

Bad breath during pregnancy, clinically known as halitosis, is primarily caused by hormonal fluctuations, morning sickness, and decreased salivary flow. These physiological changes alter the oral microbiome, increasing plaque accumulation and volatile sulfur compounds. Fortunately, this condition is highly manageable with targeted oral hygiene and professional dental care.
Clinical Summary:
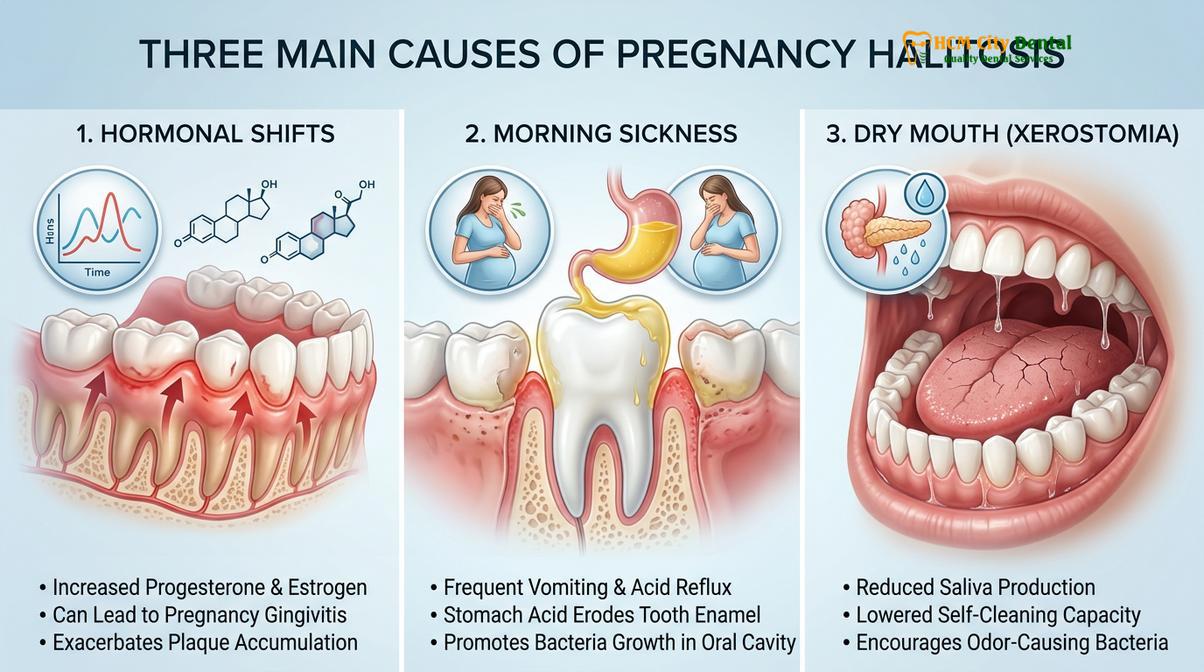
During gestation, the maternal body undergoes profound systemic changes that directly impact the oral cavity. Elevated levels of estrogen and progesterone exaggerate the gingival response to dental plaque, frequently resulting in pregnancy gingivitis—a primary contributor to oral malodor. Furthermore, hyperemesis gravidarum (morning sickness) introduces harsh gastric acids into the mouth, lowering the resting pH and creating an optimal environment for anaerobic, odor-producing bacteria. Reduced salivary flow, often exacerbated by frequent urination and altered hydration levels, further diminishes the mouth’s natural self-cleansing mechanisms. Managing this condition requires a multifaceted clinical approach, including optimized home-care routines, pH-neutralizing strategies, and routine professional prophylaxis. Expectant mothers are strongly encouraged to maintain regular dental visits, as untreated periodontal inflammation is not only a source of persistent halitosis but has also been linked in clinical literature to broader systemic pregnancy complications.
Key Takeaways:
- Hormonal surges (estrogen and progesterone) increase gingival vascularity, making gums more susceptible to plaque-induced inflammation and odor.
- Gastric acids from morning sickness lower oral pH, accelerating enamel demineralization and fostering anaerobic bacterial growth.
- Pregnancy-induced xerostomia (dry mouth) reduces the buffering and cleansing capacity of saliva, concentrating volatile sulfur compounds.
- Professional dental cleanings are entirely safe during pregnancy and are critical for managing pregnancy gingivitis.
- Immediate brushing after vomiting is contraindicated; patients should neutralize acids with a baking soda rinse first to protect enamel.
The Clinical Pathophysiology of Bad Breath During Pregnancy
Hormonal surges and physiological changes during gestation directly alter the oral environment, promoting the proliferation of anaerobic bacteria responsible for persistent halitosis.
To effectively manage bad breath during pregnancy, it is essential to understand the complex biochemical and physiological transformations occurring within the maternal body. The oral cavity is not isolated from systemic changes; rather, it acts as a highly sensitive mirror reflecting the profound hormonal shifts of gestation. When a patient experiences a sudden onset of halitosis during pregnancy, it is rarely due to a sudden decline in brushing habits. Instead, it is typically the result of an altered oral microbiome driven by endocrine fluctuations, gastrointestinal disturbances, and changes in salivary gland function. Understanding these mechanisms is a cornerstone of general dentistry services focused on maternal care.
Hormonal Shifts and the Gingival Response
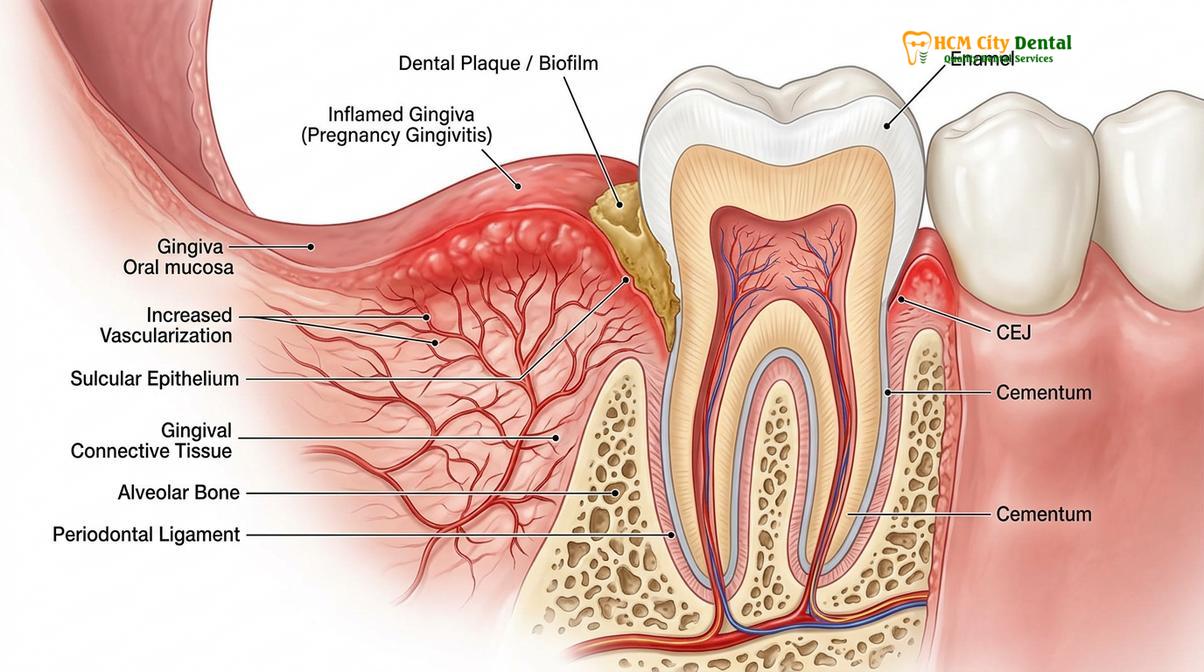
From the first trimester onward, the placenta produces massive quantities of estrogen and progesterone to support fetal development. While essential for the pregnancy, these hormones have a profound secondary effect on the periodontium. Progesterone, in particular, increases the permeability of the gingival microvasculature. This means that the blood vessels in the gums become slightly more “leaky,” allowing inflammatory mediators to flood the tissue in response to even minute amounts of dental plaque. Furthermore, certain anaerobic bacteria—specifically Prevotella intermedia—can actually utilize progesterone as a nutrient source, leading to a massive overgrowth of this specific pathogen in the subgingival biofilm [1]. As these bacteria metabolize proteins, they release Volatile Sulfur Compounds (VSCs) such as hydrogen sulfide and methyl mercaptan, which are the primary chemical agents responsible for the foul odor associated with halitosis.
Hyperemesis Gravidarum and Oral Acidification
Morning sickness, clinically termed hyperemesis gravidarum in its severe form, is another major catalyst for pregnancy-induced bad breath. The resting pH of a healthy oral cavity is typically neutral, hovering between 6.2 and 7.6. Gastric acid, however, is highly corrosive, with a pH ranging from 1.5 to 3.5. When a pregnant woman vomits, the oral cavity is flooded with this hydrochloric acid. This sudden drop in pH overwhelms the natural buffering capacity of saliva. An acidic environment not only causes immediate demineralization of the hydroxyapatite crystals in tooth enamel but also creates an ecological shift in the oral microbiome. Aciduric (acid-loving) bacteria thrive, while beneficial bacteria perish. The combination of partially digested food particles, gastric acid, and a rapid shift in bacterial flora produces a distinct, highly unpleasant malodor that is difficult to eradicate with standard brushing alone.
Pregnancy-Induced Xerostomia (Dry Mouth)
Saliva is the mouth’s most critical defense mechanism against halitosis. It contains mucins that sweep away food debris, as well as antimicrobial enzymes like lysozyme, lactoferrin, and secretory immunoglobulin A (IgA) that actively suppress bacterial overgrowth. During pregnancy, several factors contribute to a reduction in salivary flow, a condition known as xerostomia. Increased metabolic demands, frequent urination, and the expansion of maternal blood volume can lead to mild systemic dehydration if fluid intake is not proportionally increased. Additionally, hormonal changes can directly alter the composition and flow rate of the salivary glands. When the mouth is dry, the self-cleansing mechanism fails. Dead mucosal cells, food remnants, and bacteria stagnate on the posterior third of the tongue and along the gumline, putrefying and releasing concentrated sulfur gases [2].
Diagnostic Evaluation and Periodontal Implications
Persistent halitosis often serves as an early clinical indicator of pregnancy gingivitis or underlying periodontal disease, requiring prompt diagnostic evaluation to prevent systemic complications.
When an expectant mother presents with complaints of severe bad breath, a comprehensive clinical evaluation is mandatory. Halitosis is rarely an isolated symptom; it is frequently the most noticeable manifestation of underlying periodontal inflammation. According to clinical data, pregnancy gingivitis affects between 60% to 75% of all pregnant women. If left unmanaged, this localized inflammation can progress into more severe forms of periodontal disease, which carry significant implications not only for the mother’s dentition but potentially for the developing fetus.

Identifying Pregnancy Gingivitis and Pyogenic Granulomas
During a clinical examination, a dentist will look for classic signs of pregnancy gingivitis: erythema (redness), edema (swelling), and a tendency for the gums to bleed upon gentle probing. The presence of blood in the oral cavity further exacerbates bad breath, as the iron-rich heme molecules in blood are rapidly broken down by bacteria into foul-smelling compounds. In some cases, the exaggerated inflammatory response leads to the formation of a pyogenic granuloma, commonly referred to as a “pregnancy tumor.” Despite the alarming name, this is a benign, highly vascular, localized overgrowth of gingival tissue, usually located between the teeth. These lesions trap massive amounts of plaque and food debris, making them localized epicenters for halitosis production.
“Expectant mothers must understand that bleeding gums and persistent malodor are not merely cosmetic issues; they are clinical signs of active inflammation that demand professional attention to safeguard both maternal and fetal health,” notes Dr. Nguyen Van Cuong.
The Systemic Link: Periodontal Health and Pregnancy Outcomes
The medical community has increasingly recognized the bidirectional relationship between oral health and systemic well-being. The bacteria responsible for severe halitosis and periodontitis do not remain confined to the oral cavity. The inflamed, highly vascularized gingival tissues provide a direct portal of entry for these pathogens and their endotoxins into the maternal bloodstream. Once in systemic circulation, these inflammatory markers—such as Prostaglandin E2 (PGE2) and Tumor Necrosis Factor-alpha (TNF-α)—can potentially cross the placental barrier. Elevated levels of these specific cytokines are biologically associated with the initiation of uterine contractions and cervical dilation. Consequently, severe, untreated periodontal disease has been investigated in numerous clinical studies as a potential risk factor for adverse pregnancy outcomes, including low birth weight and premature birth [3]. Therefore, treating the root cause of the bad breath is a critical component of comprehensive prenatal care.
| Etiological Factor | Clinical Manifestation | Recommended Dental Intervention |
|---|---|---|
| Hormonal Surges (Progesterone) | Erythematous, edematous gums; bleeding on brushing; elevated VSC production. | Professional ultrasonic scaling; optimized home plaque control; antimicrobial rinses. |
| Hyperemesis Gravidarum | Acidic malodor; enamel erosion on lingual surfaces; dentinal hypersensitivity. | Baking soda neutralization rinses; delayed brushing; fluoride varnish application. |
| Xerostomia (Dry Mouth) | Thick, ropy saliva; coated tongue; stagnant food debris; concentrated odor. | Increased hydration; xylitol-based salivary stimulants; mechanical tongue scraping. |
| Pyogenic Granuloma | Localized, red, nodular gingival overgrowth trapping plaque and debris. | Conservative debridement; surgical excision postpartum if it does not spontaneously regress. |
To ensure that all aspects of oral health are maintained during this critical period, patients should familiarize themselves with comprehensive oral hygiene steps that are specifically adapted for the unique challenges of pregnancy.
Evidence-Based Treatment Workflows for Expectant Mothers
Managing malodor during gestation involves a combination of professional prophylaxis, optimized home care, and pH-balancing strategies tailored strictly for maternal and fetal safety.
The management of bad breath during pregnancy requires a highly customized approach. Dental professionals must balance the urgent need to reduce bacterial loads and inflammation with the paramount requirement of ensuring fetal safety. Fortunately, modern dental protocols have established clear, evidence-based guidelines for treating pregnant patients across all three trimesters. The goal is to disrupt the biofilm, neutralize the oral environment, and empower the patient with effective home-care strategies.
Trimester-Specific Professional Care
While emergency dental care can and should be performed at any time during pregnancy to relieve pain or severe infection, routine professional prophylaxis (teeth cleaning) is generally optimized based on the trimester. The first trimester is a period of critical fetal organogenesis; therefore, elective procedures are often deferred, though a basic examination and hygiene instruction are highly beneficial. The second trimester is universally considered the safest and most comfortable time for professional dental interventions. During this phase, the risk of nausea has typically subsided, and the uterus is not yet large enough to cause supine hypotensive syndrome when the patient lies back in the dental chair. A thorough ultrasonic scaling performed during the second trimester is one of the most effective ways to eliminate the hardened calculus and subgingival plaque that drive pregnancy gingivitis and halitosis [4]. Patients often wonder about the frequency of professional teeth cleaning; during pregnancy, a higher frequency (e.g., every 3-4 months) may be clinically justified to manage aggressive plaque accumulation.
Clinical Case Study: Managing Pregnancy Halitosis
A 28-year-old patient in her second trimester visited HCMC Dental Clinic in Ho Chi Minh City complaining of severe morning breath, a metallic taste, and gums that bled profusely during brushing. Clinical examination revealed generalized moderate pregnancy gingivitis and a heavily coated posterior tongue. The treatment protocol included a gentle but thorough full-mouth ultrasonic debridement to remove subgingival calculus, followed by personalized instruction on the Modified Bass brushing technique and tongue scraping. The patient was prescribed an alcohol-free, chlorhexidine-based mouthrinse for short-term use to rapidly reduce the bacterial load. Within two weeks, the gingival bleeding ceased entirely, and the patient reported a complete resolution of the halitosis, significantly improving her quality of life during the remainder of her pregnancy.
Optimizing Home-Care Protocols
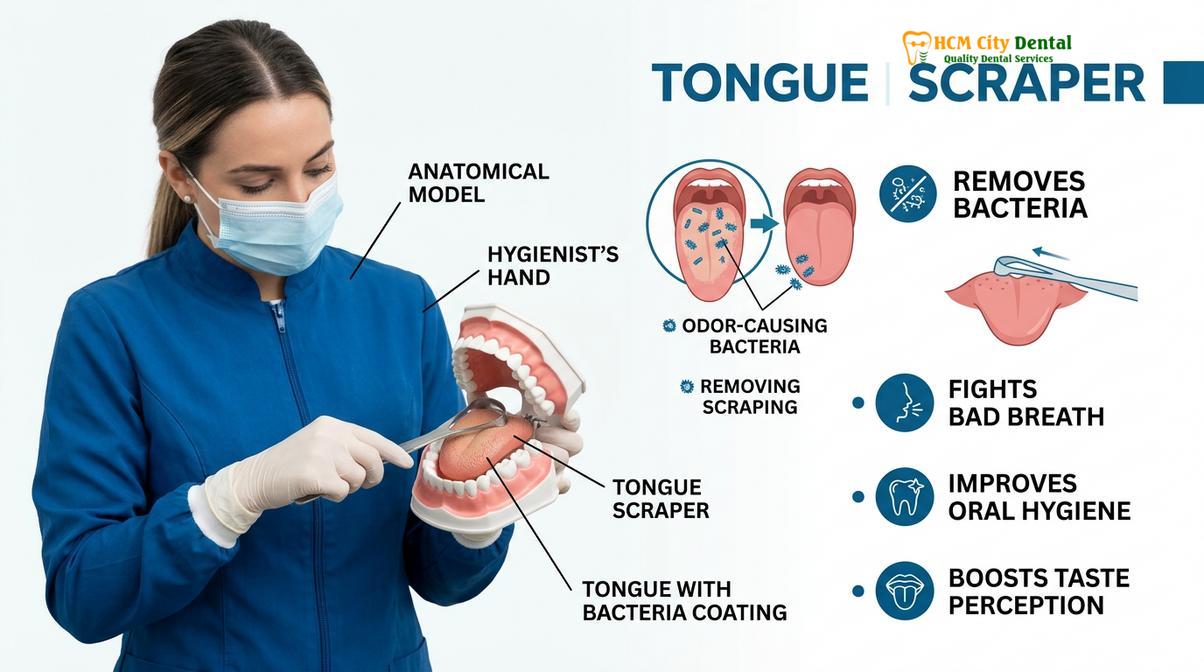
Professional cleanings must be supported by meticulous daily maintenance. Pregnant patients are advised to upgrade their home-care routines to combat the increased bacterial aggressiveness. This includes utilizing a soft-bristled toothbrush and employing the Modified Bass technique, which angles the bristles at 45 degrees toward the gumline to sweep out subgingival plaque without traumatizing the delicate, swollen tissues. Interdental cleaning—whether via traditional floss or water flossers—is non-negotiable, as the interproximal spaces are the primary breeding grounds for odor-causing anaerobes. Furthermore, mechanical tongue scraping is essential. The filiform papillae on the dorsal surface of the tongue act like a deep-pile carpet, trapping dead cells, food, and bacteria. A dedicated tongue scraper is far more effective than a toothbrush at removing this biofilm and instantly reducing VSC levels. For a detailed breakdown of these techniques, patients can review optimal oral hygiene routines.
Acid Neutralization Strategies
For women suffering from morning sickness, traditional brushing immediately after vomiting is strictly contraindicated. The gastric acids soften the enamel, and the abrasive action of a toothbrush will physically scrub away this weakened tooth structure, leading to permanent erosion and sensitivity. Instead, the immediate clinical recommendation is to vigorously rinse the mouth with a neutralizing solution. A highly effective, safe, and accessible home remedy is mixing one teaspoon of baking soda (sodium bicarbonate) into eight ounces of water. Swishing with this alkaline solution instantly neutralizes the hydrochloric acid, raises the oral pH back to a safe level, and neutralizes the acidic malodor. Patients should wait a minimum of 30 to 45 minutes after vomiting before attempting to brush their teeth with fluoride toothpaste.
Nutritional and Lifestyle Modifications for Halitosis Management
Dietary adjustments, adequate hydration, and targeted mineral supplementation play a critical role in stabilizing oral pH and reducing odor-causing bacterial loads.
Beyond mechanical cleaning, the biochemical environment of the mouth is heavily influenced by maternal diet and hydration. Pregnancy is famous for inducing intense dietary cravings, which often skew toward highly fermentable carbohydrates and sugars. While indulging these cravings is a normal part of the gestational experience, understanding their impact on oral health is vital for controlling bad breath.
Hydration and Salivary Stimulation
Combating pregnancy-induced xerostomia requires a proactive approach to hydration. Expectant mothers should aim to sip water continuously throughout the day rather than consuming large volumes infrequently. This constant moisture helps dilute bacterial byproducts and flush away food debris. To actively stimulate the salivary glands, chewing sugar-free gum containing xylitol is highly recommended. Xylitol is a naturally occurring sugar alcohol that cannot be metabolized by cavity-causing bacteria. Not only does the mechanical act of chewing stimulate salivary flow, but the xylitol itself actively inhibits the growth of Streptococcus mutans, thereby reducing both the risk of decay and the severity of halitosis.
“Dietary cravings often lead to an increased frequency of carbohydrate consumption, which rapidly accelerates plaque formation and volatile sulfur compound production if not meticulously managed through immediate oral rinsing,” explains a senior clinical hygienist.
Managing Cravings and Dietary Impact
When cravings strike, the type of food consumed dictates the resulting oral environment. Sticky, sugary snacks adhere to the teeth and provide an immediate fuel source for anaerobic bacteria, leading to a rapid spike in acid and odor production. Whenever possible, patients should try to substitute sugary snacks with crunchy, water-rich fruits and vegetables, such as apples, celery, and carrots. These foods have a mild detergent effect; their fibrous texture helps physically scrub the surfaces of the teeth, while their high water content stimulates saliva production. Additionally, evaluating dairy consumption and dental health is important, as unsweetened dairy products like cheese and plain yogurt contain casein and calcium, which help buffer oral acids and promote enamel remineralization.
Calcium Metabolism and Demineralization
A persistent myth surrounding pregnancy is that the developing baby “steals” calcium directly from the mother’s teeth, leading to the old adage “lose a tooth for every child.” Clinically, this is entirely false. The calcium within the crystalline structure of adult teeth is stable and cannot be resorbed into the bloodstream to supply the fetus. However, calcium can be drawn from the maternal alveolar bone (the jawbone supporting the teeth) if dietary intake is insufficient. Furthermore, if the oral environment is constantly acidic due to morning sickness or frequent snacking, the teeth will demineralize from the outside in. Ensuring adequate systemic calcium and vitamin D intake is crucial for both fetal skeletal development and maintaining the integrity of the maternal jawbone [5]. This systemic nutritional support is just as important as understanding the timeline of neonatal dental development for the child’s future health.
When to See a Doctor: Important Clinical Considerations
While mild bad breath and slight gingival bleeding are common during pregnancy, certain clinical signs indicate that the condition has progressed beyond simple pregnancy gingivitis and requires immediate professional intervention. Ignoring these red flags can lead to irreversible tissue damage and potential systemic complications.
Warning: Delaying periodontal treatment during pregnancy due to safety misconceptions can exacerbate systemic inflammation. Always consult a certified dental professional for a personalized risk assessment rather than relying solely on home remedies.
Dr. Cuong strongly advises that any sudden onset of severe halitosis accompanied by spontaneous gingival bleeding, purulent discharge (pus) from the gumline, or increased tooth mobility should be evaluated immediately. These are hallmark signs of advanced periodontitis, an active infection that destroys the bone supporting the teeth. Additionally, if bad breath is accompanied by localized, throbbing pain or sensitivity to hot and cold, it may indicate a deep carious lesion (cavity) that has reached the dental pulp, necessitating endodontic evaluation. Expectant mothers should never endure dental pain or severe infection under the false assumption that treatment is unsafe. Modern dental anesthetics, shielded digital radiography, and specific fluoride applications are rigorously tested and proven safe for use during pregnancy when administered by a qualified professional.

Frequently Asked Questions
Is bad breath considered an early sign of pregnancy?
No, bad breath is not a primary or definitive early sign of pregnancy. However, as hormonal levels shift and morning sickness begins in the first trimester, secondary changes in the oral microbiome can lead to noticeable halitosis. It is a byproduct of physiological changes rather than a diagnostic indicator of conception.
Can morning sickness permanently damage my teeth and cause bad breath?
Yes, frequent vomiting introduces highly acidic gastric contents into the oral cavity, which can cause permanent enamel erosion if not managed. This erosion creates micro-cavities and rough surfaces where odor-causing bacteria thrive, exacerbating bad breath. Rinsing with baking soda and water immediately after vomiting is crucial to prevent this damage.
Are mouthwashes safe to use during pregnancy to treat halitosis?
Yes, alcohol-free, clinically approved mouthwashes are entirely safe and highly recommended during pregnancy. They help neutralize volatile sulfur compounds without causing the mucosal desiccation associated with alcohol-based rinses. Always consult your dentist to ensure the specific active ingredients (such as cetylpyridinium chloride or low-dose chlorhexidine) are appropriate for your condition.
Will my bad breath naturally disappear after giving birth?
In most cases, pregnancy-induced halitosis resolves postpartum as hormone levels stabilize and salivary flow normalizes. However, if the bad breath was caused by advanced periodontal disease, deep calculus buildup, or untreated decay that developed during the pregnancy, professional dental intervention will still be required to eliminate the odor completely.
Is it safe to undergo professional dental cleaning while pregnant?
Yes, professional dental cleanings are completely safe and highly encouraged during pregnancy. The second trimester is generally considered the most comfortable time for routine scaling and prophylaxis to manage pregnancy gingivitis and halitosis. Removing hardened plaque is essential to reduce the bacterial load and prevent systemic inflammation.
References
- Journal of Periodontology. Hormonal influences on the periodontium during pregnancy. (2021).
- American Dental Association (ADA). Oral health care during pregnancy and through the lifespan. (2022).
- Clinical Oral Investigations. Volatile sulfur compounds and halitosis in pregnant women: A clinical study. (2020).
- International Journal of Dentistry. The impact of hyperemesis gravidarum on oral health and salivary pH. (2019).
- Journal of Clinical Periodontology. Periodontal disease and adverse pregnancy outcomes: A systematic review. (2023).



