A pediatric dentist is a specialized dental professional dedicated to the oral health of children from infancy through adolescence. They complete advanced residency training to diagnose, treat, and manage pediatric dental conditions, behavioral anxieties, and developmental facial growth, ensuring a lifetime of healthy smiles.
Clinical Summary:
Pediatric dentistry (pedodontics) focuses on the comprehensive oral healthcare of infants, children, and adolescents, including those with special healthcare needs. Beyond standard dental school, these specialists undergo rigorous residency training in child psychology, growth and development, and advanced behavioral management techniques. Their clinical scope ranges from preventive interventions like sealants and fluoride varnishes to complex restorative procedures and interceptive orthodontics. By establishing a “dental home” early, pediatric dentists mitigate the risks of early childhood caries and guide optimal craniofacial development, ensuring that primary dentition successfully paves the way for a healthy permanent smile.
Key Takeaways:
- Pediatric dentists complete two to three years of specialized residency after general dental school.
- They manage everything from infant oral exams to adolescent orthodontic assessments.
- Behavioral management and child psychology are core components of their clinical practice.
- The first dental visit is highly recommended by age one or when the first tooth erupts.
- Early intervention prevents severe early childhood caries and guides proper jaw development.
The Clinical Definition: What Is a Pediatric Dentist?
A pediatric dentist is a recognized dental specialist who provides comprehensive preventive and therapeutic oral healthcare for infants, children, and adolescents. They serve as the primary care provider for pediatric dental needs, managing both routine and complex developmental conditions.
Understanding the specialized field of pediatric dentistry requires looking beyond routine teeth cleaning. A pediatric dentist, historically referred to as a pedodontist, is the pediatric equivalent of a pediatrician in medicine. While a general dentist is equipped to treat patients of all ages, a pediatric dentist limits their practice entirely to the younger demographic. This specialization is not merely a preference; it is a distinct clinical discipline recognized by major dental boards worldwide[1]. The anatomical, physiological, and psychological differences between a child and an adult necessitate a highly tailored approach to oral healthcare.
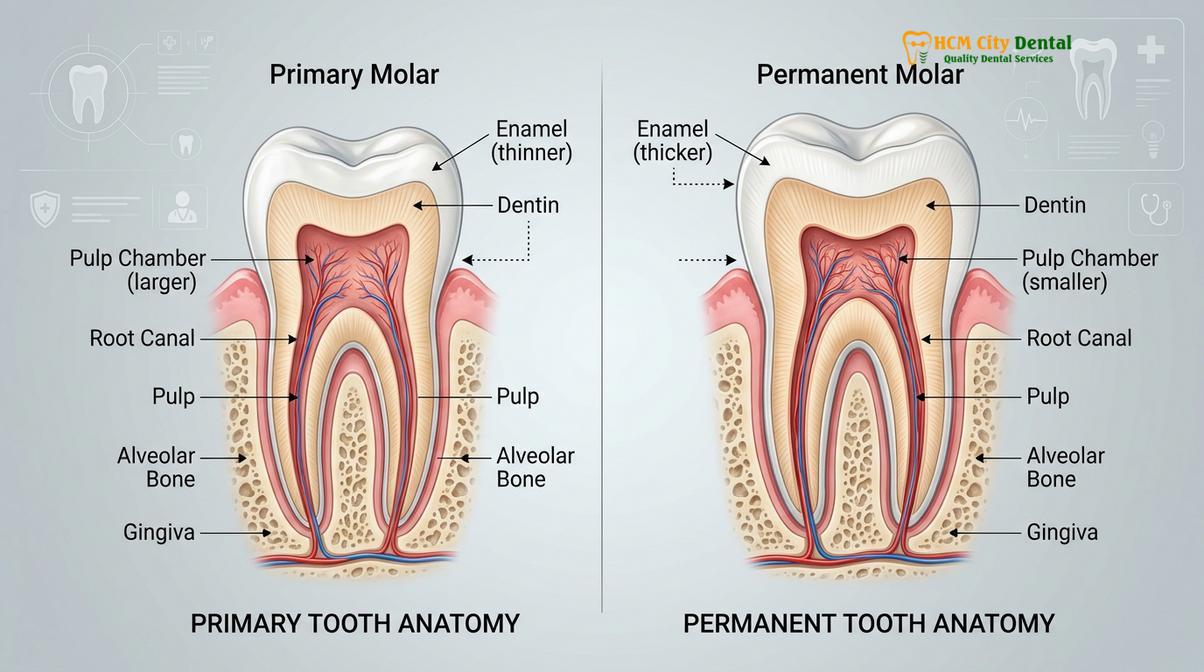
Primary teeth, commonly known as baby teeth, possess a significantly different morphology compared to permanent adult teeth. They have thinner enamel, thinner dentin, and proportionally larger pulp chambers. Because of these anatomical variations, dental caries (tooth decay) can progress rapidly from the outer enamel into the sensitive nerve tissue, leading to severe pain and systemic infection much faster than in an adult tooth. Pediatric dentists are intimately familiar with these structural nuances and utilize specialized materials and techniques designed specifically for the primary dentition.

Furthermore, the scope of a pediatric dentist extends into the realm of craniofacial growth and development. As a child grows, their maxilla (upper jaw) and mandible (lower jaw) undergo continuous changes. A pediatric specialist monitors these changes meticulously, identifying early signs of malocclusion, crowding, or skeletal discrepancies. By intervening at the optimal biological time, they can guide jaw growth and tooth eruption, often reducing or eliminating the need for extensive orthodontic work later in life. For parents seeking comprehensive general dental care for their families, understanding the unique value of a pediatric specialist is the first step toward ensuring optimal oral health for their children.
Educational Pathway: Becoming a Dentist for Children
The journey of becoming a dentist for children requires completing a standard four-year dental degree followed by a rigorous two- to three-year pediatric residency program. This advanced training focuses heavily on child psychology, sedation, and special needs care.
The process of becoming a dentist who specializes in pediatrics is exceptionally rigorous. After obtaining a Bachelor’s degree, a candidate must complete four years of dental school to earn either a Doctor of Dental Surgery (DDS) or a Doctor of Dental Medicine (DMD) degree. At this stage, the individual is a fully qualified general dentist. However, to earn the title of a pediatric dentist, they must be accepted into and complete a highly competitive pediatric dentistry residency program, which typically lasts an additional two to three years.
During this intensive residency, the curriculum shifts dramatically from general adult dentistry to the specific needs of the growing child. Residents receive extensive didactic and clinical training in child psychology and behavioral management. They learn how to communicate effectively with children at various cognitive developmental stages, from pre-verbal toddlers to independent adolescents. This psychological training is crucial, as a child’s early experiences in the dental chair often dictate their lifelong attitude toward oral healthcare[2].
Another critical component of pediatric residency is training in advanced pharmacological behavior management. Residents learn the precise protocols for administering nitrous oxide (laughing gas), oral conscious sedation, and intravenous (IV) sedation. They also complete rotations in hospital settings, where they learn to perform comprehensive dental rehabilitation under general anesthesia in operating rooms. This hospital training is particularly vital for treating young children with extensive early childhood caries or patients with severe special healthcare needs, such as autism spectrum disorder, cerebral palsy, or congenital heart defects.
“The true art of pediatric dentistry lies not just in the flawless execution of a clinical procedure, but in the ability to perform that procedure while simultaneously nurturing a child’s trust and confidence. We are treating the child’s mind just as much as we are treating their teeth.”
By the end of their residency, a pediatric dentist is not only a master of pediatric restorative techniques but also an expert in managing complex medical histories, dental trauma, and interceptive orthodontics. This specialized education ensures that they are uniquely equipped to handle any oral health challenge a child might face.
Core Clinical Procedures and Treatments
Pediatric dentists perform a wide array of procedures, including preventive fluoride applications, pit and fissure sealants, restorative fillings, and specialized pulp therapies for primary teeth. They also monitor early orthodontic needs to guide proper jaw growth.
The clinical workflow in a pediatric dental office is divided into preventive, restorative, and interceptive phases. Preventive dentistry is the cornerstone of the specialty. Pediatric dentists employ a proactive approach to stop dental disease before it starts. One of the most common preventive measures is the application of fluoride varnish. Fluoride is a naturally occurring mineral that integrates into the crystalline structure of the tooth enamel, converting hydroxyapatite into fluorapatite, which is significantly more resistant to acid attacks from cariogenic bacteria.
Another highly effective preventive treatment is the placement of dental sealants. The chewing surfaces of primary and permanent molars often feature deep pits and fissures—narrow grooves that are impossible to clean effectively with a toothbrush bristle. A pediatric dentist applies a flowable resin material into these grooves, curing it with a specialized light to create a smooth, protective barrier that seals out food particles and bacteria.
When prevention is not enough and decay occurs, restorative dentistry becomes necessary. The clinical management of tooth decay in children requires specific materials. For small to moderate cavities, pediatric dentists typically use composite resin (tooth-colored) fillings. However, if a primary tooth has extensive decay that compromises its structural integrity, a filling may not suffice. In these cases, a pediatric dentist will often place a pre-formed crown. Stainless steel crowns are the gold standard for restoring severely decayed primary molars due to their durability and moisture tolerance during placement. For anterior (front) teeth or for parents seeking a more aesthetic option, zirconia (white ceramic) pediatric crowns are increasingly utilized[3].
If the decay has reached the nerve of the primary tooth, a pediatric dentist will perform pulp therapy, commonly known as a “baby root canal.” Depending on the extent of the infection, this may involve a pulpotomy (removal of the infected coronal pulp tissue while leaving the healthy radicular pulp intact) or a pulpectomy (complete removal of the pulp tissue from the crown and roots). These procedures are critical for alleviating pain and preserving the primary tooth until it naturally exfoliates.
Summary of Pediatric Dental Interventions
| Treatment Category | Common Procedures | Clinical Objective |
|---|---|---|
| Preventive Care | Prophylaxis, Fluoride Varnish, Dental Sealants | Strengthen enamel, seal vulnerable fissures, and prevent the onset of caries. |
| Restorative Care | Composite Fillings, Stainless Steel Crowns, Zirconia Crowns | Restore the structural integrity and function of decayed or fractured teeth. |
| Pulp Therapy | Pulpotomy, Pulpectomy, Indirect Pulp Capping | Remove infected nerve tissue, alleviate pain, and save the primary tooth. |
| Interceptive Orthodontics | Space Maintainers, Palatal Expanders, Habit Appliances | Guide jaw growth, preserve space for permanent teeth, and correct crossbites early. |
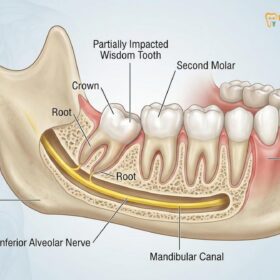
Beyond restorative work, pediatric dentists are trained to identify and manage the early stages of malocclusion. If a primary tooth is lost prematurely due to decay or trauma, the adjacent teeth can drift into the empty space, blocking the eruption path of the underlying permanent tooth. To prevent this, a pediatric dentist will place a space maintainer—a custom-made appliance that holds the space open until the adult tooth is ready to emerge. They also monitor the wisdom teeth development in older adolescents, coordinating with oral surgeons when extractions are clinically indicated.
The Infant Dentist: Early Intervention and First Visits
An infant dentist focuses on early oral health assessments, typically seeing children by their first birthday to evaluate caries risk and educate parents. This proactive approach establishes a vital dental home before complex problems develop.
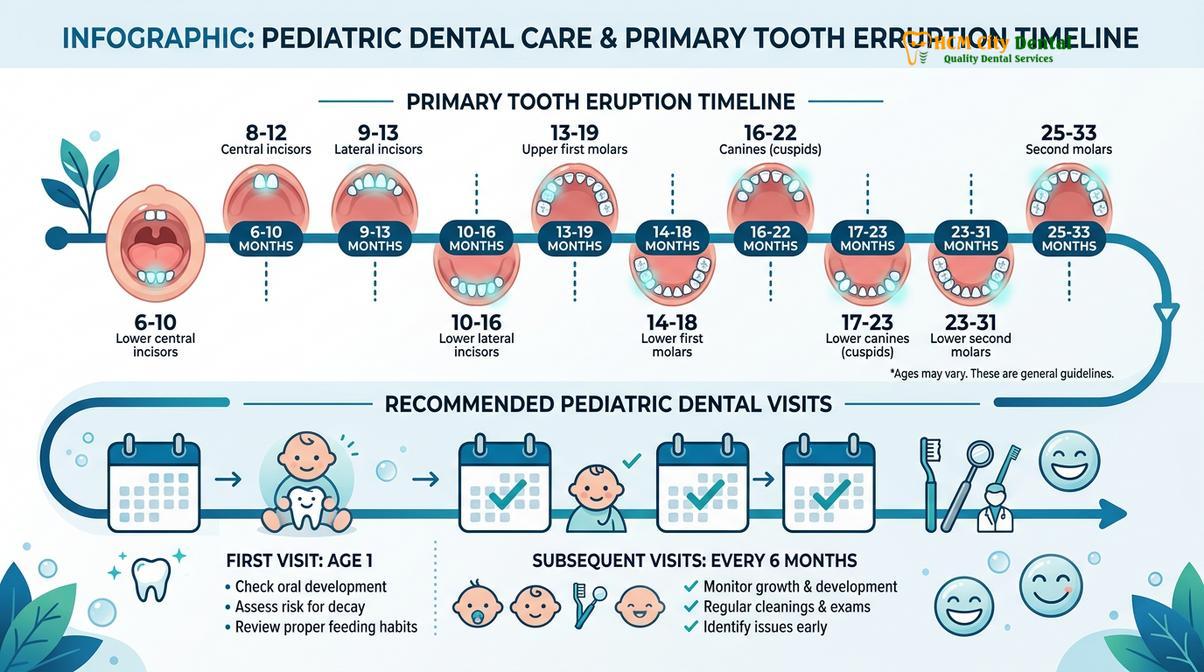
The concept of the infant dentist has gained significant traction in modern pediatric healthcare. The American Academy of Pediatric Dentistry (AAPD) and the American Academy of Pediatrics (AAP) both strongly recommend that a child’s first dental visit occur within six months of the eruption of their first tooth, and no later than their first birthday. This early intervention is not primarily about cleaning teeth; it is about establishing a “dental home” and providing crucial anticipatory guidance to parents.
During an infant oral exam, the pediatric dentist typically utilizes a “knee-to-knee” position. The parent and the dentist sit facing each other, and the child lies back with their head resting in the dentist’s lap. This position allows the dentist to perform a thorough examination while the child remains comforted by the physical contact and visual presence of their parent. The dentist evaluates the child’s oral hygiene, assesses the development of the jaws and soft tissues, and checks for early signs of demineralization or decay.
One of the primary goals of these early visits is to prevent Early Childhood Caries (ECC), previously known as “baby bottle tooth decay.” ECC is a virulent form of tooth decay that can rapidly destroy a toddler’s teeth, often leading to severe pediatric tooth pain and the need for extensive surgical intervention. Pediatric dentists educate parents on proper dietary habits, emphasizing the dangers of putting a child to bed with a bottle containing milk, formula, or juice. The pooling of these sugary liquids around the teeth during sleep, combined with decreased salivary flow, creates a highly cariogenic environment[4].
Furthermore, the infant dentist discusses teething management, non-nutritive sucking habits (such as pacifier use or thumb sucking), and proper oral hygiene techniques for infants and toddlers. By addressing these factors early, the pediatric dentist empowers parents to take control of their child’s oral health, significantly reducing the risk of future dental disease.
Behavioral Management and Dental Anxiety
Managing pediatric dental anxiety involves specialized behavioral techniques like Tell-Show-Do, positive reinforcement, and, when necessary, safe pharmacological sedation. These strategies ensure children receive essential care without developing long-term dental phobias.
Perhaps the most distinguishing characteristic of a pediatric dentist is their expertise in behavioral management. Dental anxiety is a common and entirely normal response for children facing an unfamiliar environment filled with strange sounds, bright lights, and unusual sensations. A pediatric dentist’s clinic is specifically designed to mitigate this anxiety. The waiting rooms are often vibrant and engaging, and the clinical areas are structured to feel less intimidating than a standard medical facility.
Dr. Nguyen Van Cuong, a leading expert in dental care, frequently emphasizes that the psychological approach is just as critical as the clinical technique when treating children. The foundational technique used by pediatric dentists is “Tell-Show-Do.” Before initiating any procedure, the dentist will tell the child what is going to happen using age-appropriate, non-threatening language (e.g., calling the suction a “thirsty straw” or the drill a “tooth tickler”). Next, they will show the child the instrument and demonstrate how it works, often on the child’s finger or a stuffed animal. Finally, once the child understands and is comfortable, the dentist will do the procedure.

Positive reinforcement is another critical tool. Pediatric dentists constantly praise children for specific cooperative behaviors, such as keeping their hands on their tummy or opening their mouth wide. Distraction techniques, such as playing the child’s favorite movie on a ceiling-mounted monitor or engaging them in conversation about their favorite toys, help divert their attention away from the clinical procedure.
However, despite the best non-pharmacological efforts, some children—due to young age, severe anxiety, or extensive treatment needs—cannot safely cooperate for dental procedures. In these instances, pediatric dentists are highly trained to utilize pharmacological behavior management. Nitrous oxide/oxygen analgesia is the most common and safest form of mild sedation used in pediatric dentistry. It helps relax the child, raises their pain threshold, and suppresses the gag reflex, all while the child remains fully conscious and responsive[5].
For more complex cases, oral conscious sedation or deep sedation/general anesthesia may be recommended. These modalities are administered under strict monitoring protocols, often in collaboration with a specialized pediatric anesthesiologist. The goal is always to provide the necessary dental care in the safest, most comfortable manner possible, preventing the development of lifelong dental phobias.
Tips for Choosing a Dentist for Your Child
Selecting the right provider involves evaluating their specialized credentials, the clinic’s child-friendly environment, and the practitioner’s ability to communicate effectively with young patients. A positive clinic atmosphere significantly reduces pediatric dental anxiety.
For parents, finding the right healthcare provider for their child is a top priority. When considering tips for choosing a dentist, the first and most crucial step is verifying the practitioner’s credentials. Ensure that the dentist has completed an accredited pediatric dentistry residency program. While many general dentists enjoy treating children and do an excellent job, a certified pediatric dentist has the advanced training necessary to handle complex behavioral and developmental issues.
Many parents seek a “Dr. Bright dentist” persona—a practitioner who brings radiant positivity, warmth, and engaging educational methods to the clinic. The ideal pediatric dentist should possess a calm, patient demeanor and a genuine affinity for children. During the initial consultation, observe how the dentist and their staff interact with your child. Do they speak directly to the child, or do they only address the parent? A great pediatric dentist will make the child feel seen, respected, and involved in their own care.
Clinical Case Review: Overcoming Severe Dental Phobia
A 4-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City with severe early childhood caries and extreme dental phobia, having refused to sit in the chair at a previous general dental office. The pediatric specialist utilized a desensitization approach over two introductory visits, employing the Tell-Show-Do technique and sensory-adapted environments. Once trust was established, the necessary restorative work, including stainless steel crowns and composite fillings, was successfully completed under mild nitrous oxide sedation. The patient now looks forward to their biannual checkups, demonstrating the profound impact of specialized pediatric behavioral management.
The physical environment of the clinic is also a significant factor. A pediatric dental office should be designed with children in mind. Look for a clinic that offers a welcoming atmosphere, child-sized dental chairs, and engaging visual distractions. Furthermore, inquire about the clinic’s approach to preventive care and their protocols for handling dental emergencies. A comprehensive pediatric practice will not only focus on treating existing problems but will also emphasize advanced orthodontic principles and long-term oral health strategies.
When to See a Doctor (Pediatric Dentist)
While routine biannual checkups are the standard recommendation for maintaining pediatric oral health, certain clinical situations require immediate evaluation by a pediatric dentist. Parents must be vigilant in monitoring their child’s oral cavity for signs of acute infection, developmental anomalies, or trauma.
You should schedule an immediate appointment if your child experiences any of the following:
- Visible signs of decay: White, chalky spots on the enamel (early demineralization) or dark brown/black pitting on the tooth surface.
- Acute dental pain: Spontaneous throbbing pain, especially if it wakes the child up at night, which is a strong indicator of irreversible pulpitis.
- Swelling or abscess: Any swelling of the gums, face, or neck, or the presence of a pimple-like bump (fistula) on the gums near a tooth root. This indicates a severe bacterial infection that requires urgent antibiotic therapy and clinical intervention.
- Delayed tooth eruption: If a child’s primary teeth have not begun to erupt by 15-18 months of age, or if there is a significant asymmetry in the eruption of permanent teeth.
Clinical Warning: Pediatric Dental Trauma
Dental trauma in children is a medical emergency. If a primary (baby) tooth is knocked out (avulsed), DO NOT attempt to reimplant it, as this can damage the developing permanent tooth underneath; seek immediate evaluation. If a permanent (adult) tooth is knocked out, hold it by the crown (avoid touching the root), rinse it gently with milk or saline if dirty, and attempt to reimplant it immediately, or store it in milk and rush to a pediatric dentist within 30-60 minutes for the highest chance of saving the tooth.
Dr. Cuong advises parents that early intervention is always preferable to delayed treatment. Waiting for a child to complain of pain often means that the dental disease has progressed to an advanced stage, requiring more invasive and costly procedures. Regular monitoring by a qualified pediatric specialist ensures that minor issues are addressed before they escalate into major clinical complications. If your child requires specialized restorative care, the team at HCMC Dental Clinic is equipped to provide comprehensive solutions, from preventive sealants to restorative dental prosthetics tailored for developing smiles.
Frequently Asked Questions
At what age should a child first visit a pediatric dentist?
A child should visit a pediatric dentist by their first birthday or within six months of their first tooth erupting. Early visits establish a dental home, allow for caries risk assessment, and provide parents with essential anticipatory guidance for oral hygiene. During this initial visit, the dentist will evaluate the child’s oral development, discuss teething strategies, and educate parents on proper dietary habits to prevent early childhood caries.
What is the difference between a pediatric dentist and a general dentist?
A pediatric dentist completes two to three years of specialized residency training after dental school, focusing exclusively on children. They possess advanced expertise in child psychology, craniofacial growth, sedation protocols, and managing patients with special healthcare needs. While general dentists are qualified to treat patients of all ages, pediatric specialists are uniquely equipped to handle complex behavioral issues and severe pediatric dental conditions in a child-friendly environment.
Why is it important to treat cavities in baby teeth if they fall out anyway?
Treating cavities in baby teeth is crucial because these teeth maintain space for permanent teeth, aid in speech development, and facilitate proper chewing. Untreated decay can lead to severe pain, systemic infection, and damage to the underlying developing adult teeth. Premature loss of primary teeth due to decay can cause adjacent teeth to shift, leading to severe crowding and the need for extensive orthodontic treatment later in life.
How do pediatric dentists handle children with severe dental anxiety?
Pediatric dentists utilize behavioral management techniques like Tell-Show-Do, positive reinforcement, and distraction to handle anxiety. For severe cases, they may employ safe pharmacological interventions such as nitrous oxide (laughing gas) or mild oral conscious sedation. The clinic environment is also specifically designed to be welcoming and non-threatening, helping to desensitize the child and build long-term trust between the patient and the dental team.
Are dental X-rays safe for young children?
Yes, dental X-rays are highly safe for children when proper protocols are followed. Modern digital radiography emits extremely low doses of radiation, and pediatric dentists use lead aprons and thyroid collars to ensure maximum protection during diagnostic imaging. X-rays are an essential diagnostic tool that allows the dentist to detect cavities between the teeth, evaluate the development of permanent teeth under the gums, and identify potential bone pathology.

References
- American Academy of Pediatric Dentistry (AAPD). Core Clinical Guidelines on Pediatric Oral Health. (2022).
- Journal of Dentistry for Children. Behavioral Management Techniques in Pediatric Dentistry. (2021).
- International Journal of Paediatric Dentistry. Early Childhood Caries: Etiology, Pathology, and Prevention. (2020).
- Pediatric Dentistry Journal. The Efficacy of Stainless Steel Crowns vs. Zirconia in Primary Dentition. (2019).
- Journal of Clinical Pediatric Dentistry. Sedation Protocols and Safety in Pediatric Dental Clinics. (2023).