The primary cause of tooth decay is the accumulation of dental plaque, a sticky biofilm of bacteria that feeds on dietary sugars. These bacteria produce lactic acid, which progressively strips essential minerals from the tooth enamel, leading to structural breakdown and the formation of cavities.
Clinical Summary:
Dental caries, commonly known as tooth decay, is a multifactorial infectious disease characterized by the localized destruction of susceptible dental hard tissues. The etiology involves a complex interaction between cariogenic bacteria (primarily Streptococcus mutans and Lactobacillus species), fermentable carbohydrates, and host factors such as salivary flow and tooth anatomy. When bacteria metabolize sugars, they generate organic acids that lower the ambient pH below the critical threshold of 5.5, initiating the demineralization of hydroxyapatite crystals in the enamel. If the rate of demineralization exceeds the natural remineralization capacity of saliva, a carious lesion develops. Clinical management focuses on early detection, risk assessment, remineralization therapies, and restorative interventions to preserve the natural dentition and prevent endodontic complications.
Key Takeaways:
- Tooth decay is primarily caused by acid-producing bacteria thriving in dental plaque.
- Frequent consumption of fermentable carbohydrates accelerates enamel demineralization.
- Saliva plays a critical defensive role by neutralizing acids and supplying remineralizing ions.
- Early-stage decay (white spot lesions) can often be reversed with targeted fluoride therapy.
- Advanced decay requires professional restorative treatments to prevent severe pulpal infection.
The Biological Mechanism: How Tooth Decay Develops
Tooth decay develops through a continuous cycle of demineralization driven by bacterial acids, which eventually overpower the mouth’s natural remineralization process and destroy the tooth structure.
To fully comprehend the cause of tooth decay, one must examine the microscopic biological processes that occur within the oral cavity on a daily basis. The mouth is a complex ecosystem harboring hundreds of bacterial species. While many of these microorganisms are benign or even beneficial, specific strains are highly cariogenic—meaning they have a strong propensity to cause cavities. The development of dental caries is not a sudden event but rather a chronic, progressive shift in the balance between mineral loss (demineralization) and mineral gain (remineralization) at the tooth surface [1].
The Role of Dental Plaque and Cariogenic Bacteria
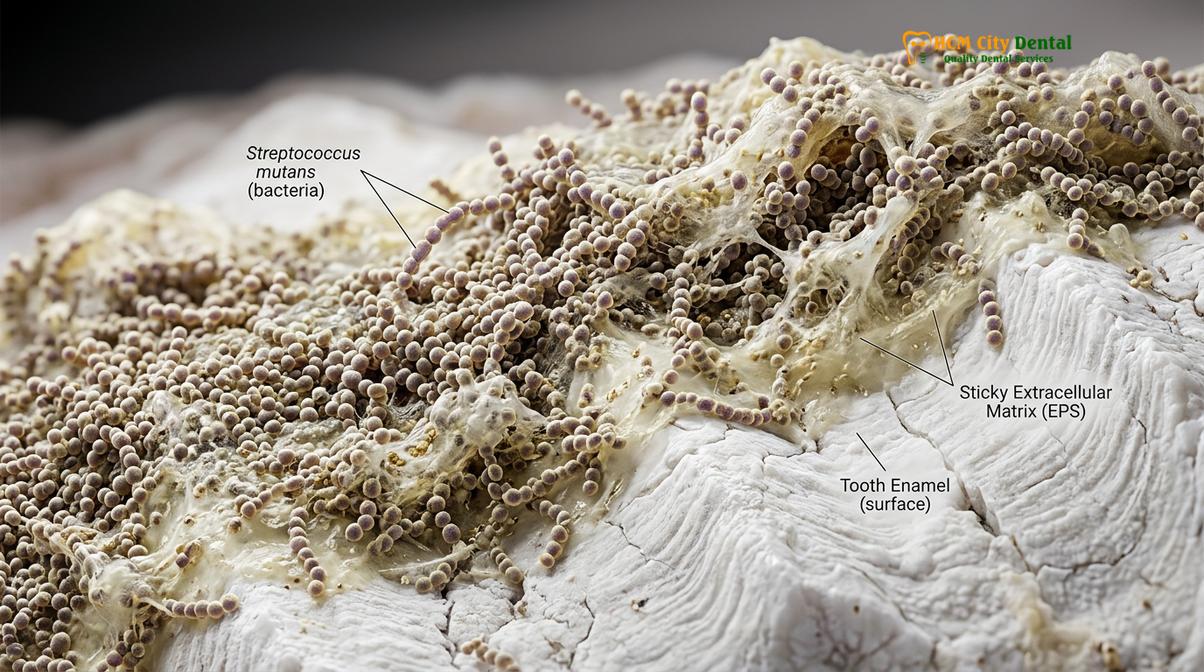
The foundation of tooth decay is dental plaque. Plaque is a dense, sticky, and colorless biofilm that constantly forms on the teeth. The formation of plaque begins mere minutes after brushing, starting with the deposition of a salivary pellicle—a thin protein layer that coats the enamel. This pellicle acts as a biological adhesive, allowing primary bacterial colonizers to attach to the tooth surface.
Among these colonizers, Streptococcus mutans is the most notorious culprit in the initiation of dental caries. As the biofilm matures, it creates an anaerobic environment that favors the growth of aciduric (acid-tolerating) and acidogenic (acid-producing) bacteria, including various Lactobacillus species. These bacteria are uniquely adapted to survive in highly acidic environments, giving them a competitive advantage over healthier oral flora. When a patient consumes foods or beverages containing fermentable carbohydrates, these bacteria rapidly metabolize the sugars, utilizing them as an energy source and producing organic acids—predominantly lactic acid—as a metabolic byproduct [2].
Acid Production and Enamel Demineralization
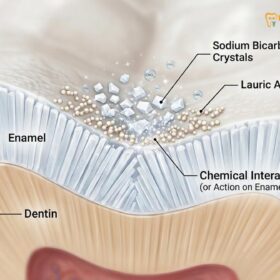
The human tooth is covered by enamel, the hardest substance in the body, composed of approximately 96% inorganic minerals, primarily in the form of hydroxyapatite crystals. Despite its remarkable strength, enamel is highly vulnerable to chemical dissolution by acids. The critical pH for enamel demineralization is generally accepted to be 5.5. When the pH of the plaque biofilm drops below this threshold due to bacterial acid production, the hydrogen ions begin to dissolve the calcium and phosphate minerals from the hydroxyapatite crystal structure.
This phenomenon is clinically described by the Stephan Curve, which illustrates the rapid drop in plaque pH following sugar exposure, followed by a slow recovery period. If sugar consumption is infrequent, the saliva has sufficient time to buffer the acids, raise the pH, and redeposit calcium and phosphate back into the enamel—a process known as remineralization. However, if the frequency of sugar intake is high, the plaque pH remains chronically depressed. The continuous acid attack overwhelms the remineralization capacity of the saliva, leading to a net loss of minerals. Over time, this subsurface demineralization weakens the structural integrity of the enamel, eventually causing it to collapse and form a macroscopic cavity.
“Dental caries is fundamentally a disease of ecological imbalance. It is not merely the presence of bacteria that causes decay, but rather the environmental shift driven by frequent carbohydrate exposure that allows acid-producing strains to dominate the biofilm and dismantle the tooth’s mineral defenses.”
Primary Causes and Contributing Risk Factors
Beyond bacterial plaque, the primary causes of tooth decay include frequent consumption of sugary foods, poor oral hygiene, and systemic conditions that reduce protective salivary flow.
While the biological mechanism of acid demineralization is the direct cause of tooth decay, numerous behavioral, environmental, and physiological factors significantly influence an individual’s susceptibility to the disease. Understanding these risk factors is essential for developing comprehensive general dentistry protocols aimed at effective prevention and management.
Dietary Habits and Fermentable Carbohydrates
Diet plays an undeniable role in the etiology of dental caries. However, it is not just the total amount of sugar consumed that dictates the risk, but rather the frequency of consumption and the physical consistency of the food. Sucrose (table sugar) is widely considered the most cariogenic carbohydrate because it is easily metabolized by bacteria and is utilized by Streptococcus mutans to synthesize extracellular polysaccharides. These sticky polymers act like a glue, thickening the plaque biofilm, increasing its adherence to the tooth, and restricting the diffusion of neutralizing saliva into the plaque matrix.
Frequent snacking or continuous sipping of sugary or acidic beverages (such as sodas, sports drinks, and sweetened coffees) keeps the oral environment in a constant state of acidity. Furthermore, sticky foods like dried fruits, caramels, and gummy candies adhere to the tooth surfaces for prolonged periods, providing a sustained food source for cariogenic bacteria. Even complex carbohydrates, such as potato chips and crackers, can be broken down into simple sugars by salivary amylase, contributing to the acidogenic challenge.
Clinical Warning: “Baby bottle tooth decay” is a severe form of early childhood caries caused by allowing an infant to sleep with a bottle containing milk, formula, or juice. The pooling of sugary liquids around the teeth during sleep, combined with reduced salivary flow, can cause rapid and devastating destruction of the primary dentition.
Salivary Flow and Dry Mouth (Xerostomia)
Saliva is the mouth’s primary natural defense mechanism against tooth decay. It performs several critical functions: it mechanically washes away food debris and unattached bacteria; it contains antimicrobial agents (such as lysozyme and lactoferrin) that inhibit bacterial growth; and most importantly, it acts as a powerful buffering agent. Saliva is supersaturated with calcium and phosphate ions, which are essential for repairing early demineralized lesions [3].
When salivary flow is compromised—a condition known as xerostomia or dry mouth—the risk of rampant tooth decay increases exponentially. Xerostomia can be caused by various factors, including the use of certain medications (such as antihistamines, antidepressants, and antihypertensives), systemic autoimmune conditions like Sjögren’s syndrome, or radiation therapy to the head and neck region. Without the protective benefits of saliva, even minor dietary indiscretions can lead to aggressive cavity formation.
Anatomical Vulnerabilities and Tooth Location
The physical anatomy of the teeth also dictates their susceptibility to decay. The posterior teeth (molars and premolars) are at a significantly higher risk of developing cavities compared to the anterior (front) teeth. This is due to the complex morphology of their occlusal (chewing) surfaces, which feature deep pits, fissures, and developmental grooves. These microscopic crevices are often narrower than a single toothbrush bristle, making them virtually impossible to clean thoroughly. Consequently, they serve as ideal retentive areas for food particles and plaque biofilm to accumulate undisturbed.
Additionally, systemic conditions that introduce intrinsic acids into the oral cavity can severely erode enamel, making it more susceptible to bacterial decay. Gastroesophageal reflux disease (GERD) and eating disorders involving frequent vomiting (such as bulimia nervosa) expose the teeth to highly corrosive stomach acid. This chemical erosion strips away the protective enamel layer, exposing the softer underlying dentin and dramatically accelerating the clinical management of dental caries.
The Five Clinical Stages of Dental Caries
Dental caries progresses through five distinct stages, beginning with reversible white spot lesions and advancing to severe pulpal infection if left untreated.
Tooth decay is not a static condition; it is a dynamic and progressive disease. If the causative factors are not addressed, the lesion will advance deeper into the tooth structure. Clinicians categorize the progression of dental caries into distinct stages, each requiring a different therapeutic approach.
From Initial Demineralization to Pulpal Necrosis
The progression of a cavity follows a predictable anatomical path, moving from the highly mineralized outer enamel to the sensitive inner tissues of the tooth. Understanding these stages is crucial for timely intervention.
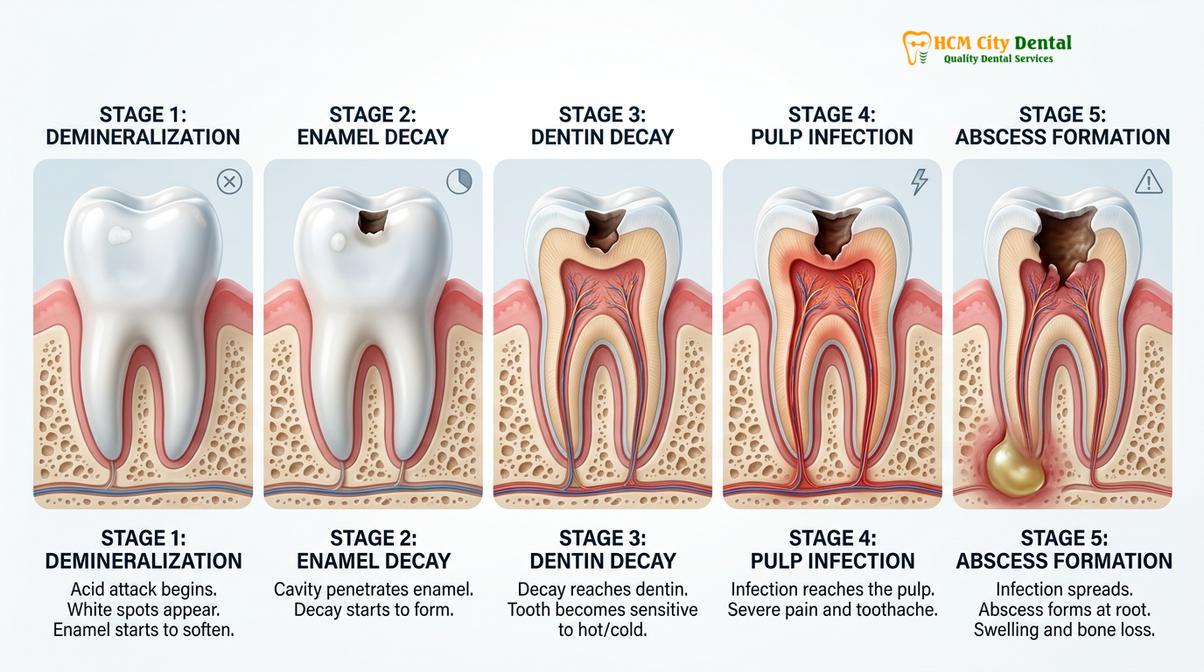
- Stage 1: Initial Demineralization (White Spot Lesion): The earliest sign of tooth decay is the appearance of a chalky white spot on the enamel surface. This opacity indicates subsurface mineral loss. At this stage, the enamel surface remains intact (non-cavitated). Crucially, this stage is entirely reversible. With the application of topical fluoride and improved oral hygiene, the lost minerals can be replaced, arresting the decay process.
- Stage 2: Enamel Cavitation: If demineralization continues, the weakened enamel structure eventually collapses, creating a physical hole or micro-cavity. The lesion may take on a brown or black appearance as it absorbs pigments from food and beverages. At this point, the decay is irreversible, and the tooth cannot heal itself. Professional restorative treatment is required to remove the diseased tissue and seal the tooth.
- Stage 3: Dentin Involvement: Once the decay breaches the enamel-dentin junction (EDJ), it enters the dentin layer. Dentin is significantly softer and more porous than enamel, containing thousands of microscopic tubules that communicate directly with the dental pulp. Because of this tubular structure, decay spreads much more rapidly in dentin. Patients often begin to experience sensitivity to sweet, hot, or cold stimuli at this stage due to fluid movement within the dentinal tubules (the hydrodynamic theory of tooth sensitivity) [4].
- Stage 4: Pulpal Involvement (Pulpitis): If the dentinal decay is left untreated, the bacterial infection will eventually reach the dental pulp—the innermost chamber of the tooth containing nerves, blood vessels, and connective tissue. The invasion of bacteria triggers an intense inflammatory response known as pulpitis. Because the pulp is encased in rigid tooth structure, the swelling causes severe pressure and excruciating, spontaneous pain. This stage typically requires endodontic therapy (root canal treatment) to salvage the tooth.
- Stage 5: Abscess Formation and Necrosis: In the final stage, the pulpal tissue undergoes necrosis (death) due to overwhelming infection and lack of blood supply. The bacteria and their toxic byproducts exit the tip of the tooth root (the apex) and invade the surrounding alveolar bone, forming a periapical abscess. This can cause severe facial swelling, systemic fever, and potentially life-threatening complications if the infection spreads to fascial spaces. Extraction or complex endodontic retreatment is often the only recourse.
| Stage of Decay | Clinical Presentation | Typical Treatment Protocol |
|---|---|---|
| 1. Demineralization | Chalky white spots, intact surface | Fluoride varnish, CPP-ACP, hygiene instruction |
| 2. Enamel Cavitation | Small physical hole, dark staining | Conservative composite resin restoration |
| 3. Dentin Decay | Larger cavity, thermal/sweet sensitivity | Deep composite filling, inlay, or onlay |
| 4. Pulpitis | Spontaneous throbbing pain, lingering sensitivity | Root canal therapy and dental crown |
| 5. Abscess | Facial swelling, severe pain on biting, pus | Root canal therapy, antibiotics, or extraction |
Diagnostic Protocols and Treatment Workflows
Clinical treatment for tooth decay ranges from non-invasive fluoride remineralization for early lesions to complex restorative or endodontic procedures for advanced structural damage.
Accurate diagnosis is the cornerstone of effective caries management. Modern dentistry employs a combination of visual inspection, tactile examination using a dental explorer, and advanced imaging technologies. Digital bitewing radiographs are indispensable for detecting interproximal decay (cavities between the teeth) that cannot be seen with the naked eye. Additionally, clinicians may utilize laser fluorescence devices (such as DIAGNOdent) or transillumination to detect early demineralization hidden within deep occlusal fissures.
Early Detection and Remineralization Strategies
When tooth decay is detected in its incipient stage (Stage 1), the primary goal is to halt the progression and encourage remineralization. This non-invasive approach relies heavily on fluoride therapy. Professional application of high-concentration fluoride varnishes (typically 5% sodium fluoride) creates a temporary reservoir of calcium fluoride on the tooth surface. As the pH drops during an acid attack, this reservoir releases fluoride ions, which integrate into the enamel structure to form fluorapatite—a mineral compound that is significantly more resistant to acid dissolution than natural hydroxyapatite [5].
In addition to fluoride, clinicians may prescribe remineralizing pastes containing Casein Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP) to provide the necessary building blocks for enamel repair. Dietary counseling is also a critical component of this phase, educating patients on reducing the frequency of fermentable carbohydrate intake.
“The paradigm of caries management has shifted from a purely surgical approach—’drill and fill’—to a medical model focused on risk assessment, early detection, and the biochemical remineralization of early lesions before irreversible cavitation occurs.”
Restorative Interventions (Fillings and Crowns)
Once cavitation has occurred (Stages 2 and 3), surgical intervention is necessary to remove the infected tooth structure and restore the tooth’s form, function, and aesthetics. The standard workflow involves administering local anesthesia, isolating the tooth (often using a rubber dam to prevent salivary contamination), and meticulously excavating the decayed enamel and dentin using high-speed and low-speed handpieces.
For small to moderate cavities, direct composite resin restorations are the material of choice. The preparation is treated with a mild etchant to create microscopic pores in the enamel and dentin. A bonding agent is then applied and cured, forming a hybrid layer that securely anchors the composite resin to the tooth. The resin is placed in increments, sculpted to match the natural tooth anatomy, and polymerized using a specialized curing light.

If the decay is extensive and has compromised a significant portion of the tooth structure, a direct filling may not provide adequate strength. In such cases, indirect restorations like inlays, onlays, or full-coverage dental crowns are indicated. These restorations are custom-fabricated in a dental laboratory or milled in-office using CAD/CAM technology. For patients missing teeth due to severe decay, fixed dental bridge restorations or implants may be required to restore the dental arch.
Clinical Case Review: A 28-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City complaining of severe sensitivity in a lower right molar. Clinical examination by Dr. Nguyen Van Cuong revealed deep occlusal decay that had penetrated the dentin but had not yet reached the pulp. Dr. Cuong utilized a conservative preparation technique to remove the infected tissue, preserving as much healthy tooth structure as possible. The tooth was successfully restored with a biomimetic composite onlay, immediately resolving the patient’s symptoms and preventing the need for a root canal.
Advanced Endodontic Therapy
When the cariogenic bacteria breach the pulp chamber (Stage 4), restorative dentistry alone is insufficient. The infected pulpal tissue must be entirely removed through endodontic therapy (root canal treatment). This intricate procedure involves accessing the pulp chamber, navigating the complex root canal anatomy, and mechanically cleaning and chemically disinfecting the canals using sodium hypochlorite and other irrigants. Once sterilized, the canals are obturated (filled) with a biocompatible material called gutta-percha to seal the space and prevent reinfection.
Teeth that have undergone root canal therapy become brittle over time due to the loss of blood supply and internal moisture. Therefore, it is generally recommended to protect endodontically treated posterior teeth with a full-coverage crown to prevent catastrophic vertical root fractures. In cases where the decay is so profound that the tooth is deemed non-restorable, extraction is the final option. This is frequently seen in impacted third molars, where poor accessibility leads to rampant decay, necessitating wisdom teeth extraction procedures.
It is also worth noting that general dentists frequently encounter complex cases where severe decay has altered the patient’s bite or caused adjacent teeth to shift. In such scenarios, comprehensive treatment planning is essential. Many practitioners pursue advanced orthodontic training for general dentists to better understand the biomechanical relationship between restorative interventions and overall occlusal harmony.
When to See a Doctor
While early-stage tooth decay is often asymptomatic, it is crucial not to wait for pain before seeking professional care. Regular biannual dental check-ups are essential for detecting cavities in their incipient, reversible stages. However, you should schedule an immediate clinical evaluation if you experience any of the following symptoms:
- Spontaneous, unprovoked toothache that throbs or keeps you awake at night.
- Sharp, lingering pain when consuming hot, cold, or sweet foods and beverages.
- Visible holes, dark brown pits, or black staining on the surfaces of your teeth.
- Pain when biting down or applying pressure to a specific tooth.
- Swelling in your gums, cheek, or jaw, which may indicate a severe periapical abscess.
If you are experiencing evaluating unexplained tooth pain, prompt intervention is critical to saving the tooth. At HCMC Dental Clinic in Ho Chi Minh City, Dr. Nguyen Van Cuong and the clinical team utilize advanced diagnostic imaging to accurately assess the extent of the decay and formulate a personalized, evidence-based treatment plan designed to restore your oral health efficiently and comfortably.

Frequently Asked Questions
What is the main cause of tooth decay?
The main cause of tooth decay is the accumulation of bacterial plaque that feeds on dietary sugars to produce enamel-destroying acids. Over time, this continuous acid attack depletes the tooth of essential minerals, leading to structural cavitation. Maintaining strict oral hygiene disrupts this biofilm.
Can early tooth decay be reversed?
Yes, early tooth decay in the demineralization stage can often be reversed. Through targeted fluoride therapy, improved oral hygiene, and dietary modifications, the enamel can remineralize before a physical cavity forms. Once a physical hole (cavitation) appears, professional restoration is required.
Why do some people get more cavities despite brushing?
Genetics, salivary flow rates, and tooth anatomy significantly influence cavity risk. Individuals with deep molar fissures, dry mouth conditions, or a highly acidic oral microbiome may experience more decay despite maintaining standard brushing habits. Personalized preventive strategies are necessary for high-risk patients.
How does dry mouth contribute to tooth decay?
Dry mouth accelerates tooth decay because there is insufficient saliva to wash away food particles and neutralize bacterial acids. Saliva also provides the calcium and phosphate necessary for the natural remineralization of tooth enamel. Without it, the teeth are highly vulnerable to rapid demineralization.
Is tooth decay contagious?
The bacteria that cause tooth decay, primarily Streptococcus mutans, can be transmitted between individuals. Sharing utensils or kissing can transfer these cariogenic bacteria, potentially increasing the cavity risk for the recipient, especially in infants whose oral microbiome is still developing.
References
- Journal of Dental Research. The role of Streptococcus mutans and biofilm dynamics in dental caries. (2020).
- American Dental Association. Clinical guidelines on caries risk assessment and evidence-based management. (2021).
- International Journal of Dentistry. Salivary buffering capacity and its impact on enamel demineralization kinetics. (2019).
- Journal of Endodontics. Progression of dental caries to pulpal necrosis: histological and clinical perspectives. (2022).
- Clinical Oral Investigations. Efficacy of fluoride varnishes and remineralization agents in arresting early enamel lesions. (2018).