Natal teeth are teeth present in an infant’s mouth at birth, representing a rare clinical anomaly that requires prompt pediatric dental evaluation. Typically presenting as lower primary central incisors, these prematurely erupted teeth can lead to feeding difficulties, sublingual ulceration, or severe airway aspiration risks if not properly assessed and managed by a dental professional.
Clinical Summary:
Natal teeth represent a rare but significant pediatric dental condition where an infant is born with prematurely erupted teeth. Unlike neonatal teeth, which erupt within the first month of life, natal teeth are present at delivery. Clinical management depends heavily on the tooth’s mobility, root development, and its impact on breastfeeding mechanics. While asymptomatic, stable natal teeth can be safely retained, hypermobile teeth lacking root structure often necessitate extraction to mitigate the risk of airway aspiration and to resolve Riga-Fede disease (traumatic ulceration of the infant’s tongue). Comprehensive evaluation by a pediatric dental specialist ensures safe, evidence-based intervention, balancing the preservation of the primary dentition with the immediate physiological safety of the newborn.
Key Takeaways:
- Natal teeth are present at birth, whereas neonatal teeth erupt shortly after delivery.
- The vast majority of these teeth are mandibular central incisors with poor or absent root formation.
- A primary clinical concern is Riga-Fede disease, which causes painful, traumatic ulcerations on the ventral surface of the infant’s tongue.
- Extraction is generally delayed to allow for adequate Vitamin K synthesis, preventing postoperative hemorrhage.
- Conservative treatments include smoothing the incisal edges or applying composite resin to protect maternal tissues and the infant’s oral mucosa during breastfeeding.
Understanding Natal Teeth: Clinical Definition and Classification
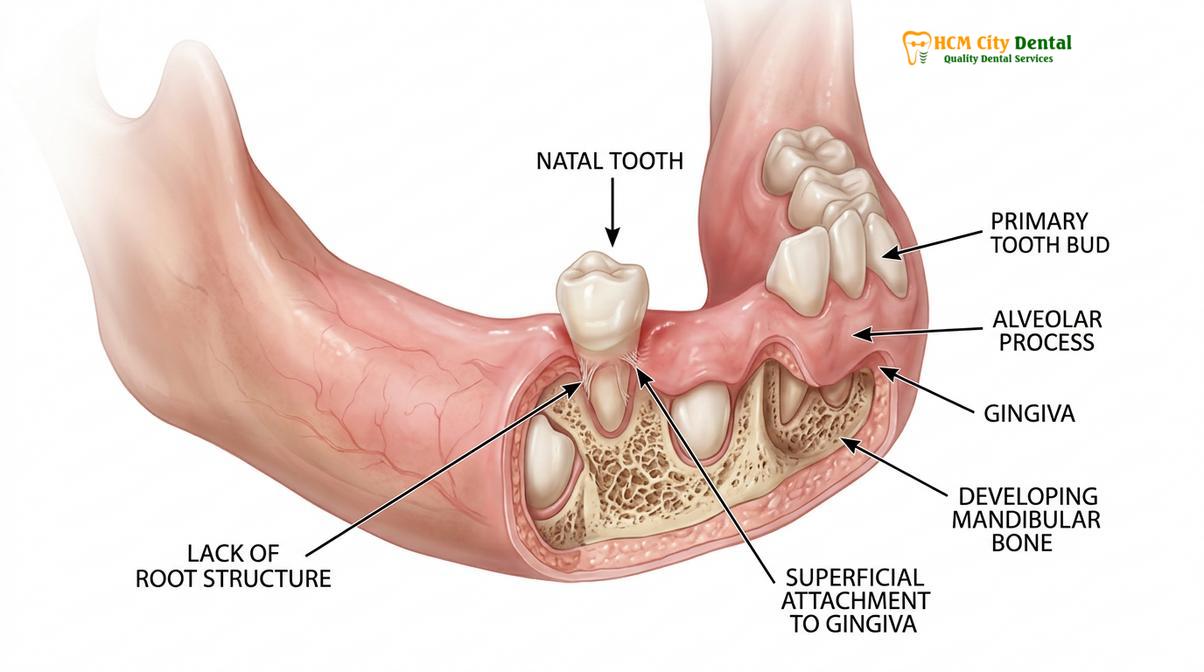
Natal teeth are prematurely erupted primary teeth present at birth, classified clinically based on their degree of alveolar attachment, mobility, and structural maturity.
The normal eruption of primary teeth typically begins around six months of age. However, in rare instances, infants are born with teeth already present in the oral cavity. These are clinically defined as natal teeth. It is crucial to differentiate them from neonatal teeth, which are not present at birth but erupt prematurely shortly after. The incidence of this phenomenon is relatively rare, with global epidemiological studies suggesting an occurrence rate ranging from 1 in 2,000 to 1 in 3,500 live births[1]. There is a slight predilection for females, though the statistical significance varies across different demographic populations.
Anatomically, the teeth most frequently affected are the lower primary central incisors, accounting for approximately 85% of all cases. Maxillary incisors account for about 11%, while mandibular canines and molars make up the remaining rare occurrences. These teeth usually erupt in pairs. Unlike normal primary dentition, natal teeth often exhibit hypoplastic enamel, poor dentin formation, and a distinct lack of root development. This structural immaturity is what leads to their characteristic hypermobility.
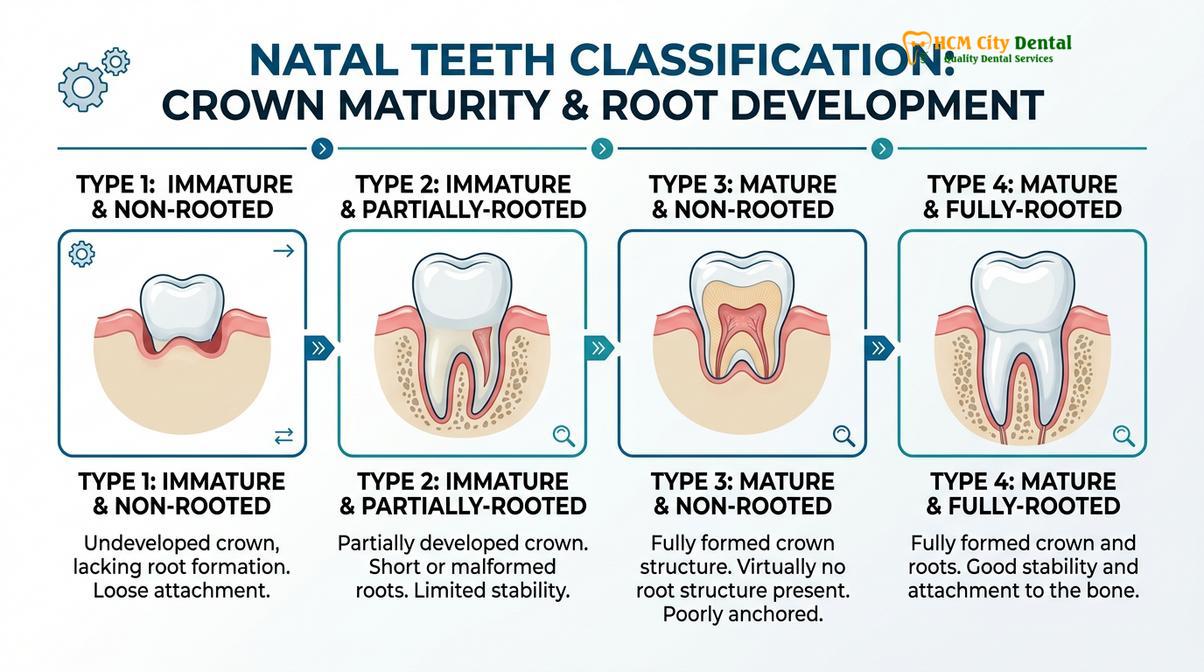
To standardize clinical assessment and treatment planning, dental professionals utilize specific classification systems. The most widely accepted clinical categorization divides these prematurely erupted teeth into four distinct categories based on their morphological characteristics and degree of attachment to the surrounding alveolar bone and gingival tissues.
| Category | Clinical Description | Root Development | Management Implication |
|---|---|---|---|
| Category 1 | A shell-like crown structure loosely attached to the alveolus by a rim of oral mucosa. | No root formation. | High risk of aspiration; extraction is almost always indicated. |
| Category 2 | A solid crown loosely attached to the alveolus by oral mucosa. | Little to no root formation. | Moderate to high risk; requires close monitoring or extraction based on mobility. |
| Category 3 | The incisal edge of the crown has just erupted through the oral mucosa. | Partial root development. | Often retained; conservative management and observation preferred. |
| Category 4 | A mucosal swelling with the tooth unerupted but palpable beneath the gums. | Developing root. | Observation; normal eruption sequence is expected. |
Understanding these categories is paramount for any clinician providing comprehensive general dentistry care protocols. The classification directly dictates the urgency and type of intervention required. A Category 1 tooth, for instance, is essentially a floating crown held only by soft tissue, presenting an immediate danger to the infant’s airway.
Etiology and Associated Genetic Syndromes
The exact cause of natal teeth remains multifactorial, often linked to superficial tooth germ positioning, genetic inheritance, or specific underlying systemic syndromes.
The precise etiology of natal teeth is not fully understood, but modern pediatric dentistry attributes the phenomenon to a combination of anatomical, genetic, and environmental factors. The most widely accepted anatomical theory suggests that the developing tooth germ is positioned abnormally close to the surface of the alveolar bone. This superficial positioning predisposes the tooth to erupt prematurely, bypassing the normal timeline of osteoclastic bone resorption and root elongation that typically accompanies tooth eruption[2].
Genetics also play a significant role. A positive family history is frequently reported in cases of natal teeth, suggesting an autosomal dominant inheritance pattern with incomplete penetrance in some families. If a parent or sibling had prematurely erupted teeth, the likelihood of the infant presenting with the same condition increases significantly. This genetic link is a vital component of the patient’s medical history during the initial consultation.
Furthermore, the presence of natal teeth can sometimes serve as an early clinical marker for underlying systemic conditions or genetic syndromes. While most cases are isolated anomalies in otherwise healthy infants, clinicians must remain vigilant for associated disorders. Syndromes known to have a higher incidence of natal teeth include Ellis-van Creveld Syndrome, Hallermann-Streiff Syndrome, Pierre Robin Sequence, and Sotos Syndrome.
Clinical Complications and Diagnostic Evaluation
Evaluating natal teeth requires assessing hypermobility, the presence of Riga-Fede disease, and the potential for maternal trauma during breastfeeding to determine the appropriate intervention.
The presence of a tooth at birth is not merely an anatomical curiosity; it presents several immediate clinical challenges that can significantly impact the infant’s health and the mother’s well-being. The diagnostic evaluation must be thorough, focusing on three primary complications: the risk of aspiration, infant oral ulceration, and feeding difficulties.
The most severe potential complication is the aspiration of a highly mobile tooth. Because natal teeth often lack root structure, they are held in place only by a fragile rim of gingival mucosa. The mechanical forces exerted during crying, suckling, or coughing can easily dislodge the tooth. If the dislodged tooth falls into the posterior oropharynx, it can be aspirated into the respiratory tract, leading to a life-threatening airway obstruction or aspiration pneumonia.
Another frequent and painful complication is Riga-Fede disease. This condition is characterized by a traumatic ulceration that develops on the ventral surface of the infant’s tongue. During the natural suckling motion, the infant’s tongue protrudes and rubs against the sharp incisal edge of the natal tooth. Over time, this constant friction strips away the delicate mucosal epithelium, creating a deep, fibrotic ulcer[3]. Riga-Fede disease is highly painful for the infant, often leading to a refusal to feed, subsequent dehydration, and failure to thrive.

“The presence of natal teeth requires a delicate balance between preserving the primary dentition and mitigating immediate risks. Our primary diagnostic objective is to rule out aspiration hazards while ensuring the infant can feed without pain or nutritional compromise,” explains Dr. Nguyen Van Cuong.
Maternal complications are equally significant. Breastfeeding an infant with natal teeth can cause severe lacerations and trauma to the mother’s nipple and areola. The pain associated with this trauma can disrupt the maternal-infant bonding process and lead to early, unintended cessation of breastfeeding. Therefore, the diagnostic evaluation must include a discussion with the mother regarding her comfort and any difficulties experienced during feeding.
Evidence-Based Treatment Workflows for Natal Teeth
Treatment strategies range from conservative observation and composite resin application to surgical extraction, depending strictly on tooth mobility and feeding complications.
The management of natal teeth is highly individualized. The decision to intervene surgically versus conservatively hinges on the clinical presentation, specifically the degree of mobility and the presence of complications like Riga-Fede disease. According to pediatric dental guidelines, the overarching goal is to maintain the tooth if it is safe to do so, as premature loss of a primary incisor can occasionally lead to minor space management issues later in childhood[4].
Conservative Management Protocols
If the natal tooth is stable, exhibits minimal mobility, and does not interfere with breastfeeding, conservative management is the treatment of choice. The clinician will closely monitor the tooth’s development. If the tooth is stable but has a sharp incisal edge causing mild irritation to the infant’s tongue or the mother’s breast, the dentist may perform a gentle ameloplasty. This involves using a specialized dental instrument to smooth and round off the sharp enamel edges.
In cases where smoothing is insufficient, a small dome of photopolymerizable composite resin can be bonded over the incisal edge. This creates a smooth, rounded surface that glides easily against the tongue and breast tissue, effectively preventing or treating early-stage Riga-Fede disease without the need for extraction.

Surgical Extraction Protocols
Extraction is strictly indicated when the natal tooth is hypermobile, posing an unacceptable risk of aspiration, or when conservative measures fail to resolve severe Riga-Fede disease and feeding refusal. However, the timing of the extraction is a critical medical consideration.
Newborn infants have a physiological deficiency of Vitamin K, a crucial component required by the liver to synthesize blood-clotting factors. The infant’s gut microbiome, which eventually produces Vitamin K, is not fully established at birth. Therefore, performing a surgical extraction in the first few days of life carries a high risk of prolonged, uncontrolled hemorrhage[5].
Standard medical protocol dictates that, unless the aspiration risk is critically imminent, extraction should be delayed until the infant is older. If immediate extraction is unavoidable due to extreme mobility, the pediatric dentist must consult with the infant’s pediatrician to ensure that a prophylactic intramuscular injection of Vitamin K has been administered prior to the procedure.
An infant was brought to HCMC Dental Clinic in Ho Chi Minh City presenting with a hypermobile lower central incisor and severe sublingual ulceration (Riga-Fede disease). The infant was experiencing significant weight loss due to feeding refusal. Upon examination, the tooth was classified as Category 1 with zero root formation. Following pediatric protocols and confirming prophylactic Vitamin K administration, the tooth was safely extracted under topical anesthesia. Within 48 hours, the sublingual ulcer began healing, and normal breastfeeding resumed, highlighting the efficacy of timely, evidence-based intervention.
The extraction procedure itself is generally straightforward due to the lack of root structure. A topical anesthetic is applied to the gingiva. The tooth is then gently grasped with sterile forceps or digital pressure and removed. Curettage of the socket is sometimes performed to remove any underlying odontogenic cellular remnants, preventing the continued development of root structures or cysts. The principles of atraumatic removal here mirror the foundational concepts used in more complex surgical extraction protocols in adults.
When to Seek Immediate Medical Attention
Parents should monitor natal teeth closely and seek immediate pediatric dental care if signs of hypermobility, feeding refusal, or oral ulcerations develop.
While some natal teeth remain stable and asymptomatic, their condition can change rapidly as the infant grows and begins to feed more vigorously. It is vital for parents and caregivers to understand the warning signs that necessitate urgent clinical evaluation. According to the Vietnam Ministry of Health (MOH) guidelines on pediatric oral health, early intervention is key to preventing severe complications in neonates[6].
Immediate medical or dental attention should be sought if the tooth becomes noticeably loose to the touch, as this significantly elevates the risk of spontaneous dislodgement and airway aspiration. Additionally, if the infant consistently refuses to breastfeed or bottle-feed, cries excessively during feeding attempts, or shows signs of dehydration, a thorough oral examination is required to rule out Riga-Fede disease. Parents should also inspect the underside of the infant’s tongue daily; the appearance of any red, raw, or white ulcerated patches warrants a prompt visit to a pediatric dental specialist.
Psychological Impact and Parental Counseling
Effective management of natal teeth extends beyond surgical intervention, requiring empathetic parental counseling to alleviate anxiety and dispel cultural misconceptions.
The birth of a child is a highly emotional period, and the unexpected discovery of teeth in a newborn can cause significant distress and anxiety for the parents. In many cultures, natal teeth are surrounded by folklore and superstition, sometimes viewed negatively as a bad omen. It is the responsibility of the dental professional to provide clear, scientifically backed reassurance, explaining that natal teeth are a recognized, manageable anatomical variation rather than a cause for alarm.
Dr. Nguyen Van Cuong, a leading specialist at HCMC Dental Clinic, emphasizes the importance of conservative management whenever possible. Dr. Cuong frequently educates parents on the nuances of early childhood oral health, drawing parallels to the preventative strategies outlined in his clinical guide to tooth decay. By fostering an environment of trust and open communication, the clinical team ensures that parents feel supported throughout the diagnostic and treatment phases.

“Parental education is just as critical as the clinical procedure itself. When parents understand the anatomical reasons behind natal teeth and the safety protocols we follow, their anxiety diminishes, allowing them to focus entirely on the well-being and nourishment of their newborn,” notes Dr. Cuong.
Counseling also involves practical advice on oral hygiene for the infant. Even if the natal tooth is retained, parents must be instructed on how to gently clean the tooth and surrounding gums using a soft, damp cloth to prevent plaque accumulation and gingival inflammation. This early introduction to oral hygiene sets a positive foundation for the child’s future dental health.
Comprehensive Care at HCMC Dental Clinic
Managing natal teeth requires a delicate, evidence-based approach that prioritizes the infant’s airway safety, nutritional intake, and overall comfort. Whether the clinical situation calls for conservative monitoring, composite resin application, or safe surgical extraction, timely intervention by a qualified pediatric dental professional is essential. If you have concerns about your newborn’s oral health or notice prematurely erupted teeth, schedule a specialized consultation at HCMC Dental Clinic, Ho Chi Minh City, to ensure your child receives the highest standard of compassionate, expert care.
References
- Journal of Clinical Pediatric Dentistry. Management of natal and neonatal teeth: A clinical review. (2021).
- International Journal of Paediatric Dentistry. Histological and clinical evaluation of prematurely erupted primary incisors. (2019).
- Pediatric Dentistry Journal. Riga-Fede disease and its association with natal teeth: Diagnostic criteria. (2020).
- American Academy of Pediatric Dentistry (AAPD). Guidelines on the management of acute pediatric dental anomalies. (2022).
- Journal of Oral and Maxillofacial Surgery. Hemostasis and Vitamin K prophylaxis in neonatal dental extractions. (2018).
- Vietnam Ministry of Health (MOH). National Guidelines on Pediatric Oral Health and Neonatal Care. (2023).