Halitosis, clinically recognized as oral malodor or bad breath, is a highly prevalent condition characterized by unpleasant odors emanating from the oral cavity. It is primarily caused by anaerobic bacteria breaking down proteins into volatile sulfur compounds, requiring professional dental evaluation to rule out underlying periodontal or systemic diseases.
Clinical Summary:
Halitosis is a multifactorial clinical condition predominantly originating from the oral cavity, accounting for 80 to 85 percent of documented cases. The primary pathophysiological mechanism involves Gram-negative anaerobic bacteria degrading sulfur-containing amino acids into volatile sulfur compounds (VSCs) such as hydrogen sulfide, methyl mercaptan, and dimethyl sulfide. Clinical management requires a comprehensive diagnostic approach, often utilizing organoleptic assessment and objective sulfide monitoring. Treatment prioritizes mechanical biofilm disruption, non-surgical periodontal therapy, and targeted antimicrobial mouth rinses. When intraoral causes are definitively ruled out, interdisciplinary referral is necessary to investigate extraoral etiologies, including otorhinolaryngological, gastrointestinal, or metabolic disorders.
Key Takeaways:
- Over 80% of halitosis cases originate intraorally due to tongue coating, gingivitis, or advanced periodontitis.
- Volatile sulfur compounds (VSCs) are the primary chemical agents responsible for the characteristic foul odor.
- Xerostomia (dry mouth) significantly exacerbates malodor by reducing the mechanical flushing and buffering action of saliva.
- Clinical diagnosis relies on organoleptic scoring combined with objective instrumental measurements like the Halimeter.
- Effective long-term treatment requires professional mechanical debridement combined with rigorous at-home oral hygiene protocols.
The Pathophysiology of Halitosis: The Biochemistry of Breath
Halitosis develops when anaerobic bacteria in the mouth degrade proteins into volatile sulfur compounds (VSCs). These malodorous gases, primarily hydrogen sulfide and methyl mercaptan, are the direct chemical cause of bad breath.
To effectively manage halitosis, it is crucial to understand the underlying biochemical processes that generate oral malodor. The oral cavity is a complex ecosystem harboring hundreds of bacterial species. In a healthy state, there is a symbiotic balance; however, when this balance is disrupted, pathogenic bacteria can proliferate. The primary culprits behind genuine halitosis are Gram-negative, proteolytic, anaerobic bacteria. These microorganisms thrive in oxygen-depleted environments, such as deep periodontal pockets, the intricate crypts of the tonsils, and the posterior dorsal surface of the tongue.[1]
The biochemical pathway of halitosis begins with the degradation of organic substrates. Food debris, desquamated epithelial cells, salivary proteins, and blood elements (in cases of gingival bleeding) provide a rich source of sulfur-containing amino acids, specifically cysteine and methionine. When anaerobic bacteria metabolize these amino acids, they excrete Volatile Sulfur Compounds (VSCs) as metabolic byproducts. The three primary VSCs responsible for oral malodor are:
- Hydrogen Sulfide (H₂S): Often compared to the smell of rotten eggs, this compound is primarily produced by bacteria residing on the dorsal surface of the tongue.
- Methyl Mercaptan (CH₃SH): Characterized by a strong, feces-like odor, this compound is heavily associated with severe periodontal disease and deep gingival pocketing.
- Dimethyl Sulfide ((CH₃)₂S): Typically exhibiting a sweet, cabbage-like odor, this compound is more frequently associated with extraoral or systemic causes of halitosis.

Beyond VSCs, other malodorous compounds contribute to the overall scent profile of halitosis. These include diamines such as putrescine and cadaverine (which smell like decaying meat), as well as short-chain fatty acids like butyric acid (smelling like vomit) and propionic acid. The volatility of these compounds is highly dependent on the pH of the oral environment. An alkaline pH facilitates the transition of these compounds from a dissolved state in saliva into a gaseous state, making the odor detectable in the exhaled breath.[2]
“The transition of sulfur compounds from the liquid phase of saliva to the gaseous phase of breath is the critical biochemical moment when localized bacterial metabolism becomes a socially detectable condition.”
Intraoral vs. Extraoral Etiology: Identifying the Source
While the vast majority of halitosis cases stem from oral issues like gum disease and tongue biofilm, systemic conditions such as respiratory infections or gastrointestinal disorders can also be responsible.
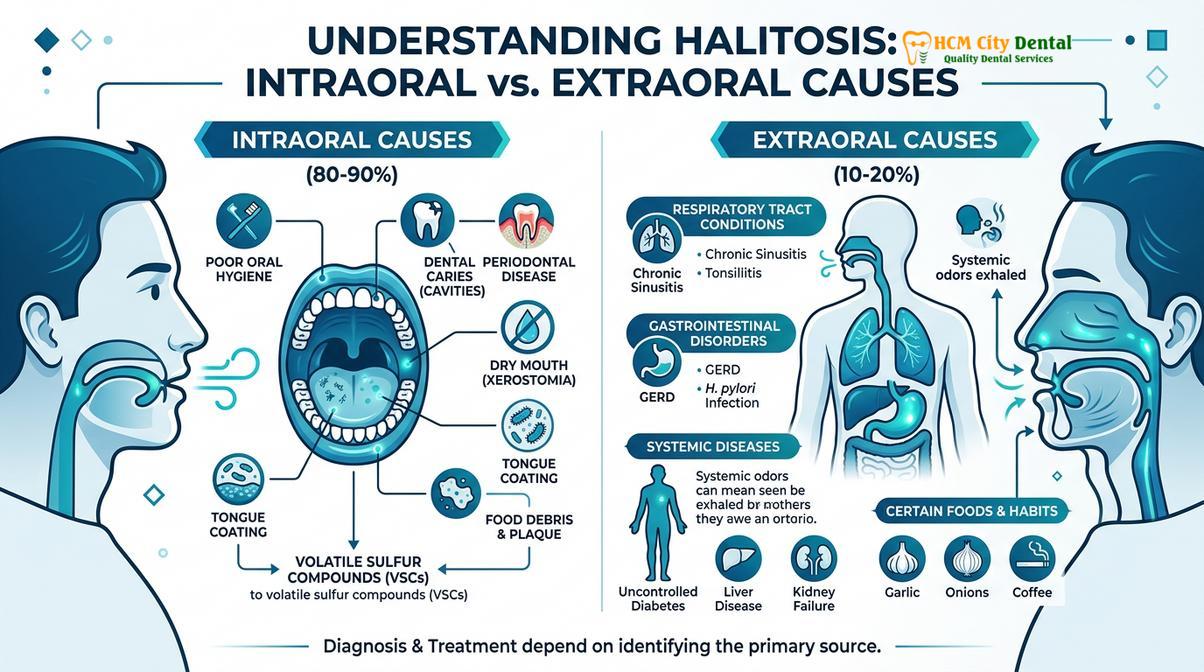
Clinical diagnostics categorize halitosis based on its origin. Understanding whether the malodor is intraoral (originating within the mouth) or extraoral (originating elsewhere in the body) dictates the entire treatment workflow. As a foundational principle of General Dentistry, ruling out local factors is always the first step before pursuing complex systemic evaluations.
Intraoral Causes (80% – 85% of Cases)
The oral cavity provides an ideal incubator for odor-causing bacteria due to its constant temperature, high humidity, and abundant nutrient supply. The most frequent intraoral causes include:
- Tongue Coating: The posterior third of the dorsal tongue has a highly irregular surface with deep fissures and elongated filiform papillae. This topography traps bacteria, post-nasal drip, and food particles, creating a dense, malodorous biofilm.
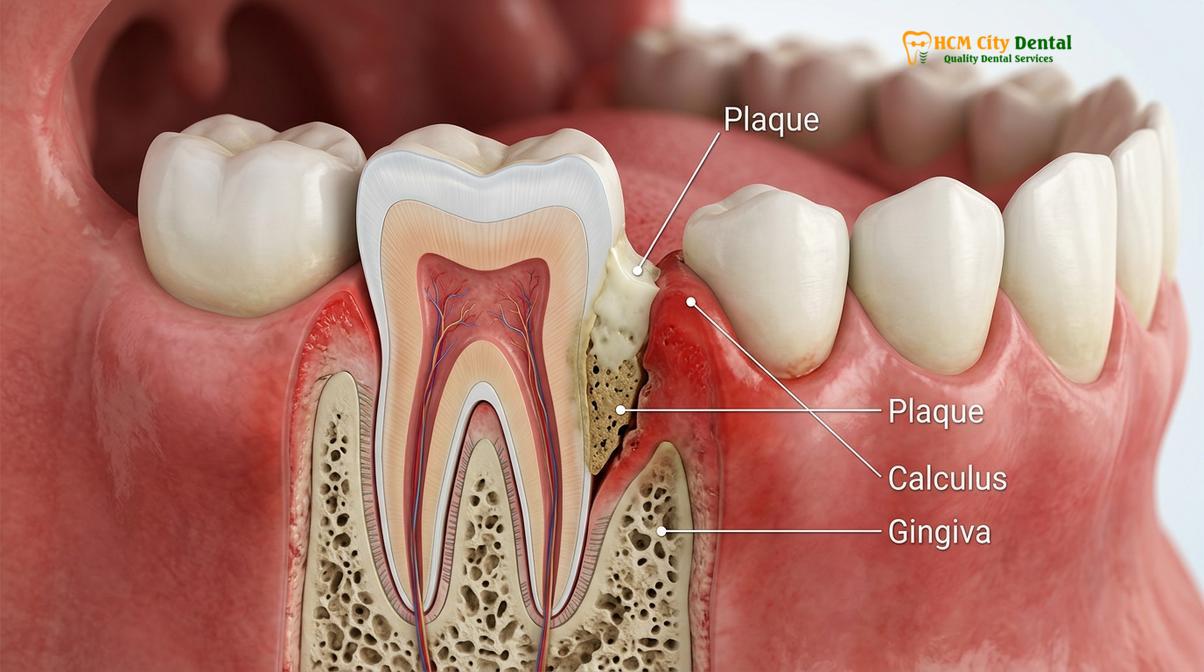
- Periodontal Infections: Gingivitis and periodontitis are major contributors. Deep periodontal pockets provide an anaerobic sanctuary for bacteria like Porphyromonas gingivalis and Treponema denticola. The inflammatory exudate and bleeding gums supply the proteins necessary for massive VSC production.
- Dental Caries and Pulpal Necrosis: Deep, untreated cavities act as food traps. If the decay reaches the dental pulp, the resulting necrotic tissue and periapical abscesses emit a distinctly foul odor.
- Poorly Maintained Prosthetics: Ill-fitting dentures, defective crown margins, and unpolished restorations can harbor plaque. Patients utilizing removable appliances must adhere to strict hygiene protocols; failure to do so allows acrylic resins to absorb odors. Understanding the risks of improper cleaning is vital, which is why professionals often advise against unverified DIY dental tool cleaners.
Extraoral Causes (10% – 15% of Cases)
When a thorough dental examination reveals a healthy oral cavity, the clinician must investigate extraoral sources. These are broadly categorized into respiratory, gastrointestinal, and metabolic disorders.
| Systemic Category | Specific Conditions | Clinical Odor Profile |
|---|---|---|
| Otorhinolaryngological (ENT) | Tonsilloliths (tonsil stones), chronic sinusitis, post-nasal drip, pharyngitis. | Cheesy, putrid odor; often worse upon waking. |
| Gastrointestinal (GI) | GERD, Zenker’s diverticulum, Helicobacter pylori infection, pyloric stenosis. | Acidic, sour, or fecal odor; may worsen after meals. |
| Metabolic / Endocrine | Diabetic ketoacidosis, uremia (renal failure), hepatic encephalopathy. | Fruity/acetone (diabetes), ammoniacal (renal), musty/sweet (hepatic). |
| Pharmacological | Antihistamines, antidepressants, diuretics, chemotherapy agents. | Variable; primarily causes malodor secondary to drug-induced xerostomia. |
According to Dr. Nguyen Van Cuong, a leading specialist at HCMC Dental Clinic, distinguishing between genuine intraoral halitosis and extraoral manifestations is a critical first step in the diagnostic workflow to prevent unnecessary dental treatments and address potential underlying systemic health threats.
Clinical Diagnostic Protocols for Oral Malodor
Dentists diagnose halitosis using organoleptic measurement (direct sniffing) and advanced instrumental analysis like sulfide monitors or gas chromatography to quantify the exact levels of VSCs.
Diagnosing halitosis requires a structured, evidence-based approach. Because self-assessment of breath odor is notoriously unreliable due to olfactory adaptation (the brain’s tendency to ignore continuous stimuli), objective clinical measurement is essential.[3]
Organoleptic Measurement
Despite technological advancements, the organoleptic assessment remains the gold standard for diagnosing halitosis. This involves the clinician directly smelling the patient’s breath. To standardize this subjective process, the Rosenberg scale is commonly utilized, scoring the odor from 0 to 5:
- 0: Absence of odor.
- 1: Questionable odor (barely detectable).
- 2: Slight but clearly noticeable malodor.
- 3: Moderate malodor.
- 4: Strong, offensive malodor.
- 5: Extremely foul, overwhelming malodor.
During this test, the clinician will assess breath expelled from the mouth, breath expelled from the nose, and the odor of a spoon or gauze scraped across the posterior tongue. If the odor is present in mouth-exhaled air but absent in nose-exhaled air, the source is almost certainly intraoral.

Instrumental Analysis
To provide objective, quantifiable data, modern dental clinics employ specialized diagnostic equipment:
- Halimeter (Sulfide Monitoring): This device uses an electrochemical voltammetric sensor to measure the concentration of hydrogen sulfide and methyl mercaptan in parts per billion (ppb). A reading above 100-150 ppb generally indicates clinically significant halitosis.
- Gas Chromatography: This is the most precise method available. It separates the breath sample into its individual chemical components, allowing the clinician to measure the exact concentrations of hydrogen sulfide, methyl mercaptan, and dimethyl sulfide independently. This is particularly useful for distinguishing between intraoral and extraoral causes.
- BANA Test: This microbiological test detects the presence of specific proteolytic enzymes produced by the red complex bacteria (P. gingivalis, T. denticola, T. forsythia), which are heavily implicated in both periodontitis and halitosis.
Proper diagnostics also involve evaluating the integrity of existing dental work. For instance, a patient presenting with a grey tooth may have a necrotic pulp silently leaking malodorous gases into the oral cavity, which would be identified during a comprehensive radiographic examination.
Evidence-Based Treatment Workflows
Managing halitosis requires a combination of professional periodontal therapy, mechanical tongue cleaning, and the use of targeted antimicrobial mouthwashes containing active ingredients like chlorhexidine or zinc.
The treatment of halitosis is highly dependent on the definitive diagnosis. If the etiology is intraoral, the primary objective is to reduce the bacterial load and eliminate the environments where anaerobic bacteria thrive. This is achieved through a phased clinical approach.[4]
Phase 1: Mechanical Debridement and Biofilm Disruption
Mechanical removal of the bacterial biofilm is the cornerstone of halitosis therapy. Professional intervention begins with scaling and root planing to remove calculus and plaque from above and below the gumline. This eliminates the anaerobic pockets that harbor VSC-producing bacteria. Furthermore, any defective restorations that act as plaque traps must be replaced, and active carious lesions must be restored.
Patient education is equally critical in this phase. The clinician must instruct the patient on proper brushing techniques, interdental cleaning (flossing or interdental brushes), and, most importantly, tongue cleaning. Using a dedicated tongue scraper to gently clean the posterior dorsal surface of the tongue is often the single most effective at-home intervention for reducing morning breath.
Phase 2: Chemical Adjuncts
While mechanical cleaning is paramount, chemical adjuncts can significantly enhance the reduction of oral malodor. Therapeutic mouthwashes are formulated to either neutralize VSCs or exert an antimicrobial effect. Active ingredients proven to be effective include:
- Chlorhexidine Gluconate (CHX): A potent broad-spectrum antimicrobial agent that disrupts bacterial cell membranes. It is highly effective but reserved for short-term use due to side effects.
- Cetylpyridinium Chloride (CPC): A quaternary ammonium compound that reduces bacterial plaque and is suitable for longer-term daily use.
- Zinc Ions (Zinc Chloride): Zinc has a high affinity for sulfur. It binds directly to VSCs, converting them into non-volatile, odorless zinc sulfides.
- Chlorine Dioxide: An oxidizing agent that degrades VSCs and alters the anaerobic environment, making it less hospitable for odor-causing bacteria.
Patients often inquire about cosmetic solutions to mask bad breath. While mints and generic mouthwashes offer a temporary masking effect, they do not cure the condition. For patients seeking comprehensive oral care, finding a qualified professional is essential. Reviewing a guide on how to find a good dentist can help patients locate a clinic equipped with the necessary diagnostic tools for halitosis.
The Role of Saliva and Xerostomia in Breath Odor
Saliva acts as a natural cleanser that buffers oral acids and washes away odor-causing bacteria; therefore, conditions causing dry mouth directly amplify the severity of halitosis.
Saliva is the oral cavity’s primary defense mechanism. It possesses mechanical flushing properties that continuously clear food debris and unattached bacteria from the mouth. Furthermore, saliva contains antimicrobial enzymes (like lysozyme and lactoferrin) and acts as a critical buffer, maintaining a neutral pH that inhibits the volatility of sulfur compounds.
Xerostomia, or chronic dry mouth, drastically alters this protective environment. When salivary flow decreases, the oral pH drops, creating an acidic environment that favors bacterial proliferation. The lack of mechanical flushing allows thick, stagnant biofilms to accumulate on the teeth and tongue. Xerostomia can be induced by numerous factors, including:
- Medications: Over 400 commonly prescribed drugs, including antihypertensives, antidepressants, and antihistamines, list dry mouth as a side effect.
- Systemic Diseases: Autoimmune conditions like Sjögren’s syndrome directly attack the salivary glands.
- Lifestyle Factors: Chronic mouth breathing, snoring, and inadequate hydration significantly dry out the oral mucosa.
“The management of halitosis is inextricably linked to the management of salivary flow; without adequate hydration and buffering capacity, mechanical and chemical interventions will ultimately fail to provide long-term relief.”
Managing xerostomia-induced halitosis involves stimulating salivary flow through sugar-free chewing gum, utilizing artificial saliva substitutes, and ensuring adequate systemic hydration. In some cases, adjusting the patient’s oral hygiene products is necessary. For example, understanding the role of various toothpaste ingredients is crucial; patients can consult resources on fluoride facts or seek advice from recommended cosmetic dentists to select non-irritating, hydrating oral care products.
Psychological Dimensions: Halitophobia and Pseudo-Halitosis
Some patients experience severe anxiety over perceived bad breath that does not clinically exist, requiring careful psychological management and reassurance rather than dental intervention.
The clinical management of halitosis is not solely confined to microbiology and biochemistry; it has a profound psychological component. The fear of having bad breath can lead to significant social anxiety, isolation, and obsessive oral hygiene behaviors. Clinicians classify these psychological manifestations into two categories:
Pseudo-halitosis occurs when a patient complains of bad breath, but objective testing (organoleptic and instrumental) reveals no malodor. These patients can usually be successfully managed through education, reassurance, and demonstrating the negative results of the Halimeter tests. Once they understand the science, their anxiety typically subsides.
Halitophobia, however, is a more complex psychiatric condition, often categorized under Olfactory Reference Syndrome. Patients with halitophobia possess a fixed, delusional belief that their breath is offensive, despite repeated objective evidence to the contrary. They often misinterpret the actions of others (e.g., someone rubbing their nose or stepping back) as a reaction to their breath. Dental treatment is contraindicated for halitophobia; instead, compassionate referral to a mental health professional for cognitive behavioral therapy is the standard of care.[5]
When to See a Doctor (Clinical Red Flags)
While occasional morning breath is a normal physiological occurrence, persistent halitosis warrants professional evaluation. Patients should not rely indefinitely on over-the-counter masking agents, as bad breath can be a primary indicator of progressive tissue destruction or systemic illness.
Dr. Cuong advises that if rigorous oral hygiene and professional dental cleanings do not resolve the malodor within a few weeks, a multidisciplinary evaluation is warranted to rule out systemic pathologies. Immediate clinical attention is required if halitosis is accompanied by any of the following red flag symptoms:
- Persistent bleeding or swollen gums, indicating active periodontal infection.
- Purulent discharge (pus) from the gums or a specific tooth, suggesting an acute abscess.
- White patches on the tongue or oral mucosa, which may indicate oral candidiasis (thrush).
- Chronic dry mouth accompanied by difficulty swallowing or speaking.
- Fever, chronic cough, or thick post-nasal drip, pointing toward a respiratory tract infection.
- A sudden, distinct change in breath odor (e.g., smelling like acetone or ammonia), which requires immediate medical referral for potential metabolic crises.

For patients experiencing persistent oral malodor, seeking a comprehensive diagnostic evaluation is the safest course of action. Whether the goal is addressing periodontal health or exploring aesthetic improvements like teeth whitening after resolving the underlying infections, professional guidance ensures safe and effective outcomes.
Frequently Asked Questions
What is the most common cause of halitosis?
The most common cause of halitosis is poor oral hygiene leading to the accumulation of bacterial biofilm on the tongue and teeth. This accounts for approximately 80 to 85 percent of all clinical cases. When food debris and plaque are not effectively removed, anaerobic bacteria proliferate and degrade proteins into volatile sulfur compounds, which produce the characteristic foul odor. Regular brushing, flossing, and tongue scraping are the first lines of defense.
Can gastrointestinal issues cause bad breath?
Yes, gastrointestinal issues can cause bad breath, though they account for a very small percentage of cases. Conditions such as gastroesophageal reflux disease (GERD), hiatal hernias, and Helicobacter pylori infections can allow stomach acids and gases to travel up the esophagus and enter the oral cavity, contributing to extraoral halitosis. If a dentist rules out all oral causes, a referral to a gastroenterologist is typically the next step.
How do dentists objectively measure bad breath?
Dentists objectively measure bad breath using instrumental analysis such as a Halimeter or Gas Chromatography, alongside organoleptic scoring. A Halimeter detects the concentration of volatile sulfur compounds in parts per billion, while Gas Chromatography can isolate and quantify specific gases like hydrogen sulfide and methyl mercaptan, providing a precise clinical diagnosis. This prevents misdiagnosis and helps differentiate between genuine halitosis and halitophobia.
Is mouthwash an effective long-term cure for halitosis?
Mouthwash is not a standalone long-term cure for halitosis; it is a chemical adjunct used alongside mechanical cleaning. While therapeutic rinses containing chlorhexidine or zinc can temporarily neutralize volatile sulfur compounds and reduce bacterial loads, they do not address the root causes such as deep periodontal pockets or chronic tonsillitis. Over-reliance on mouthwash without professional dental care only masks the underlying pathology.
What is halitophobia and how is it treated?
Halitophobia is a psychological condition where a patient genuinely believes they have severe bad breath despite objective clinical evidence proving otherwise. Treatment requires a multidisciplinary approach; after a dentist definitively rules out organic malodor using objective testing, the patient is typically referred to a psychologist or psychiatrist for cognitive behavioral therapy. Dental interventions are generally avoided as they do not resolve the underlying psychological distress.
References
- Journal of the American Dental Association. Halitosis: Prevalence, risk factors, sources, measurement and treatment. (2020).
- StatPearls Publishing. Halitosis: Etiology, Pathophysiology, and Clinical Management. (2023).
- International Journal of Oral Science. The oral microbiome and volatile sulfur compounds in halitosis. (2019).
- Journal of Clinical Periodontology. Efficacy of mechanical and chemical interventions in managing oral malodor. (2021).
- American Academy of Periodontology. The relationship between periodontal disease and halitosis. (2022).