The primary difference between a root canal and a filling lies in the depth of tooth decay. A filling repairs superficial damage in the enamel or dentin, whereas a root canal treats severe infection that has penetrated the innermost pulp tissue and nerve of the tooth.
Clinical Summary:
When evaluating a root canal vs filling, dental professionals assess the extent of bacterial penetration within the tooth structure. Dental fillings are conservative treatments designed to restore teeth affected by early to moderate decay, specifically when the damage is confined to the outer enamel and the underlying dentin layers. This procedure involves removing the decayed tissue and sealing the cavity with materials like composite resin, leaving the tooth’s internal nerve intact and vital. Conversely, root canal therapy is an advanced endodontic intervention required when caries or trauma breaches the pulp chamber, leading to irreversible pulpitis or pulpal necrosis. This complex procedure necessitates the complete extirpation of the infected nerve tissue, meticulous disinfection of the root canal system, and hermetic obturation to prevent reinfection. Accurate diagnosis relies on clinical symptom analysis, vitality testing, and radiographic imaging to determine the appropriate restorative pathway and preserve the natural dentition.
Key Takeaways:
- Depth of Decay: Fillings treat superficial cavities in the enamel and dentin, while root canals address deep infections inside the pulp chamber.
- Symptom Variations: Mild sensitivity usually indicates a filling is needed, whereas severe, lingering, or spontaneous throbbing pain points toward a root canal.
- Procedure Complexity: A filling is a straightforward, single-visit procedure; endodontic therapy is a meticulous, multi-step process that may require multiple appointments.
- Tooth Vitality: A filling preserves the living nerve of the tooth, while a root canal removes the necrotic or inflamed nerve to eliminate infection.
- Post-Treatment Restoration: Teeth with fillings are immediately functional, whereas endodontically treated teeth typically require a protective dental crown to prevent structural fracture.
The Pathogenesis of Dental Caries: From Surface to Pulp
Dental caries begin as superficial enamel demineralization, which can be treated with a filling, but if left unchecked, the bacteria will eventually breach the dentin and infect the pulp, necessitating endodontic therapy.
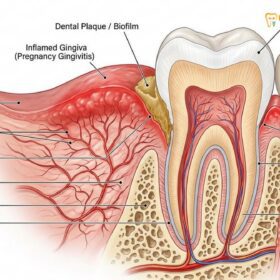
To fully understand the clinical distinction between a root canal vs filling, it is essential to first comprehend the anatomical structure of a human tooth and the biological progression of dental caries (tooth decay). A tooth is not a solid block of bone; rather, it is a complex, multi-layered organ with a distinct histology. The outermost layer is the enamel, the hardest substance in the human body, composed primarily of highly mineralized hydroxyapatite crystals. Beneath the enamel lies the dentin, a softer, porous tissue containing microscopic tubules that communicate directly with the tooth’s core. At the very center of the tooth is the pulp chamber and root canal system, which houses the vital dental pulp—a delicate matrix of nerves, blood vessels, and connective tissue that provides sensory function and nourishment during the tooth’s development.
The pathogenesis of dental caries is a dynamic, bacteria-driven process. When fermentable carbohydrates from the diet are metabolized by cariogenic bacteria (such as Streptococcus mutans) in the oral cavity, they produce organic acids. These acids lower the local pH, leading to the demineralization of the enamel surface. In its earliest stages, this demineralization presents as a non-cavitated white spot lesion. If the acidic environment persists, the enamel structure collapses, forming a physical cavity. At this stage, the decay is superficial, and the tooth’s vital pulp remains healthy and unaffected. This is the precise clinical window where a standard dental filling is highly effective. By excavating the diseased enamel and sealing the defect, the dentist halts the progression of the disease and restores the tooth’s structural integrity.
However, if the initial cavity is neglected, the bacterial biofilm advances deeper into the tooth, penetrating the dentinoenamel junction (DEJ) and invading the dentin. Because dentin is less mineralized and highly porous, decay spreads much more rapidly through this layer. As bacteria and their acidic byproducts travel through the dentinal tubules toward the pulp, the nerve begins to react. This initial inflammatory response is known as reversible pulpitis, characterized by transient sensitivity to cold or sweet stimuli. A prompt filling at this stage can still save the nerve. But if the bacterial invasion breaches the pulp chamber, the inflammation becomes severe and irreversible. The confined space of the pulp chamber cannot accommodate the swelling tissue, leading to intense pressure, excruciating pain, and eventually, the strangulation and death of the nerve tissue (pulpal necrosis) [1]. Once the pulp is irreversibly damaged or necrotic, a filling is no longer a viable medical option, and specialized endodontic therapy becomes an absolute necessity to prevent the infection from spreading into the surrounding alveolar bone.
Dental Fillings: Clinical Scope and Restorative Workflow
A dental filling is a conservative restorative procedure designed to halt early-to-moderate decay within the enamel and dentin layers, restoring the tooth’s structural integrity without accessing the nerve.
A dental filling is the cornerstone of conservative restorative dentistry. Its primary objective is to intercept the disease process before it can compromise the vitality of the tooth. Fillings are indicated for the treatment of primary caries (new cavities), secondary caries (decay around existing restorations), minor structural fractures, and non-carious cervical lesions such as abrasion or erosion. The fundamental philosophy behind this treatment is maximum preservation of healthy tooth structure while completely eradicating the diseased tissue.
The clinical workflow for placing a modern dental filling is a highly precise, technique-sensitive process, particularly when utilizing advanced tooth-colored materials like composite resin. The procedure begins with the administration of local anesthesia to ensure patient comfort. Once the tooth is profoundly numb, the clinician isolates the operative field. Isolation is critical; many modern restorative materials are highly sensitive to moisture, and contamination from saliva or respiratory humidity can severely compromise the bond strength and longevity of the filling. Following isolation, the dentist utilizes high-speed rotary instruments equipped with diamond or carbide burs to meticulously excavate the carious tissue. The goal is to remove all soft, infected dentin while preserving as much of the hard, healthy tooth structure as possible.
“Conservative dentistry prioritizes the early detection and minimally invasive treatment of carious lesions. By intervening at the enamel or superficial dentin level with high-quality restorative materials, we preserve the tooth’s natural biomechanics and vitality, significantly reducing the future need for complex endodontic interventions.”
Once the cavity preparation is clean and verified to be free of decay, the restorative phase begins. Historically, dental amalgam (a mixture of silver, tin, copper, and mercury) was the material of choice due to its durability and moisture tolerance. However, modern dentistry has largely shifted toward composite resins—a sophisticated blend of acrylic plastics and glass or quartz fillers. Composite resins offer superior aesthetics, as they can be precisely shade-matched to the natural tooth, and they bond micro-mechanically to the tooth structure, providing additional reinforcement [2].
The bonding protocol for composite fillings involves several meticulous steps. First, the prepared enamel and dentin are treated with a mild phosphoric acid etchant. This process, known as acid etching, creates microscopic porosities in the tooth surface and removes the smear layer (a layer of debris left by the dental drill). Next, a liquid bonding agent (adhesive) is applied and cured with a specialized blue light. This adhesive flows into the microscopic porosities, creating a hybrid layer that locks the restorative material to the tooth. Finally, the composite resin is placed into the cavity in small increments. Each increment is individually light-cured to minimize polymerization shrinkage—a phenomenon where the material contracts slightly as it hardens, which can lead to marginal gaps and post-operative sensitivity. After the cavity is fully filled, the dentist shapes the material to match the natural anatomical contours of the tooth, adjusts the patient’s bite to ensure proper occlusion, and polishes the restoration to a high gloss, rendering it virtually seamless with the surrounding enamel.

Root Canal Therapy: Advanced Endodontic Intervention
Root canal treatment is an advanced endodontic procedure required when bacterial infection reaches the dental pulp, involving the complete removal of necrotic tissue, disinfection of the canal system, and hermetic sealing.
When evaluating a root canal vs filling, it is crucial to understand that endodontic therapy is not merely a deeper filling; it is a fundamentally different medical procedure aimed at treating infection within the body’s tissues. Root canal therapy, formally known as endodontic treatment, is indicated when the dental pulp becomes irreversibly inflamed (irreversible pulpitis) or completely necrotic (dead) due to deep decay, repeated dental procedures, structural cracks, or traumatic injury. If left untreated, the bacteria within the necrotic pulp will migrate through the root apex (the tip of the root) and invade the periapical tissues, leading to the formation of a dental abscess, localized bone destruction, and potentially severe systemic complications.
The objective of a clinical root canal treatment is to meticulously clean out the infected pulp chamber and the intricate network of root canals, disinfect the hollowed-out space, and seal it completely to prevent bacterial recolonization. This procedure allows the patient to retain their natural tooth structure and root system, maintaining normal chewing function and preventing the jawbone resorption that typically follows a tooth extraction.
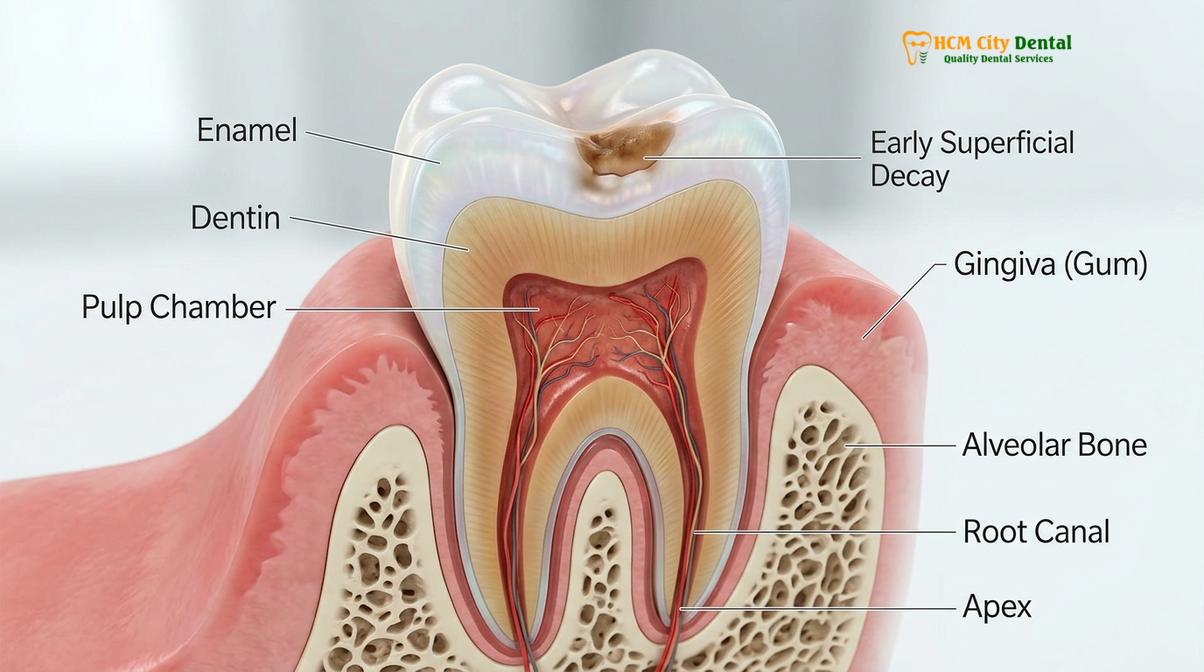
The endodontic workflow is highly complex and requires specialized instruments and profound anatomical knowledge. Dr. Nguyen Van Cuong, a leading expert in restorative and endodontic care, emphasizes that modern root canal therapy relies heavily on advanced technology to ensure high success rates and patient comfort. The procedure begins with profound local anesthesia. Because an infected tooth can sometimes be difficult to numb due to the acidic environment created by the infection, specialized anesthetic techniques, such as intraligamentary or intraosseous injections, may be employed to ensure the patient feels absolutely no pain during the procedure.
Once the tooth is anesthetized, a rubber dam is placed. In endodontics, the rubber dam is not optional; it is a strict standard of care. It prevents the harsh chemical irrigants used to clean the tooth from entering the patient’s mouth and, more importantly, prevents the bacteria in the patient’s saliva from contaminating the sterile root canal system. The dentist then creates an access cavity through the biting surface of the tooth to reach the pulp chamber. Using specialized endodontic instruments, including microscopic hand files and engine-driven nickel-titanium (NiTi) rotary files, the clinician carefully extirpates (removes) the diseased nerve tissue [3].
The next phase is biomechanical preparation. The root canals are not simple, straight tubes; they are complex, branching networks with microscopic fins and lateral canals. The rotary files are used to shape the main canals, while powerful chemical irrigants—primarily sodium hypochlorite (bleach) and EDTA (ethylenediaminetetraacetic acid)—are continuously flushed through the system. These chemicals dissolve organic tissue remnants, kill obligate anaerobic bacteria, and remove the smear layer from the canal walls. This chemical disinfection is arguably the most critical step in ensuring the long-term success of the specialized endodontic therapy.
Once the canal system is thoroughly cleaned, shaped, and dried, it must be obturated (filled and sealed). The standard material for obturation is gutta-percha, a biocompatible, rubber-like material derived from the sap of certain tropical trees. The gutta-percha cones are coated with an antimicrobial sealer cement and compacted tightly into the root canals, extending precisely to the root apex. This creates a hermetic seal that entomb any remaining microscopic bacteria and prevents new bacteria from entering. Finally, a temporary or permanent filling is placed in the access cavity to seal the coronal (top) portion of the tooth, completing the step-by-step root canal procedure.
Root Canal vs Filling: A Comprehensive Clinical Comparison
While both procedures aim to save the natural tooth, fillings address superficial structural damage, whereas root canals resolve deep internal infections and require more complex, multi-step endodontic protocols.
Understanding the precise differences between a root canal vs filling empowers patients to make informed decisions about their oral health. While both are restorative procedures designed to salvage a compromised tooth, their clinical indications, procedural complexity, and long-term management strategies differ significantly. A filling is a structural repair; a root canal is an infection management protocol combined with a structural repair.
To provide clear clinical clarity, the following table outlines the primary distinctions between the two treatments across several critical medical parameters:
| Clinical Parameter | Dental Filling | Root Canal Therapy |
|---|---|---|
| Depth of Pathology | Confined to the outer enamel and underlying dentin layers. | Penetration into the deep pulp chamber and root canal system. |
| Tooth Vitality | Preserves the living nerve and blood supply of the tooth. | Removes the necrotic or irreversibly inflamed nerve tissue. |
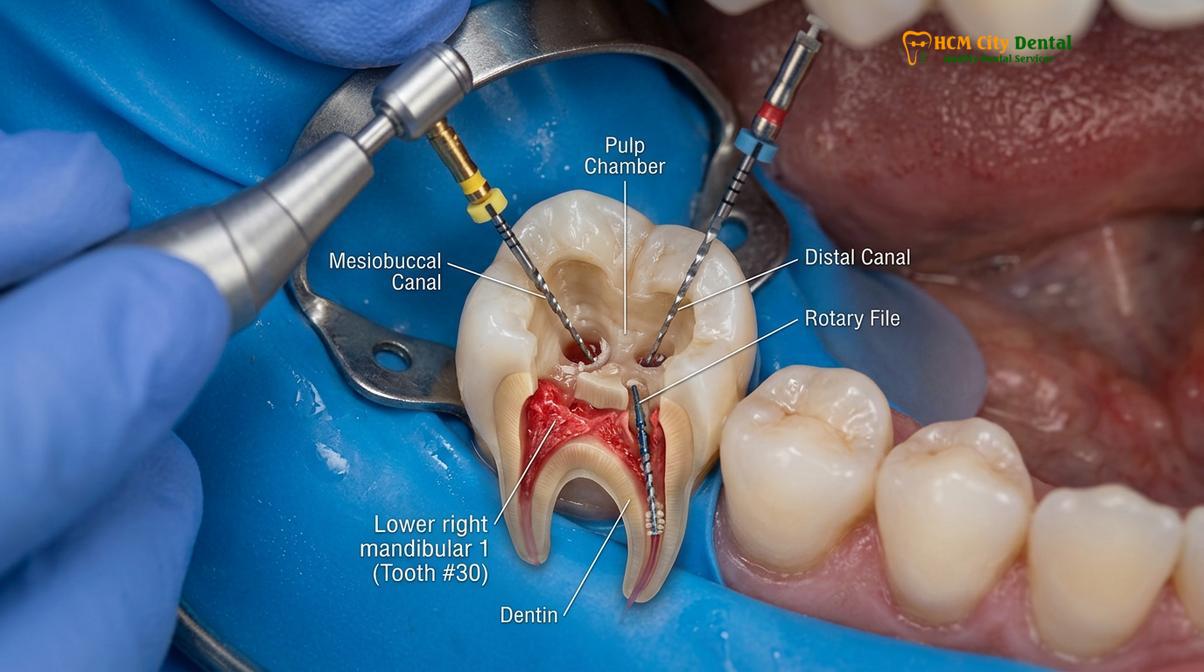
| Primary Symptoms | Mild to moderate sensitivity to cold, heat, or sweet stimuli; localized pain when chewing. | Severe, spontaneous throbbing pain; lingering pain after thermal stimulus; swelling; nocturnal pain. |
| Procedural Time | Typically completed in a single visit lasting 30 to 60 minutes. | Often requires 90 to 120 minutes, potentially spanning one to two appointments. |
| Anesthesia Required | Standard local infiltration or nerve block; sometimes optional for very shallow lesions. | Profound local anesthesia is mandatory; specialized injection techniques may be required. |
| Post-Op Restoration | The filling itself is the final restoration; tooth is immediately functional. | Requires a core build-up and typically a full-coverage dental crown for structural protection. |
One of the most common patient concerns when comparing these procedures is the anticipation of pain. There is a pervasive, outdated stigma that root canals are excruciatingly painful. In modern clinical practice, this is a misconception. The severe pain patients associate with a root canal is actually the pain of the acute pulpal infection that precedes the treatment. The procedure itself, performed under profound local anesthesia, is designed to eliminate that pain. From a sensory perspective during the procedure, receiving a root canal feels very similar to receiving a deep filling—the patient will feel pressure and vibration, but no sharp pain [4]. If a tooth is deemed unsalvageable due to massive structural loss or vertical root fracture, the clinician may need to discuss comparing root canal therapy to extraction, though preservation of the natural tooth is always the primary medical goal.
Diagnostic Methodologies: Determining the Appropriate Treatment
Dentists utilize a combination of patient symptom history, thermal and electrical vitality testing, and high-resolution radiographic imaging to accurately diagnose whether a tooth requires a simple filling or a complex root canal.
The decision to perform a root canal vs filling is not arbitrary; it is based on a rigorous diagnostic protocol. When a patient presents with tooth pain, the clinician must act as a diagnostician, gathering subjective symptoms and objective clinical data to determine the exact status of the dental pulp. At HCMC Dental Clinic in Ho Chi Minh City, comprehensive diagnostic evaluations are the foundation of successful restorative outcomes.
The diagnostic process begins with a detailed patient history. The nature of the pain provides critical clues. If a patient reports that their tooth hurts only when they drink ice water, and the pain subsides immediately after the cold stimulus is removed, this typically indicates reversible pulpitis—a condition that can usually be resolved with a standard filling. However, if the patient reports that the pain lingers for minutes or hours after a hot or cold stimulus, wakes them up in the middle of the night, or occurs spontaneously without any trigger, this strongly suggests irreversible pulpitis or pulpal necrosis, mandating endodontic therapy.
Clinical Case Review: Diagnostic Differentiation
A 34-year-old patient visited HCMC Dental Clinic in Ho Chi Minh City complaining of severe, localized pain in the lower right quadrant. The patient assumed they needed a simple filling for a visible cavity. However, clinical diagnostics revealed a different reality. Thermal testing with Endo-Ice produced a severe, lingering pain response lasting over 60 seconds, indicative of irreversible pulpitis. Furthermore, percussion testing (gently tapping the tooth) elicited sharp pain, suggesting the inflammation had spread to the periapical tissues surrounding the root tip. Radiographic imaging confirmed a deep carious lesion communicating directly with the pulp chamber. Based on these objective findings, Dr. Cuong diagnosed the tooth with irreversible pulpitis and symptomatic apical periodontitis. A simple filling would have sealed the infection inside, leading to a severe abscess. Instead, a successful single-visit root canal was performed, immediately resolving the patient’s pain and saving the natural tooth structure.
Following the symptom history, the dentist performs objective clinical tests. Thermal testing, usually utilizing a specialized refrigerant spray (Endo-Ice), assesses the nerve’s response to cold. Electric Pulp Testing (EPT) delivers a mild electrical current to the tooth to determine if the nerve fibers are still capable of conducting signals. Percussion testing involves gently tapping the tooth with the handle of a dental mirror; a painful response indicates inflammation in the periodontal ligament at the root apex, a classic sign of endodontic pathology.
Radiographic imaging is the final, indispensable diagnostic tool. High-resolution digital X-rays, and increasingly Cone Beam Computed Tomography (CBCT) 3D imaging, allow the dentist to visualize the internal structures of the tooth and the surrounding bone. Radiographs reveal the depth of the carious lesion in relation to the pulp chamber. If the X-ray shows a clear band of healthy dentin between the cavity and the nerve, a filling is appropriate. If the decay has breached the pulp, or if there is a radiolucent shadow (dark spot) at the root apex indicating bone destruction from an abscess, a root canal is definitively required.
The Risks of Delayed Treatment and Infection Spread
Postponing treatment for dental decay allows bacteria to proliferate deeper into the tooth structure, transforming a minor cavity that requires a simple filling into a severe infection demanding a root canal or extraction.
One of the most critical aspects of dental care is timely intervention. Dental caries is a progressive, irreversible disease; it does not heal on its own. A common clinical scenario involves a patient who notices mild sensitivity or a small hole in their tooth but delays seeking treatment due to anxiety, financial concerns, or a busy schedule. During this delay, the cariogenic bacteria continue to metabolize sugars and produce acids, driving the decay deeper into the dentin.
What begins as a minor issue requiring a quick, minimally invasive filling can rapidly escalate into a major medical problem. Once the bacteria breach the pulp chamber, the resulting infection can cause excruciating pain. If the patient continues to delay treatment, the nerve will eventually die. Paradoxically, the severe pain may suddenly stop when the nerve dies, leading the patient to falsely believe the problem has resolved itself. However, the necrotic tissue inside the tooth becomes a breeding ground for obligate anaerobic bacteria. These bacteria multiply and exit through the root apex, invading the surrounding alveolar bone [5].
Clinical Warning: The Dangers of Untreated Dental Infections
Ignoring the signs of deep tooth decay can lead to severe, life-altering complications. An untreated pulpal infection will inevitably progress into a periapical abscess—a localized collection of pus within the jawbone. If left unmanaged, this infection can spread through the fascial spaces of the head and neck, leading to facial cellulitis, severe swelling, and in extreme cases, airway obstruction or systemic sepsis. If you are experiencing severe, throbbing tooth pain or facial swelling, you must seek urgent relief for root canal pain and professional endodontic evaluation immediately.
Treating a tooth at the filling stage is highly predictable, cost-effective, and preserves the maximum amount of natural tooth structure. Waiting until a root canal is necessary significantly increases the complexity, time, and financial investment required to save the tooth. Furthermore, if the structural damage from the decay is too extensive, even a root canal may not be possible, and the tooth will have to be extracted and replaced with a dental implant or bridge.
Post-Operative Restoration: Crowns vs. Direct Fillings
Following a filling, the tooth is immediately functional, whereas a tooth that has undergone a root canal typically requires a full-coverage dental crown to prevent structural fracture and ensure long-term survival.
The final phase of comparing a root canal vs filling involves understanding the post-operative restorative requirements. When a tooth receives a standard composite filling, the restorative material is bonded directly into the prepared cavity. Because the tooth’s internal blood supply and moisture content remain intact, the surrounding enamel and dentin retain their natural resilience and elasticity. Once the filling is polished and the bite is adjusted, the treatment is complete, and the tooth can immediately withstand normal masticatory (chewing) forces.
Conversely, a tooth that has undergone root canal therapy undergoes significant biomechanical changes. The removal of the vital pulp means the tooth loses its internal hydration, causing the remaining dentin to become more brittle over time. Furthermore, the process of accessing the pulp chamber and cleaning the root canals requires the removal of a substantial amount of internal core structure, including the roof of the pulp chamber, which acts as a critical structural tie-bar for the tooth.
“An endodontically treated posterior tooth is highly susceptible to catastrophic vertical root fracture if not properly protected. While the root canal procedure cures the biological infection, it is the placement of a full-coverage coronal restoration, such as a ceramic crown, that ensures the long-term biomechanical survival of the tooth.”
Because of this structural compromise, a simple filling is rarely sufficient to restore a posterior tooth (molar or premolar) after a root canal. The standard of care dictates that the tooth must be protected with a full-coverage dental crown. The crown acts like a protective helmet, encasing the remaining tooth structure and distributing chewing forces evenly down the long axis of the roots, preventing the brittle tooth from splitting. Before the crown is placed, the dentist will often place a “core build-up”—a dense composite material used to replace the missing internal structure and provide a solid foundation for the crown. In some cases, a fiber or titanium post may be cemented into one of the treated root canals to help anchor the core material. Proper post-operative care, including excellent oral hygiene, is essential to prevent secondary issues such as managing post-treatment oral malodor or recurrent decay around the margins of the new crown.
When to See a Doctor for Tooth Pain
Determining whether you need a filling or a root canal is not something that can be done accurately at home; it requires professional clinical diagnostics. However, recognizing the early warning signs of dental pathology can help you seek treatment before a minor issue becomes a major emergency. You should schedule a comprehensive evaluation with a qualified dental professional, such as Dr. Nguyen Van Cuong, if you experience any of the following symptoms:
- Localized Sensitivity: Sharp, transient pain when consuming hot, cold, or sweet foods and beverages, which may indicate early enamel or dentin decay suitable for a filling.
- Lingering Pain: Pain from thermal stimuli that lasts for more than 30 seconds after the stimulus is removed, strongly suggesting irreversible nerve inflammation.
- Spontaneous Throbbing: A deep, pulsating ache that occurs without any obvious trigger, often worsening at night or when lying down.
- Pain on Biting: Sharp pain when applying chewing pressure to a specific tooth, which can indicate a cracked tooth or inflammation at the root apex.
- Gingival Swelling or Fistula: The presence of a localized swelling, a pimple-like bump (sinus tract) on the gums near the root of the tooth, or a bad taste in the mouth, all of which are classic signs of an active endodontic abscess.
Early intervention is the key to conservative dentistry. If you are experiencing any of these symptoms, we encourage you to explore our comprehensive general dental guide and contact HCMC Dental Clinic for a thorough clinical assessment to determine the most appropriate and effective treatment plan for your specific needs.

Frequently Asked Questions
How do I know if I need a root canal or just a filling?
You likely need a filling for mild sensitivity to sweet or cold foods, whereas severe, lingering throbbing pain or gum swelling typically indicates the need for a root canal. A clinical examination and dental X-rays are required to provide a definitive diagnosis. If the decay is confined to the outer enamel and dentin, a filling is sufficient. However, if the bacteria have penetrated the inner pulp chamber, endodontic therapy is mandatory to save the tooth.
Is a root canal more painful than a filling?
No, modern root canals are not more painful than fillings because both procedures are performed under profound local anesthesia. The reputation for pain comes from the severe infection preceding the treatment, not the procedure itself. Once the tooth is fully numbed, you should only feel pressure, similar to receiving a standard dental filling. Post-operative soreness is common but manageable with over-the-counter analgesics.
Can a deep filling prevent the need for a root canal?
Yes, a deep filling can sometimes prevent a root canal if the decay is removed just before it breaches the pulp chamber. Dentists often use specialized pulp-capping materials to soothe the nerve in these borderline cases. However, if the nerve is already irreversibly inflamed or infected, a deep filling will not resolve the issue, and endodontic treatment will eventually be required.
How much longer does a root canal take compared to a filling?
A standard dental filling typically takes 30 to 60 minutes in a single visit, while a root canal usually requires 90 to 120 minutes and may span one or two appointments. The extended time for endodontic therapy is due to the meticulous process of cleaning, shaping, and disinfecting the microscopic nerve canals inside the tooth roots before sealing them.
Why do I need a crown after a root canal but not after a filling?
A crown is usually required after a root canal because the tooth becomes brittle and is at a high risk of fracturing without its internal blood supply. A filling leaves the tooth’s core structure and vitality intact, so a crown is unnecessary for minor restorations. The crown provides essential structural reinforcement, ensuring the endodontically treated tooth can withstand normal chewing forces.
References
- Journal of Endodontics. Diagnostic accuracy of clinical pulp testing and radiographic imaging. (2020).
- Journal of the American Dental Association. Longevity and clinical performance of posterior composite restorations. (2021).
- International Endodontic Journal. Clinical outcomes and survival rates of primary root canal treatment. (2019).
- Clinical Oral Investigations. Histological progression of dental caries and pulpal involvement. (2018).
- British Dental Journal. Patient-reported pain and anxiety associated with endodontic procedures. (2022).