

A dentist removes plaque and hardened tartar (calculus) using a clinical procedure called scaling. This involves specialized ultrasonic instruments that emit high-frequency vibrations to shatter calcified deposits, followed by precise manual hand scalers to meticulously scrape away remaining bacterial biofilm from the tooth surface and below the gumline[1].
Clinical Summary:
Professional plaque and calculus removal is a fundamental periodontal procedure designed to arrest gingival inflammation and prevent structural tooth loss. Dentists utilize a combination of ultrasonic cavitation and manual instrumentation to debride the clinical crown and root surfaces. While daily oral hygiene disrupts soft bacterial biofilm, mineralized calculus requires professional intervention. Advanced modalities, including air polishing and laser-assisted therapy, further enhance the efficacy of subgingival debridement. Regular diagnostic assessments ensure timely intervention, maintaining the integrity of the periodontium and supporting long-term systemic health.
Key Takeaways:
- Plaque is a soft bacterial biofilm that mineralizes into hardened calculus (tartar) within 24 to 72 hours if not mechanically removed.
- Dentists use ultrasonic scalers that rely on high-frequency vibrations and water cavitation to shatter heavy calculus deposits safely.
- Manual hand instruments, such as area-specific curettes and sickle scalers, are utilized for precise subgingival debridement and root planing.
- Scaling and root planing (SRP) is a deeper therapeutic procedure required when calculus extends beneath the gumline, causing periodontitis.
- Attempting to remove hardened calculus at home with DIY tools can cause severe enamel scratching and irreversible gingival trauma.
The Clinical Pathogenesis of Plaque and Calculus (Tartar)
Dental plaque is a sticky, complex biofilm of bacteria that, if left undisturbed, mineralizes into hardened calculus (tartar) through the precipitation of salivary calcium and phosphate ions, requiring professional extraction.
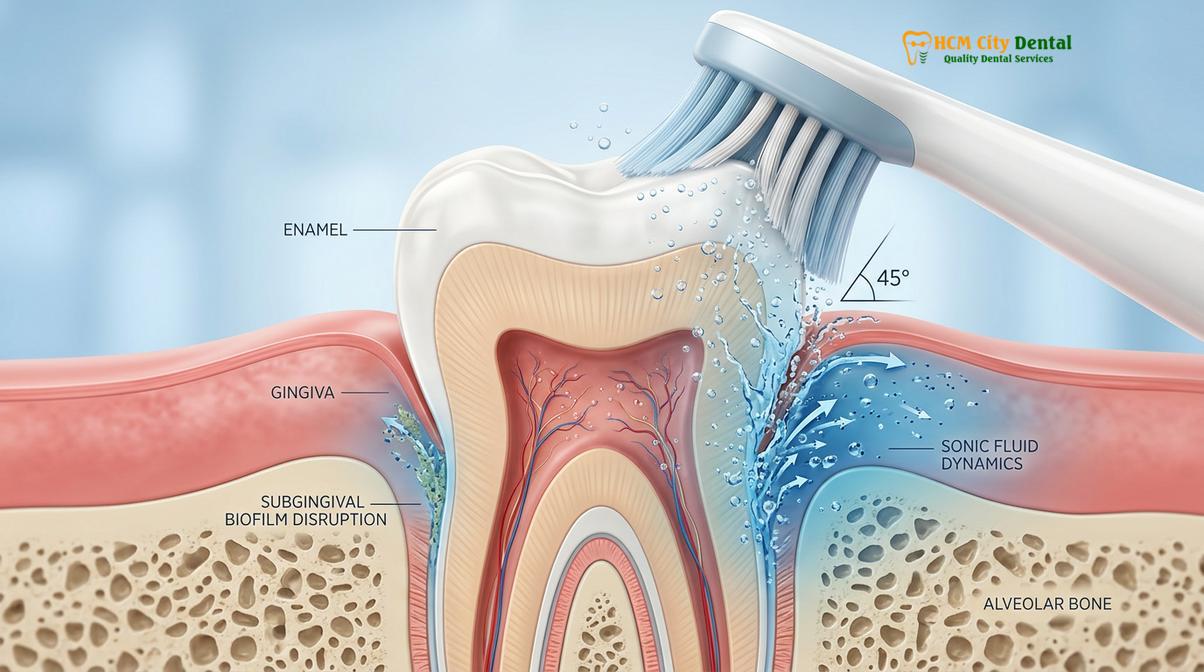
To understand how a dentist removes plaque, it is essential to first understand the biological mechanisms of how plaque forms and evolves. The oral cavity is a dynamic ecosystem. Within minutes after brushing, a thin, acellular protein layer called the acquired pellicle forms over the enamel. This pellicle, composed primarily of salivary glycoproteins, acts as an adhesive surface for primary bacterial colonizers, predominantly Gram-positive cocci.
As these initial bacteria adhere and multiply, they excrete extracellular polymeric substances (EPS), creating a sticky, protective matrix known as dental plaque. If this soft biofilm is not disrupted by daily brushing and flossing, the microenvironment within the plaque matures. Oxygen levels drop, allowing more pathogenic, Gram-negative anaerobic bacteria to thrive. This mature biofilm is highly organized and capable of triggering a localized inflammatory response in the gingival tissues[2].

When plaque remains undisturbed for 24 to 72 hours, it begins to undergo mineralization. Calcium and phosphate ions naturally present in saliva precipitate into the plaque matrix, forming crystals of hydroxyapatite. This calcification process transforms the soft, easily removable plaque into a rock-hard substance known as dental calculus, or tartar. Calculus can form above the gumline (supragingival calculus), which is typically yellow or white, or below the gumline (subgingival calculus), which often appears dark brown or black due to the incorporation of blood pigments from inflamed gums.
| Characteristic | Dental Plaque | Dental Calculus (Tartar) |
|---|---|---|
| Composition | Soft bacterial biofilm and salivary proteins | Mineralized calcium and phosphate crystals |
| Removal Method | Daily brushing and flossing at home | Professional ultrasonic and manual scaling |
| Clinical Appearance | Colorless to pale yellow, sticky film | Hardened yellow, brown, or black deposits |
| Pathological Impact | Initiates early gingival inflammation (gingivitis) | Acts as a porous reservoir for deeper periodontal infection |
Diagnostic Assessment Before Plaque Removal
Before initiating plaque removal, dentists conduct a comprehensive periodontal evaluation, utilizing calibrated periodontal probes and radiographic imaging to assess the extent of subgingival calculus and underlying alveolar bone health.
Professional plaque removal is not a one-size-fits-all procedure. It requires a meticulous diagnostic phase to determine the appropriate level of intervention. When a patient visits a clinic, the dental team begins with a thorough visual and tactile examination of the oral cavity. The dentist evaluates the color, contour, and consistency of the gingival tissues, looking for signs of erythema (redness), edema (swelling), and bleeding, which are clinical indicators of gingivitis or periodontitis.
The cornerstone of this diagnostic assessment is periodontal probing. Using a calibrated instrument called a periodontal probe, the dentist gently measures the depth of the sulcus—the space between the tooth and the surrounding gum tissue. In a healthy mouth, these probing depths typically range from 1 to 3 millimeters. Depths of 4 millimeters or greater indicate the presence of periodontal pockets, where the gingival tissue has detached from the tooth due to bacterial toxins and the body’s inflammatory response.
“Accurate periodontal probing and radiographic analysis are the cornerstones of effective calculus removal. We cannot treat what we cannot see, and subgingival diagnostics dictate the entire clinical workflow, ensuring we target the root cause of the inflammation.”
In addition to probing, radiographic imaging (X-rays) is frequently utilized. Bitewing and periapical radiographs allow the dentist to visualize the interproximal areas (between the teeth) and assess the crestal bone levels. Heavy calculus deposits often appear as radiopaque (white) spurs on the X-rays, guiding the clinician on where to focus their scaling efforts.
Professional Dental Cleaning: Step-by-Step Plaque Removal
The professional plaque removal workflow, clinically known as dental prophylaxis, systematically utilizes ultrasonic scaling, precise hand instrumentation, and coronal polishing to eradicate bacterial biofilm and restore enamel smoothness.
The clinical procedure to safely remove plaque from teeth and eliminate hardened calculus is known as scaling. This process is highly technique-sensitive and relies on a combination of advanced technology and manual dexterity. The standard workflow for a healthy patient or one with mild gingivitis involves several distinct phases.
Phase 1: Ultrasonic Scaling and Cavitation
The primary weapon against heavy calculus is the ultrasonic scaler. These devices use either magnetostrictive or piezoelectric technology to generate high-frequency vibrations at the instrument tip, typically ranging from 25,000 to 50,000 cycles per second (Hz). When the vibrating tip is applied to the tooth surface, it shatters the crystalline structure of the calculus, effectively breaking it away from the enamel.
Simultaneously, the ultrasonic scaler emits a continuous stream of water. The rapid vibration of the tip within this water creates a phenomenon known as cavitation—the formation and implosion of microscopic bubbles. The energy released by these imploding bubbles creates acoustic microstreaming, which generates fluid shear forces strong enough to lyse (break open) bacterial cell walls and flush the debris out of the gingival sulcus[3]. This dual action of mechanical vibration and fluid dynamics makes ultrasonic scaling highly efficient.
Phase 2: Manual Hand Scaling and Root Planing
While ultrasonic scalers are excellent for bulk calculus removal, they are followed by precise manual instrumentation. Dentists and dental hygienists use specialized hand tools, primarily sickle scalers and Gracey curettes. Sickle scalers have a pointed tip and two cutting edges, making them ideal for removing supragingival calculus, particularly in the tight interproximal spaces.
Gracey curettes, on the other hand, are area-specific instruments designed for subgingival use. They feature a rounded toe and a blade offset at a specific angle, allowing the clinician to adapt the cutting edge perfectly to the complex contours of the tooth roots without traumatizing the soft tissue. The clinician relies on tactile sensitivity to detect and remove microscopic remnants of calculus, ensuring the root surface is completely smooth.
Phase 3: Coronal Polishing
Once all calculus and plaque biofilm have been removed, the teeth are polished. Coronal polishing utilizes a slow-speed handpiece equipped with a soft rubber cup and a specialized prophylaxis paste. This paste contains mild abrasives, such as pumice or perlite, which gently buff the enamel surface. Polishing removes residual extrinsic stains caused by coffee, tea, or tobacco, and eliminates the microscopic acquired pellicle, leaving the teeth exceptionally smooth. A smooth enamel surface makes it significantly more difficult for new bacteria to adhere.
Deep Cleaning (Scaling and Root Planing) for Heavy Tartar
When calculus extends deep beneath the gumline causing periodontal inflammation and pocket formation, dentists perform scaling and root planing (SRP) under local anesthesia to detoxify root surfaces and promote gingival reattachment.
A standard dental prophylaxis is a preventive measure designed for patients with generally healthy gums. However, when a patient presents with active periodontal disease—characterized by deep periodontal pockets, significant subgingival calculus, and alveolar bone loss—a more intensive therapeutic procedure is required. This procedure is known as scaling and root planing (SRP), commonly referred to as a “deep cleaning.”
Because SRP involves instrumenting deep below the gumline into inflamed tissue, the dentist will typically administer local anesthesia to ensure the patient is completely comfortable. The scaling phase focuses on removing the calcified deposits from the crown and root surfaces. The root planing phase is what distinguishes this procedure from a standard cleaning. The clinician meticulously smooths the cementum (the calcified tissue covering the tooth root), removing microscopic layers of cementum that have become embedded with bacterial endotoxins.

By creating a biologically acceptable, glass-like root surface, SRP eliminates the bacterial reservoir and provides an optimal environment for the gingival tissues to heal. Following a successful SRP procedure, the inflammation subsides, the swelling resolves, and the gingival tissues can reattach to the clean root surface, effectively reducing the depth of the periodontal pockets.
Clinical Case Study: Periodontal Rehabilitation
A 45-year-old male patient presented to HCMC Dental Clinic in Ho Chi Minh City complaining of chronic halitosis and bleeding gums during brushing. Clinical examination revealed generalized heavy subgingival calculus and probing depths of 5-6mm, indicative of moderate periodontitis. The patient underwent full-mouth scaling and root planing under local anesthesia over two visits. At the 4-week re-evaluation, the gingival inflammation had completely resolved, bleeding on probing was eliminated, and pocket depths had reduced to a healthy 2-3mm, demonstrating the profound efficacy of professional subgingival debridement.
Advanced Technologies in Plaque and Calculus Removal
Modern dentistry employs advanced modalities such as air polishing with low-abrasion powders and laser-assisted periodontal therapy to disrupt plaque biofilm more efficiently, comfortably, and with superior bactericidal outcomes.
The field of periodontics is continuously evolving, and modern clinics integrate advanced technologies to enhance the efficacy and comfort of plaque removal. One such advancement is subgingival air polishing. Traditional air polishing used sodium bicarbonate powder, which was highly effective for stain removal but too abrasive for exposed root surfaces. Today, clinicians utilize ultra-fine powders like erythritol or glycine. These low-abrasion powders, combined with specialized subgingival nozzles, can safely and painlessly blast away soft plaque biofilm from deep periodontal pockets without damaging the cementum or gingival tissue[4].
Another significant advancement is laser-assisted periodontal therapy. Diode lasers, operating at specific wavelengths, are used as an adjunct to traditional scaling and root planing. The laser energy is highly absorbed by the dark pigments of periodontal pathogens and inflamed tissue. The laser effectively vaporizes the bacteria and diseased tissue lining the periodontal pocket while simultaneously coagulating blood vessels to minimize bleeding. This bactericidal effect promotes faster healing and reduces post-operative discomfort, offering a highly sophisticated approach to managing severe plaque and calculus buildup.
When to See a Dentist: Important Clinical Notes
Recognizing the early warning signs of calculus accumulation, such as gingival bleeding and persistent halitosis, is critical for seeking timely professional intervention before irreversible bone loss occurs.
Clinical Warning: Never attempt to remove hardened calculus at home using DIY tartar scrapers or sharp tools. Without professional training and visibility, these instruments can cause severe, irreversible scratches to the enamel and significant lacerations to the delicate gingival tissues, leading to acute infection and permanent recession.
Patients often wonder when it is strictly necessary to schedule a professional cleaning. While general guidelines suggest biannual visits, certain clinical signs indicate an immediate need for professional plaque removal. If you notice your gums bleeding when you brush or floss, this is a primary indicator of gingivitis caused by plaque accumulation. Additionally, persistent bad breath (halitosis) that does not improve with mouthwash, or visible yellow and brown hard deposits along the gumline, are definitive signs that calculus has formed.
According to the Vietnam Ministry of Health (MOH) National Clinical Guidelines on Odonto-Stomatology, regular periodontal assessments and professional scaling are essential preventive measures to combat the high prevalence of periodontal diseases in the population[5]. Ignoring these signs allows the bacterial biofilm to penetrate deeper into the periodontium.
“Delaying professional calculus removal allows anaerobic bacteria to proliferate beneath the gingival margin, accelerating alveolar bone loss and increasing the risk of systemic inflammatory complications.”
At-Home Maintenance vs. Professional Intervention
While daily brushing and flossing effectively disrupt soft plaque biofilm, they cannot remove mineralized calculus, making biannual professional dental cleanings essential for long-term periodontal stability.
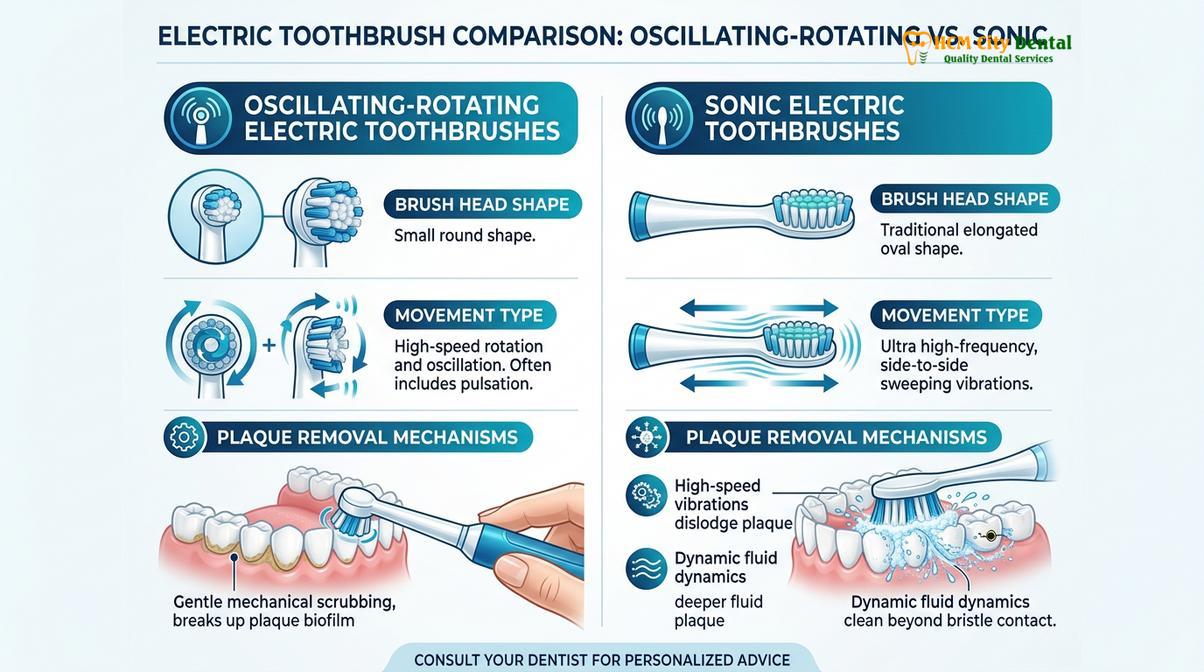
A common misconception among patients is that aggressive brushing can remove tartar. It is crucial to understand the biomechanical limitations of at-home oral hygiene. Toothbrush bristles, whether manual or electric, are designed to sweep away soft, uncalcified plaque biofilm. Dental floss is engineered to dislodge food debris and biofilm from the interproximal contact areas. However, once plaque has precipitated calcium and phosphate ions and hardened into calculus, its bond to the enamel is stronger than the physical force a toothbrush can safely apply.
Dr. Nguyen Van Cuong, a leading periodontal specialist, emphasizes that understanding how to safely remove plaque from teeth is crucial for preventing irreversible bone loss. Dr. Cuong and the clinical team utilize advanced ultrasonic instrumentation to ensure thorough debridement while maximizing patient comfort. Regular professional intervention remains the gold standard for maintaining a healthy periodontium.

Frequently Asked Questions (FAQ)
Does it hurt when a dentist removes plaque and tartar?
Professional plaque and tartar removal is generally painless, though you may experience mild sensitivity or pressure. For patients with heavy subgingival calculus or gingival inflammation, dentists can apply topical or local anesthesia to ensure a completely comfortable scaling and root planing experience.
How long does a professional plaque removal procedure take?
A standard professional dental cleaning typically takes between 30 to 60 minutes. However, if you require deep scaling and root planing due to extensive tartar buildup and periodontal disease, the procedure may be divided into multiple sessions lasting 45 to 90 minutes each.
Can I remove hardened plaque (tartar) at home?
No, you cannot safely remove hardened plaque or tartar at home. Once plaque mineralizes into calculus, it bonds tightly to the enamel and requires professional ultrasonic and manual scaling instruments. Using DIY tartar scrapers can cause severe enamel damage and irreversible gum lacerations.
How often should I get plaque professionally removed?
Most patients should undergo professional plaque removal every six months to maintain optimal oral health. Individuals with a history of periodontitis, rapid calculus accumulation, or systemic conditions like diabetes may require periodontal maintenance cleanings every three to four months based on clinical evaluation.
What is the difference between plaque and tartar?
Plaque is a soft, sticky bacterial biofilm that forms continuously on teeth and can be removed by daily brushing and flossing. Tartar, or dental calculus, is plaque that has calcified and hardened over time, requiring specialized dental instruments for safe and effective removal.
References
- Journal of Clinical Periodontology. Biofilm formation, maturation, and the pathogenesis of periodontal diseases.
- American Dental Association. Clinical practice guidelines on the non-surgical treatment of chronic periodontitis by scaling and root planing.
- International Journal of Dental Hygiene. Comparative efficacy of ultrasonic and manual scaling in the removal of subgingival calculus.
- Periodontology 2000. The role of air polishing and minimally invasive instrumentation in periodontal maintenance therapy.
- Vietnam Ministry of Health (MOH). National Clinical Guidelines on Odonto-Stomatology and Periodontal Disease Management.
If you are experiencing signs of calculus buildup or gingival inflammation, scheduling a comprehensive evaluation at HCMC Dental Clinic in Ho Chi Minh City is the first step toward restoring your periodontal health. Whether you need a routine dental cleaning or are looking for the nearest dentist to me for urgent care, our clinical team is ready to assist you.



