and dried, a biocompatible retrograde filling material is placed. Modern endodontics heavily favors bioceramic materials, such as Mineral Trioxide Aggregate (MTA) or premixed bioceramic putty. These materials are hydrophilic (they set in the presence of moisture), highly biocompatible, and actually stimulate the surrounding bone cells (osteoblasts) to regenerate new bone directly against the filling material. [4]
Finally, the surgical site is thoroughly irrigated, and the gingival flap is carefully repositioned and sutured into place using fine, synthetic monofilament sutures. These sutures minimize plaque accumulation and promote rapid, aesthetic healing of the soft tissues. The entire procedure is performed under the intense illumination and high magnification (up to 25x) of a surgical microscope, ensuring that no anatomical detail is missed and the retrograde seal is absolutely perfect.
| Clinical Feature | Non-Surgical Retreatment | Surgical Apicoectomy |
|---|---|---|
| Access Approach | Coronal (through the top of the tooth crown) | Surgical (through the gums and alveolar bone) |
| Primary Indication | Incomplete initial cleaning, missed canals | Extraradicular infection, blocked canals, large posts |
| Impact on Restorations | Requires drilling through or removing existing crowns | Bypasses crowns entirely; preserves existing restorations |
| Healing Assessment | Radiographic evaluation over 6-12 months | Radiographic evaluation over 6-12 months |
| Procedural Complexity | Moderate to High (navigating internal anatomy) | High (requires microsurgical training and equipment) |
Post-Operative Care and Recovery Timeline
Post-operative recovery requires strict adherence to oral hygiene protocols, soft diet modifications, and prescribed medications to minimize swelling and prevent secondary infection.
The recovery period following an apicoectomy is generally smooth and manageable, provided the patient strictly adheres to the post-operative instructions provided by their dental surgeon. Because the procedure involves an incision in the soft tissue and the removal of a small amount of bone, a certain degree of inflammatory response is entirely normal and expected. Patients should anticipate mild to moderate localized swelling and potentially some ecchymosis (bruising) on the face near the surgical site. This swelling typically peaks between 48 and 72 hours post-surgery before gradually subsiding over the following week.
To minimize swelling, the immediate application of cold therapy is crucial. Patients are instructed to apply an ice pack to the outside of the face, alternating 20 minutes on and 20 minutes off, for the first 24 hours. After the initial 24-hour period, switching to warm, moist compresses can help increase local blood flow and accelerate the resolution of any bruising. Pain management is usually highly effective with over-the-counter non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen, which address both pain and inflammation. In some cases, the surgeon may prescribe a stronger analgesic for the first day or two, but severe pain is rarely a feature of apicoectomy recovery. If you are planning to book a dentist appointment online for a follow-up, it is typically scheduled 5 to 7 days post-op for suture removal and evaluation of soft tissue healing.
Warning: Immediate Clinical Attention Required
While complications are rare, you must monitor your healing closely. If you experience rapidly spreading facial swelling, difficulty swallowing or breathing, uncontrolled bleeding that does not stop with firm, continuous pressure, or a fever exceeding 101°F (38.3°C) following an apicoectomy, contact your emergency dental provider immediately. These symptoms may indicate a severe, spreading postoperative infection or a systemic complication that requires urgent medical intervention.
Dietary modifications are essential during the first few days of recovery. Patients must adhere to a soft diet, avoiding hard, crunchy, spicy, or excessively hot foods that could traumatize the surgical site or dislodge the sutures. Chewing should be directed to the opposite side of the mouth. Maintaining excellent oral hygiene is critical to prevent secondary infection, but it must be done gently. Patients should brush their remaining teeth normally but avoid brushing directly over the surgical incision. Instead, a prescribed antimicrobial mouthrinse (such as chlorhexidine gluconate) or warm salt water rinses should be used to keep the surgical area clean without causing mechanical trauma.

Antibiotics are not universally prescribed following an apicoectomy. The decision to prescribe antibiotics is based on clinical diagnostics, the extent of the pre-existing infection, and the patient’s medical history. If antibiotics are prescribed, it is imperative to complete the entire course exactly as directed, even if symptoms improve rapidly. Smoking and the use of tobacco products must be strictly avoided during the healing phase, as the toxins in smoke severely impair blood flow to the gingival tissues, significantly increasing the risk of delayed healing, wound breakdown, and surgical failure.
Success Rates and Long-Term Prognosis
Modern endodontic microsurgery boasts a high success rate, often exceeding 90%, heavily dependent on the quality of the retrograde seal and the patient’s overall periodontal health.
The long-term prognosis for a tooth that has undergone a properly executed apicoectomy is exceptionally favorable. Historically, apical surgery was considered a procedure of last resort with variable outcomes, largely due to the use of macroscopic techniques and inferior filling materials like amalgam. However, the advent of endodontic microsurgery—characterized by the use of surgical microscopes, ultrasonic preparation, and biocompatible materials—has revolutionized the predictability of the procedure. Current clinical literature indicates that the success rate of modern endodontic microsurgery ranges from 85% to over 94%, making it a highly reliable method for preserving the natural dentition. [5]
The definition of “success” in apical surgery is based on both clinical and radiographic criteria. Clinically, the patient must be completely asymptomatic, with no pain, swelling, sinus tracts, or mobility. Radiographically, follow-up X-rays or CBCT scans taken at 6-month and 12-month intervals must demonstrate the regeneration of healthy bone filling the surgical crypt and the re-establishment of a normal periodontal ligament space around the resected root tip. The remarkable biocompatibility of materials like MTA allows for cementogenesis—the deposition of new cementum directly over the filling material—which is the ultimate histological marker of true biological healing.
Clinical Case Study: Apical Healing at HCMC Dental Clinic
A 45-year-old patient presented to our facility in Ho Chi Minh City with a persistent sinus tract (gum boil) and localized swelling over the upper right lateral incisor. The tooth had a previous root canal and a newly placed, highly aesthetic ceramic crown. A CBCT scan revealed a 5mm periapical radiolucency indicating chronic infection. To avoid destroying the new crown, Dr. Cuong performed an apicoectomy using a surgical microscope and an MTA retrograde filling. At the 6-month follow-up, radiographic imaging demonstrated complete osseous regeneration (bone healing) around the root apex, and the patient remained entirely asymptomatic, successfully preserving both the natural root and the prosthetic crown.
Several factors influence the long-term success of the procedure. The most critical factor is the quality of the coronal seal. Even if the surgical root-end filling is perfect, if the crown or filling on the top of the tooth is leaking, bacteria from the saliva will eventually migrate down the canal and re-infect the periapical tissues. Therefore, ensuring that the tooth has a well-fitting, permanent restoration is paramount. Additionally, the patient’s overall periodontal health plays a significant role. A tooth must have adequate bone support along the sides of its root to remain functional. If you are wondering how many teeth adults have that can be saved this way, the answer encompasses almost any tooth in the arch, provided the surgical access is safe and the periodontal foundation is sound.
“The integration of cone-beam computed tomography (CBCT) and high-powered surgical microscopes has transformed the dental procedure apicoectomy from a blind surgical approach into a highly predictable, microsurgical art, allowing us to save teeth that were previously deemed hopeless.” – Journal of Endodontics.
When to See a Doctor: Identifying Endodontic Failure
Patient vigilance is a critical component of long-term dental health, particularly for teeth that have undergone previous endodontic therapy. Recognizing the early signs of a failing root canal can mean the difference between saving the tooth with a relatively straightforward apicoectomy and losing the tooth entirely to extraction. Because the nerve of the tooth has been removed during the initial root canal, the tooth itself cannot feel hot or cold. Therefore, the symptoms of endodontic failure arise from the surrounding tissues—the bone and the periodontal ligament—which are rich in nerve endings.
One of the most common signs of a persistent periapical infection is pain upon mastication (chewing) or when tapping on the tooth. This occurs because the inflammation at the root tip increases the pressure within the confined bony socket, making the tooth exquisitely sensitive to mechanical loading. Patients may also experience a dull, continuous ache in the jaw that radiates to surrounding areas. Another hallmark sign is the development of localized swelling on the gingiva near the root apex. This swelling may present as a small, pimple-like bump known as a sinus tract or fistula. This tract acts as a pressure release valve, allowing purulent exudate (pus) to drain from the infected bone into the mouth, often resulting in a foul taste or odor.
If you experience any of these symptoms, it is imperative to seek professional evaluation without delay. Finding the nearest dentist to me who is equipped with advanced diagnostic tools like CBCT is crucial for an accurate assessment. Ignoring these signs can lead to the silent expansion of the periapical lesion, resulting in extensive destruction of the jawbone, potential involvement of adjacent healthy teeth, or the spread of infection into the fascial spaces of the head and neck. Early intervention maximizes the chances of a successful surgical outcome. Establishing a routine of regular dental check-ups, a habit that should begin early according to pediatric dental guidelines, ensures that any asymptomatic radiographic changes are detected and addressed long before they develop into acute clinical emergencies.
Frequently Asked Questions
Is the dental procedure apicoectomy painful?
No, the procedure is performed under profound local anesthesia, ensuring you feel no pain during the surgery. Post-operative discomfort is typically mild to moderate and can be effectively managed with over-the-counter non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen. The surgical site may feel tender for a few days, but severe pain is highly uncommon and should be reported to your dentist immediately.
How long does an apicoectomy procedure take?
An apicoectomy generally takes between 45 to 90 minutes to complete. The exact duration depends on the anatomical location of the tooth, the complexity of the root structure, and the extent of the periapical infection being treated. Anterior (front) teeth are typically faster to treat than posterior (back) molars, which have multiple roots and thicker overlying bone.
What is the alternative to an apicoectomy?
The primary alternative to an apicoectomy is the complete extraction of the affected tooth. Following extraction, the missing tooth is typically replaced with a dental implant, a fixed dental bridge, or a removable partial denture to restore function and prevent adjacent teeth from shifting. However, preserving the natural tooth through surgery is generally the preferred and more conservative approach.
Can an apicoectomy fail?
While success rates are highly favorable, an apicoectomy can fail if the retrograde seal is inadequate, if the tooth has an undetected vertical root fracture, or if severe periodontal disease compromises the supporting bone structure around the tooth. If an apicoectomy fails, the tooth usually must be extracted, as repeated surgical interventions on the same root apex have significantly lower success rates.
How much does an apicoectomy cost?
The cost of an apicoectomy varies based on the tooth’s location, the complexity of the surgery, and the geographic region of the clinic. According to the latest clinic fee schedules, it is generally more cost-effective than extracting the tooth and placing a dental implant. Many dental insurance plans provide partial coverage for endodontic surgery, so it is advisable to consult with your provider and the clinic’s financial coordinator.
References
- Journal of Endodontics. Modern endodontic surgery concepts and practice: a review. (2021).
- International Endodontic Journal. Outcome of endodontic surgery: a meta-analysis of the literature. (2020).
- Journal of the American Dental Association. Bioceramic materials in endodontic microsurgery. (2019).
- Clinical Oral Investigations. Healing of periapical lesions following root-end surgery. (2022).
- Oral Surgery, Oral Medicine, Oral Pathology. Cone-beam computed tomography in endodontic treatment planning. (2018).