Is fluoride bad for your teeth? When used in appropriate, clinically recommended doses, fluoride is highly beneficial and safe for preventing tooth decay. However, excessive systemic exposure during early childhood tooth development can cause dental fluorosis, highlighting the need for professionally guided, age-appropriate fluoride management.
Clinical Summary:
Fluoride remains one of the most extensively researched and effective preventive agents in modern dentistry. By integrating into the crystalline structure of tooth enamel, it significantly enhances resistance to bacterial acid attacks and promotes the remineralization of early carious lesions. While the therapeutic benefits of topical and systemic fluoride are well-documented, concerns regarding toxicity and dental fluorosis are valid when exposure exceeds optimal levels. A balanced, evidence-based approach—combining community water fluoridation, daily fluoridated toothpaste, and targeted professional applications—ensures maximum caries prevention while minimizing the risk of adverse cosmetic or systemic effects. Clinical supervision is essential to tailor fluoride exposure to individual patient risk profiles.
Key Takeaways:
- Fluoride converts vulnerable hydroxyapatite into highly durable fluorapatite, actively reversing early-stage tooth decay.
- Overexposure to systemic fluoride during early childhood can lead to dental fluorosis, a cosmetic alteration of the enamel.
- Topical fluoride (toothpaste, mouthwash, varnishes) provides localized protection without significant systemic absorption risks.
- Professional in-office fluoride treatments are highly recommended for patients with dry mouth, active decay, or orthodontic appliances.
- Consulting a qualified dental professional ensures that your daily fluoride intake is both safe and optimized for your specific oral health needs.
The Biological Role of Fluoride in Dental Health
Fluoride actively protects teeth by integrating into the enamel structure, converting naturally occurring hydroxyapatite into the more acid-resistant fluorapatite to halt and reverse early decay.
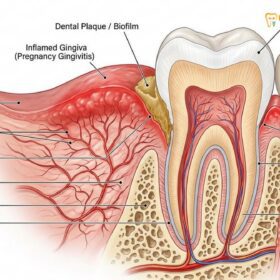
To fully understand the impact of fluoride on oral health, it is essential to examine the dynamic microscopic environment of the human mouth. Every day, the protective outer layer of the teeth—the enamel—undergoes a continuous cycle of demineralization and remineralization. When we consume carbohydrates and sugars, cariogenic bacteria in the dental plaque metabolize these fermentable substrates, producing lactic acid and other organic acids as byproducts. This localized drop in pH strips essential minerals, primarily calcium and phosphate, from the enamel matrix in a process known as demineralization.
If demineralization outpaces the body’s natural repair mechanisms, the enamel structure weakens, eventually collapsing to form a cavity. This is where fluoride intervenes as a critical therapeutic agent. When fluoride is present in the oral cavity, it acts as a catalyst for remineralization. It attracts calcium and phosphate ions from the saliva back into the porous, demineralized enamel. More importantly, the fluoride ion physically replaces the hydroxyl ion in the enamel’s crystalline structure, transforming hydroxyapatite into fluorapatite [1].
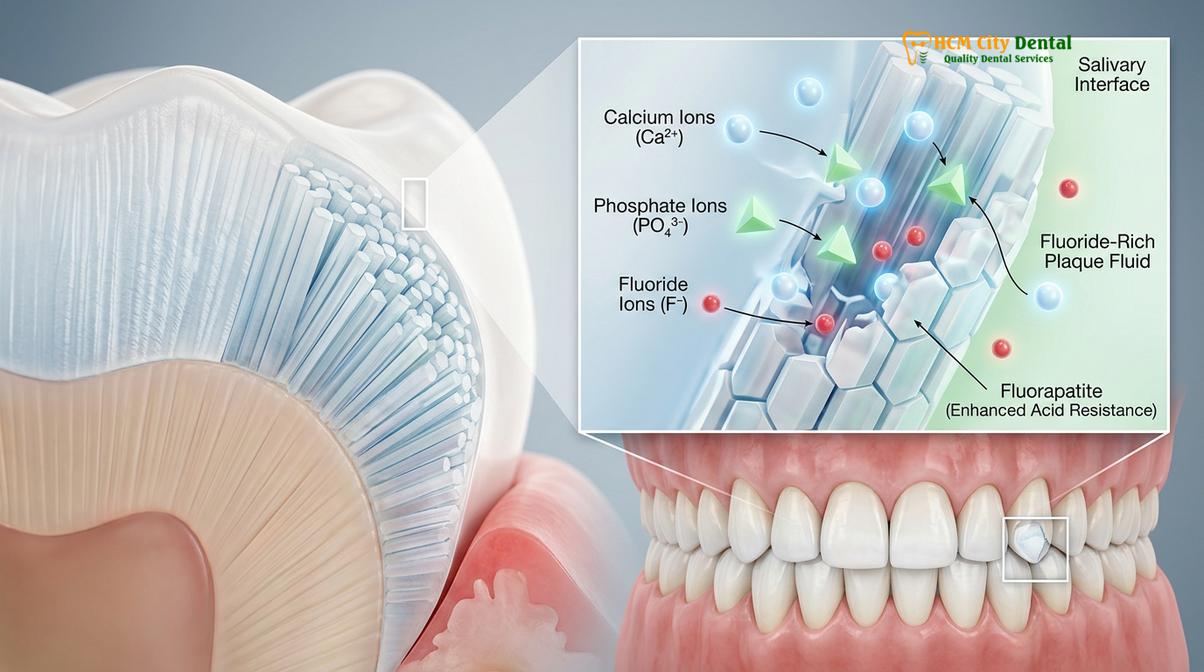
Fluorapatite is significantly more robust than natural enamel. While normal hydroxyapatite begins to dissolve at a critical pH of approximately 5.5, fluorapatite can withstand acidic environments down to a pH of 4.5. This means that teeth fortified with fluoride are vastly more resilient against the daily acid attacks orchestrated by plaque bacteria. Furthermore, fluoride exhibits direct antimicrobial properties. In high concentrations, it can cross the bacterial cell membrane as hydrogen fluoride (HF). Once inside the alkaline cytoplasm of the bacteria, it dissociates, releasing fluoride ions that inhibit enolase—a crucial enzyme in the bacterial glycolysis pathway. This effectively starves the bacteria, reducing their ability to produce acid and multiply [2].
“The continuous presence of low-concentration fluoride in the oral cavity is the most critical factor in shifting the balance from enamel demineralization to active remineralization, fundamentally altering the trajectory of dental caries.”
Dr. Nguyen Van Cuong, a leading expert at HCMC Dental Clinic, frequently emphasizes to his patients that fluoride is not merely a protective shield, but an active participant in the ongoing cellular repair of the tooth structure. By maintaining a consistent, low-level presence of fluoride through daily oral hygiene, patients can effectively manage their caries risk and maintain optimal comprehensive general dental care.
Is Fluoride Bad for Your Teeth? Understanding the Risks
Fluoride is not inherently bad for teeth; however, excessive systemic ingestion during the critical years of tooth development can lead to fluorosis, a structural enamel defect.
The question “is fluoride bad for teeth” frequently arises in clinical consultations, driven by conflicting information regarding its safety. In dentistry, as in all fields of medicine, the distinction between a therapeutic benefit and a potential toxin lies entirely in the dosage. When utilized according to established clinical guidelines, fluoride is exceptionally safe. However, excessive exposure—particularly systemic ingestion during early childhood—can lead to specific adverse effects.
The most common clinical manifestation of excessive fluoride intake is dental fluorosis. This condition occurs exclusively when a child ingests higher-than-optimal levels of fluoride while their permanent teeth are still forming beneath the gums (typically between birth and eight years of age). During the secretory and maturation phases of amelogenesis (enamel formation), excess circulating fluoride disrupts the function of ameloblasts—the cells responsible for laying down enamel. This disruption results in a hypomineralized enamel matrix.

Clinically, dental fluorosis presents on a spectrum of severity:
- Questionable to Mild Fluorosis: Characterized by faint, lacy white opaque lines or small white spots on the enamel surface. This form is purely cosmetic, does not weaken the tooth, and is often imperceptible to the untrained eye.
- Moderate Fluorosis: The white opaque areas cover a larger percentage of the tooth surface, and the enamel may begin to show slight signs of wear or brown staining due to increased porosity.
- Severe Fluorosis: The enamel is significantly hypomineralized, leading to widespread brown staining, surface pitting, and a brittle tooth structure that may be more susceptible to mechanical wear and secondary decay.
Clinical Warning: Dental fluorosis only affects developing teeth. Adults and older children whose permanent teeth have already erupted cannot develop dental fluorosis, regardless of how much topical or systemic fluoride they are exposed to.
Beyond dental fluorosis, chronic ingestion of extremely high levels of fluoride over decades can lead to skeletal fluorosis, a condition characterized by joint stiffness, bone pain, and osteosclerosis. However, this condition is exceedingly rare in regions with regulated water supplies and is typically associated with geographic areas where natural groundwater fluoride levels exceed 4.0 to 10.0 parts per million (ppm), or in cases of severe industrial exposure [3].
To address the common query, “is fluoride safe”, dental professionals rely on decades of epidemiological data. The consensus among major global health organizations is that the preventive benefits of optimal fluoride exposure far outweigh the risks of mild cosmetic fluorosis. The key to safety is meticulous supervision of pediatric fluoride intake, ensuring that young children do not swallow large quantities of fluoridated toothpaste.
Professional Fluoride Applications in Clinical Practice
In-office treatments utilize highly concentrated varnishes, foams, or gels to provide immediate, targeted protection for patients identified as having a high risk for dental caries.
While daily at-home fluoride use provides an essential baseline of protection, many patients require the enhanced intervention of professional, high-concentration fluoride therapies. A qualified fluoride treatment dentist will assess a patient’s individual Caries Risk Assessment (CRA) to determine the necessity, frequency, and modality of in-office fluoride application.
Professional fluoride treatments deliver a massive, localized dose of fluoride directly to the enamel surface, creating a temporary reservoir of calcium fluoride (CaF2). Over the following weeks and months, this reservoir slowly releases fluoride ions into the saliva and plaque fluid, providing sustained remineralization benefits long after the patient has left the dental chair [4]. These treatments are particularly crucial for patients undergoing orthodontic therapy, individuals suffering from xerostomia (dry mouth), patients with exposed root surfaces due to gingival recession, and those with a history of frequent restorative work.

In modern clinical practice, there are three primary delivery methods for professional fluoride:
| Fluoride Modality | Concentration | Clinical Application & Indications |
|---|---|---|
| Fluoride Varnish (5% NaF) | 22,600 ppm | Painted directly onto the teeth. Sets rapidly on contact with saliva. Ideal for young children, patients with strong gag reflexes, and targeted application on specific vulnerable areas. |
| Acidulated Phosphate Fluoride (APF) Gel | 12,300 ppm | Applied via disposable trays for 1-4 minutes. The acidic pH (3.5) enhances rapid enamel uptake. Contraindicated for patients with porcelain crowns or composite resins, as the acid can etch these materials. |
| Neutral Sodium Fluoride Foam | 9,050 ppm | Applied via trays. Neutral pH makes it safe for all dental restorations. Often preferred for patients who cannot tolerate the acidic taste of APF gels. |
The application of a dental fluoride gel or varnish is a rapid, non-invasive procedure. For instance, when applying a 5% sodium fluoride varnish, the clinician will first dry the teeth using gauze or compressed air. The varnish is then painted onto the buccal, lingual, and occlusal surfaces using a microbrush. Because the varnish adheres instantly upon contact with saliva, the patient can close their mouth immediately. Post-operative instructions typically advise the patient to avoid eating hard, sticky, or hot foods, and to refrain from brushing or flossing for at least 4 to 6 hours to maximize fluoride uptake.
At HCMC Dental Clinic in Ho Chi Minh City, Dr. Nguyen Van Cuong integrates professional fluoride applications into routine preventive care protocols. By identifying early signs of demineralization during routine dental examinations, the clinical team can intervene with targeted fluoride therapy, often preventing the need for invasive drilling and filling procedures.
At-Home Fluoride Use: Guidelines for Optimal Safety
Daily use of fluoridated toothpaste and mouthwashes is safe and highly effective when patients strictly adhere to age-appropriate dosing and proper spitting protocols.
The foundation of caries prevention relies heavily on patient compliance with daily at-home oral hygiene protocols. The most ubiquitous and effective vehicle for topical fluoride delivery is fluoridated toothpaste. Standard over-the-counter toothpastes typically contain between 1,000 and 1,500 ppm of fluoride, usually in the form of sodium fluoride (NaF), sodium monofluorophosphate (SMFP), or stannous fluoride (SnF2). Stannous fluoride offers the added clinical benefit of broad-spectrum antimicrobial action, making it highly effective against gingivitis as well as decay.
To maximize the benefits of at-home fluoride while minimizing any risks of systemic ingestion, clinical guidelines dictate specific age-based dosing strategies:
- Infants and Toddlers (Under 3 years): As soon as the first primary tooth erupts, parents should begin brushing the child’s teeth twice daily using a “smear” or “rice-grain-sized” amount of fluoridated toothpaste. This minute quantity provides topical protection while ensuring that, even if swallowed entirely, the systemic dose remains well below the threshold for fluorosis.
- Children (Ages 3 to 6 years): Once a child develops the cognitive and motor skills to reliably spit out excess toothpaste, the dosage can be increased to a “pea-sized” amount. Parents must actively supervise brushing sessions to enforce spitting and prevent the child from swallowing the paste or eating it directly from the tube.
- Adults and Adolescents: A standard ribbon of toothpaste is appropriate. For optimal remineralization, clinicians recommend the “spit, don’t rinse” technique. After achieving the optimal brushing duration of two minutes, patients should spit out the excess foam but avoid rinsing their mouth with water. Leaving a thin film of fluoridated paste on the teeth significantly prolongs the contact time between the fluoride ions and the enamel.
For adult patients with an exceptionally high caries risk—such as those undergoing head and neck radiation therapy, individuals with severe medication-induced xerostomia, or patients with extensive crown and bridge work—a dentist may prescribe a high-concentration toothpaste containing 5,000 ppm fluoride. This prescription-strength dentifrice provides a robust defense mechanism against aggressive decay patterns [5].
Clinical Case Study: Managing High Caries Risk
A 45-year-old patient presented to HCMC Dental Clinic with severe dry mouth caused by antihypertensive medications, leading to rapid, widespread root surface decay. Dr. Cuong implemented a comprehensive preventive protocol, including the prescription of a 5,000 ppm fluoride toothpaste for daily use and quarterly in-office 5% NaF varnish applications. Within six months, the active carious lesions had arrested, the enamel surfaces hardened, and no new cavities developed, demonstrating the profound efficacy of targeted fluoride therapy in compromised oral environments.
“The transition from generic oral hygiene to a prescription-based fluoride regimen is often the defining factor in saving the natural dentition of patients suffering from severe salivary gland dysfunction.”
Water Fluoridation: A Global Public Health Strategy
Community water fluoridation remains a cornerstone of preventive dentistry, providing equitable baseline caries reduction across diverse populations when maintained at optimal levels.
Community water fluoridation is widely recognized by major health and medical organizations as one of the top ten public health achievements of the 20th century. The premise is simple yet profoundly impactful: adjusting the natural fluoride concentration of public water supplies to an optimal level that maximizes caries prevention while minimizing the risk of dental fluorosis. Currently, the recommended optimal concentration is 0.7 parts per million (ppm), equivalent to 0.7 milligrams of fluoride per liter of water.
The mechanism of action for water fluoridation is dual-natured. Historically, it was believed that the primary benefit was systemic—that ingested fluoride was incorporated into developing teeth. While this systemic incorporation does occur, contemporary clinical research confirms that the predominant benefit of water fluoridation is actually topical. Every time a person drinks fluoridated water, consumes food prepared with it, or swallows saliva containing trace amounts of recycled fluoride, the teeth are bathed in a low-concentration fluoride solution. This constant, low-level exposure is the ideal environment for continuous enamel remineralization.
Water fluoridation is particularly vital from a health equity standpoint. It provides baseline dental protection to all members of a community, regardless of socioeconomic status, access to professional dental care, or compliance with daily oral hygiene routines. Furthermore, by reducing the overall bacterial load and decay rates in a population, optimal fluoride exposure indirectly helps manage secondary oral health issues, such as chronic bad breath caused by necrotic tooth structure and deep carious lesions.
Despite its proven efficacy, water fluoridation occasionally faces public skepticism. It is crucial for patients to rely on peer-reviewed scientific data and consult with their healthcare providers when evaluating the safety of their local water supply. For individuals living in rural areas relying on private well water, testing the natural fluoride levels is a critical step. If the well water is deficient in fluoride, pediatricians or dentists may recommend dietary fluoride supplements (drops or tablets) for young children. Conversely, if the natural fluoride levels are excessively high, alternative drinking water sources or reverse osmosis filtration systems may be necessary to prevent fluorosis. Selecting a qualified dental professional ensures that your family receives accurate, localized advice regarding systemic fluoride exposure.
Important Clinical Considerations: When to See a Doctor
While fluoride is a standard component of daily oral care, certain clinical scenarios require professional evaluation and personalized management. Patients should schedule a comprehensive dental examination if they observe any of the following signs or fall into specific high-risk categories:
- Visible Enamel Changes in Children: If you notice chalky white spots, lacy striations, or brown pitting on your child’s newly erupted permanent teeth, a clinical assessment is necessary to diagnose potential dental fluorosis or early enamel demineralization.
- Rapid Onset of Cavities: Adults experiencing a sudden increase in tooth decay, particularly along the gumline or around existing dental work, require immediate intervention. This often indicates a shift in the oral microbiome or a reduction in salivary flow, necessitating prescription-strength fluoride therapy.
- Chronic Dry Mouth (Xerostomia): Saliva is the natural carrier of fluoride, calcium, and phosphate. Patients suffering from dry mouth due to medications, autoimmune conditions (like Sjögren’s syndrome), or radiation therapy lack this natural defense and are highly dependent on supplemental fluoride to prevent catastrophic tooth loss.
- Orthodontic Treatment: Patients wearing traditional metal or ceramic braces are at a significantly higher risk for developing white spot lesions (decalcification) around the brackets. Enhanced fluoride protocols, including specialized rinses and varnishes, are mandatory during orthodontic therapy.
- Desire for Cosmetic Correction: If you are an adult with existing dental fluorosis who is unhappy with the mottled appearance of your teeth, consult a dentist. While fluorosis cannot be “cured,” the cosmetic impact can be successfully managed through microabrasion, resin infiltration, or professional teeth whitening solutions.

Ultimately, the management of fluoride is not a one-size-fits-all approach. It requires a nuanced understanding of a patient’s age, diet, medical history, and local environmental factors. By partnering with the experienced clinical team at HCMC Dental Clinic in Ho Chi Minh City, patients can ensure that their preventive strategies are both safe and scientifically optimized for long-term oral health.
If you have concerns about your family’s fluoride intake, or if you wish to undergo a comprehensive Caries Risk Assessment, we encourage you to schedule a consultation with our specialists. Early intervention and personalized preventive care are the cornerstones of a healthy, resilient smile.
Frequently Asked Questions
Can fluoride permanently damage my teeth?
No, fluoride does not permanently damage teeth when used at recommended therapeutic levels. However, excessive ingestion during early childhood tooth development can cause dental fluorosis, which alters the cosmetic appearance of the enamel but does not typically compromise its structural integrity. In severe cases of fluorosis, the enamel may become pitted, but this is rare and entirely preventable with proper dosing supervision.
Is fluoride-free toothpaste better for oral health?
Clinical evidence indicates that fluoride-free toothpaste is significantly less effective at preventing tooth decay. While it can physically remove plaque and food debris through mechanical brushing, it lacks the active remineralizing agents necessary to repair microscopic enamel damage and neutralize bacterial acids. Dental professionals strongly recommend fluoridated toothpaste for optimal caries prevention.
At what age should children start using fluoride toothpaste?
Children should begin using a tiny, smear-sized amount of fluoride toothpaste as soon as their first tooth erupts. Once they reach age three and can reliably spit out the excess foam, the amount can be increased to a pea-sized drop under adult supervision. This controlled exposure provides essential topical protection while minimizing the risk of systemic ingestion.
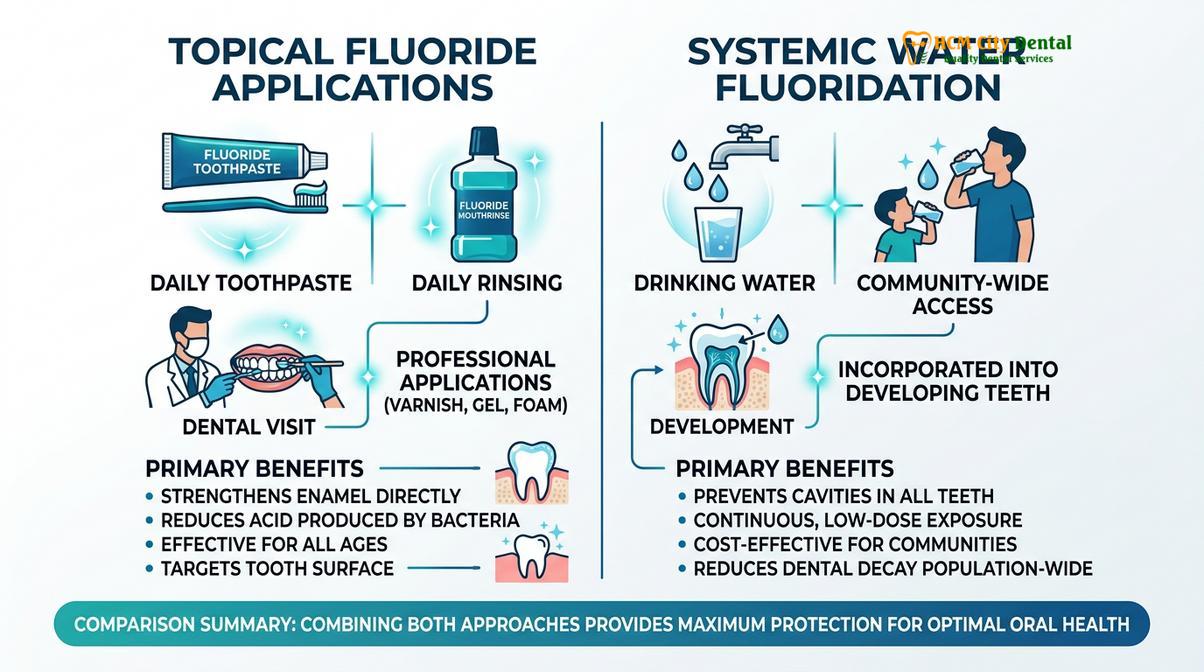
What is the difference between systemic and topical fluoride?
Systemic fluoride is ingested through water, dietary supplements, or certain foods, and it incorporates into developing teeth before they erupt into the mouth. Topical fluoride, found in toothpaste, mouthwashes, and professional dental varnishes, is applied directly to the surfaces of erupted teeth to strengthen the outer enamel and reverse early signs of decay.
How do I know if I need professional fluoride treatments?
You may need professional fluoride applications if you have a high risk of cavities, suffer from dry mouth, wear orthodontic appliances, or have exposed tooth roots due to gum recession. A comprehensive clinical evaluation by a dentist is required to determine your specific preventive needs and to prescribe the appropriate concentration and frequency of fluoride therapy.
References
- American Dental Association (ADA). Fluoridation Facts and Clinical Guidelines for Caries Management. (2022).
- Journal of Dental Research. The Mechanism of Dental Decay and Fluoride’s Role in Remineralization. (2020).
- World Health Organization (WHO). Inadequate or Excess Fluoride: A Major Public Health Concern. (2019).
- Cochrane Database of Systematic Reviews. Topical Fluoride for Preventing Dental Caries in Children and Adolescents. (2021).
- International Journal of Paediatric Dentistry. Clinical Management of Dental Fluorosis and Enamel Hypoplasia. (2023).