The American Academy of Pediatric Dentistry and global pediatric experts recommend that a child’s first dentist visit should occur within six months of the eruption of their first primary tooth, and no later than their first birthday. This early intervention establishes a vital foundation for lifelong oral health and helps prevent complex dental issues in the future.
Clinical Summary:
Determining when the first dentist visit should take place is a critical milestone in pediatric healthcare. Clinical consensus mandates that infants undergo their initial oral examination by age one, or shortly after the emergence of the first deciduous tooth. This proactive approach is designed to combat Early Childhood Caries (ECC), assess craniofacial development, and establish a “Dental Home” for the child. During this foundational visit, clinicians utilize a knee-to-knee examination technique to safely evaluate the oral cavity, apply preventive fluoride varnish, and provide parents with essential anticipatory guidance regarding diet, teething, and oral hygiene. Early establishment of professional dental care significantly reduces the risk of future complex pathologies and fosters a positive, anxiety-free relationship between the child and their dental provider.
Key Takeaways:
- The first dental visit should occur by age one or within six months of the first tooth erupting.
- Early examinations are crucial for detecting and preventing Early Childhood Caries (ECC).
- Clinicians use a secure knee-to-knee technique to examine infants safely and comfortably.
- Anticipatory guidance provided during the visit covers teething, diet, and oral hygiene practices.
- Establishing a Dental Home early helps reduce dental anxiety and long-term emergency care costs.
The Clinical Timeline: When Should the First Dentist Visit Occur?
Clinical guidelines dictate that an infant’s initial dental examination must be scheduled by age one or shortly after the first tooth emerges to help prevent early childhood caries.
The question of when the first dentist visit should occur is one of the most common inquiries fielded by pediatric dental professionals. Historically, many parents and even some medical practitioners believed that dental visits were unnecessary until a child had a complete set of primary teeth. However, modern evidence-based dentistry has fundamentally shifted this paradigm. The current, universally accepted standard established by leading pediatric health organizations is the “Age 1” rule. A child should be seen by a dentist within six months of the eruption of their first primary tooth (deciduous tooth), and absolutely no later than their first birthday[1].
The eruption of the first tooth, typically a mandibular central incisor, usually occurs between six and ten months of age. The moment this tooth breaches the gingival tissue and enters the oral cavity, it becomes susceptible to bacterial colonization and demineralization. The enamel of primary teeth is significantly thinner and less mineralized than that of permanent teeth, making it highly vulnerable to rapid decay. By adhering to the age one timeline, clinicians can intervene before any carious lesions have the opportunity to develop, shifting the focus of pediatric dentistry from surgical restoration to proactive prevention.

Integrating this early visit into a child’s overall healthcare routine is a cornerstone of comprehensive pediatric care. It aligns dental care with other critical pediatric milestones, such as well-baby medical checkups and immunizations. Delaying the first visit until age two or three drastically increases the statistical probability of the child presenting with established dental disease, which often requires invasive treatments that can induce severe dental anxiety and require pharmacological sedation.
Medical Reasoning Behind Early Infant Oral Examinations
Early dental visits allow clinicians to assess craniofacial development, detect early demineralization, and provide anticipatory guidance before irreversible dental pathologies develop.
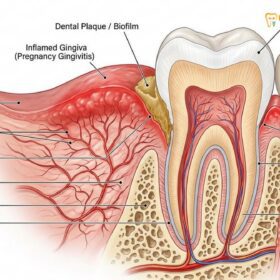
The primary medical rationale for an early first dentist visit is the prevention and management of Early Childhood Caries (ECC). ECC is a virulent, rapidly progressing form of tooth decay that affects infants and toddlers. It is an infectious disease primarily driven by the transmission of cariogenic bacteria, notably Streptococcus mutans, typically passed from the primary caregiver to the infant through saliva-sharing behaviors. Once these bacteria colonize the infant’s oral cavity, they metabolize fermentable carbohydrates from milk, formula, or juice, producing lactic acid that rapidly decalcifies the fragile primary enamel[2].
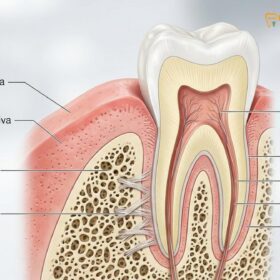
In addition to global standards, the Vietnam Ministry of Health (MOH) strongly advocates for early oral health screenings to combat the high prevalence of ECC in Southeast Asia, emphasizing that preventive care must begin as soon as the first tooth appears[3]. Beyond caries detection, the age one visit serves as a comprehensive evaluation of the infant’s overall oral and craniofacial development. Clinicians meticulously examine the soft tissues, including the gingiva, buccal mucosa, and palate. A critical component of this assessment is the evaluation of the frenulum attachments. Ankyloglossia, commonly known as tongue-tie, or a restrictive maxillary labial frenulum (lip-tie), can severely impact an infant’s ability to latch during breastfeeding, affect swallowing patterns, and eventually impede speech development.
“The establishment of a Dental Home by age one is not merely about inspecting teeth; it is a comprehensive strategy to integrate oral health into the child’s systemic well-being, providing a continuous, accessible, and family-centered foundation for lifelong preventive care.”
According to Dr. Nguyen Van Cuong, a leading specialist at HCMC Dental Clinic, early screening is not just about checking for cavities; it is a comprehensive evaluation of the child’s airway, swallowing patterns, and jaw development. Identifying early signs of malocclusion or developmental anomalies allows the dental team to monitor growth trajectories closely. This proactive monitoring is an essential component of General Dentistry tại HCMC Dental Clinic, as minor developmental issues can often be guided or corrected with minimal intervention if caught early.
Clinical Workflow: What Happens During the First Appointment?
The initial visit utilizes a knee-to-knee examination technique to safely evaluate the infant’s oral cavity, followed by gentle prophylaxis and targeted fluoride application.
Understanding the clinical workflow of the first dentist visit helps alleviate parental anxiety and sets clear expectations. Unlike an adult dental appointment, an infant exam does not involve sitting in a large dental chair for an extended period. Instead, pediatric dentists utilize a highly effective, specialized positioning method known as the knee-to-knee (or lap-to-lap) examination technique. This approach maximizes the child’s comfort while providing the clinician with optimal visibility and control[5].
In the knee-to-knee position, the parent and the dentist sit facing each other, with their knees touching to form a stable “table.” The infant is positioned facing the parent, straddling the parent’s waist. The parent then gently lays the child backward so that the child’s head rests securely in the dentist’s lap. The parent holds the child’s hands and provides soothing verbal reassurance, while the dentist has a clear, well-illuminated view of the oral cavity. It is entirely normal and expected for the infant to cry during this process. Clinically, a crying child actually facilitates the examination, as the open mouth allows for a thorough and rapid visual inspection of all oral structures.

During the examination, the dentist will use a soft, disposable dental mirror and perhaps a soft-bristled infant toothbrush to gently remove any plaque biofilm and inspect the erupting teeth. They will assess the enamel for white spot lesions (the earliest clinical sign of demineralization), check the health of the gingival tissues, and evaluate the eruption pattern. Following the visual and tactile assessment, the clinician will typically perform a gentle prophylaxis (cleaning) using a soft brush. Finally, a 5% sodium fluoride varnish is applied to the erupted teeth. Fluoride varnish is the gold standard in pediatric preventive dentistry; it adheres rapidly to the enamel in the presence of saliva, providing a sustained release of fluoride ions that remineralize microscopic defects.
| Age / Milestone | Clinical Focus | Preventive Action Taken |
|---|---|---|
| Birth to 6 Months (Pre-eruption) | Soft tissue health, feeding mechanics | Parental education on gum wiping, frenulum assessment |
| 6 to 12 Months (First Tooth Erupts) | Enamel integrity, early colonization | Knee-to-knee exam, first fluoride varnish application |
| 12 to 18 Months | Dietary habits, plaque accumulation | Caries risk assessment, oral hygiene instruction refinement |
| 18 to 24 Months | Primary molar eruption, occlusion | Monitoring for early childhood caries, assessing bite alignment |
Establishing these clinical routines early not only protects the primary dentition but also sets the stage for future oral health practices. For instance, children who are accustomed to professional cleanings and fluoride treatments from infancy are much more compliant with advanced hygiene protocols later in life, such as learning how to keep teeth white with braces during adolescent orthodontic treatment.
Anticipatory Guidance and Parental Education
Clinicians provide evidence-based counseling on proper infant feeding practices, teething management, and the cessation of non-nutritive sucking habits to ensure optimal oral development.
A significant portion of the first dentist visit is dedicated to anticipatory guidance. This is a proactive counseling process where the dentist educates parents on what to expect in the coming months regarding their child’s oral development and how to prevent disease before it starts. Because infants are entirely dependent on their caregivers for oral hygiene and dietary choices, empowering parents with evidence-based knowledge is the most effective preventive tool in pediatric dentistry[4].
Dietary counseling is paramount. The clinician will discuss the severe risks associated with Baby Bottle Tooth Decay (BBTD). Parents are strongly advised against putting a child to bed with a bottle containing milk, formula, juice, or any sweetened liquid. During sleep, salivary flow decreases significantly, reducing the mouth’s natural ability to buffer acids and wash away sugars. If a child falls asleep with a bottle, the cariogenic liquids pool around the maxillary anterior teeth, leading to rapid and devastating decay. Dentists recommend transitioning from a bottle to a free-flowing cup by the child’s first birthday to mitigate this risk.
Another critical topic of anticipatory guidance is the management of non-nutritive sucking habits, such as pacifier use and thumb sucking. While these habits are normal and self-soothing for infants, prolonged use beyond the age of two or three can exert detrimental biomechanical forces on the developing maxilla and mandible. Chronic thumb sucking can lead to a high palatal vault, posterior crossbites, and severe anterior open bites. Educating parents early allows for gentle, gradual weaning strategies, preventing the need for complex corrective treatments later in life, such as buck teeth braces to correct severe overjets caused by prolonged digit sucking.
Preparing the Child and Parent for Dental Success
Successful pediatric dental visits rely on proactive parental preparation, utilizing positive reinforcement and familiarization techniques to minimize dental anxiety.
The success of the first dentist visit is heavily influenced by how well the parents prepare themselves and their child prior to the appointment. Children are highly perceptive and can easily absorb their parents’ anxieties. Therefore, the first step in preparation is for parents to manage their own dental fears and approach the visit with a calm, positive, and enthusiastic demeanor. Using positive language is crucial; parents should avoid using words with negative connotations, such as “pain,” “hurt,” “drill,” or “shot,” even in a reassuring context.
Desensitization at home is a highly effective strategy. Parents can play “dentist” with their child, taking turns looking into each other’s mouths with a flashlight and counting teeth. Reading age-appropriate children’s books or watching positive videos about visiting the dentist can also help familiarize the child with the clinical environment. Scheduling the appointment during the morning hours, when the child is typically well-rested and most cooperative, significantly improves the likelihood of a smooth visit.
Clinical Case Study: Early Intervention at HCMC Dental Clinic
A 14-month-old patient presented at HCMC Dental Clinic in Ho Chi Minh City for a slightly delayed first dental visit. The parents reported no visible issues but wanted a routine check. During the knee-to-knee examination, the clinical team identified early white spot lesions (demineralization) along the gingival margin of the maxillary central incisors. Through detailed dietary analysis, it was discovered the child was frequently nursing throughout the night. The dentist applied a targeted 5% fluoride varnish and provided specific anticipatory guidance on nighttime feeding and oral hygiene. At the 3-month follow-up, the lesions had successfully remineralized, halting the progression of decay and preventing the need for future restorative intervention.
Building a trusting relationship between the child, the parent, and the dental team from infancy pays lifelong dividends. Children who establish a Dental Home early view routine dental care as a normal part of life rather than a punitive or frightening event. This foundation of trust is invaluable when the child grows older and may require more involved procedures. A patient who is comfortable in the dental chair is much better equipped to handle future decisions, such as evaluating wisdom teeth removal: hospital or dentist settings, without the burden of deep-seated dental phobia.
When to See a Doctor: Urgent Pediatric Dental Care
While routine visits begin at age one, certain acute conditions such as dental trauma, severe bleeding, or visible signs of infection require immediate clinical evaluation.
Although the standard recommendation for the first dentist visit is by the first birthday, parents must remain vigilant for signs that necessitate urgent care prior to this milestone. Dental trauma is one of the most common reasons for an emergency pediatric visit. As infants learn to crawl, pull themselves up, and walk, falls are inevitable. If a child sustains a blow to the mouth resulting in a chipped tooth, a tooth being pushed into the gum (intrusion), or a tooth being knocked out entirely (avulsion), immediate professional assessment is required to evaluate potential damage to the developing permanent tooth buds beneath the gums.
“Parents should never delay seeking professional care if they observe signs of acute oral pathology; early intervention in cases of trauma or infection is critical to preserving the integrity of both the primary and developing permanent dentition.”
Additionally, parents should inspect their child’s mouth regularly during daily hygiene routines. If dark spots, chalky white bands near the gumline, or visible cavities appear on the teeth, an appointment should be scheduled immediately, regardless of the child’s age. Swelling of the gums, face, or lips, accompanied by a fever or difficulty swallowing, can indicate a severe dental infection or abscess, which constitutes a medical emergency requiring prompt antibiotic therapy and clinical management.

References
- American Academy of Pediatric Dentistry. Policy on the Dental Home. (2021).
- Journal of the American Dental Association. Evidence-based clinical practice guideline on nonrestorative treatments for carious lesions. (2018).
- Vietnam Ministry of Health (MOH). National Guidelines on Pediatric Oral Health and Early Childhood Caries Prevention. (2022).
- International Journal of Paediatric Dentistry. Anticipatory guidance and infant oral health care. (2019).
- Journal of Clinical Pediatric Dentistry. The efficacy of the knee-to-knee examination technique in infants. (2022).