When selecting a dentist new to your healthcare routine, prioritizing clinical expertise, advanced diagnostic technology, and comprehensive preventive care is essential. A thorough initial evaluation establishes a baseline for long-term oral health, ensuring accurate diagnoses and personalized, evidence-based treatment protocols tailored to your unique anatomical needs.
Clinical Summary:
Transitioning to a new dental provider involves a comprehensive assessment of the clinician’s diagnostic capabilities, treatment philosophies, and technological integration. A standard initial visit should encompass full-mouth periodontal charting, digital radiographic analysis, and a meticulous oral cancer screening. Establishing a strong patient-provider relationship based on evidence-based dentistry ensures optimal continuity of care, early detection of hard and soft tissue pathologies, and the implementation of effective preventive strategies. By prioritizing a thorough clinical baseline, patients can achieve predictable, long-term oral health outcomes and mitigate the risks associated with undiagnosed dental conditions.
Key Takeaways:
- A comprehensive initial dental exam must include periodontal probing, radiographic imaging, and occlusal analysis to establish a clinical baseline.
- Modern clinics utilize advanced technologies like CBCT and intraoral scanners for precise, three-dimensional diagnostics.
- Preventive protocols should be customized based on individual caries risk, periodontal health status, and systemic health factors.
- Establishing continuity of care with a qualified practitioner minimizes the risk of undiagnosed oral pathologies and complex future interventions.
- Patient education regarding home care, biomechanics, and dietary habits is a cornerstone of effective, long-term dental treatment.
The Clinical Importance of Selecting a Qualified Practitioner
Choosing a highly qualified practitioner ensures that your oral health is managed through evidence-based protocols, minimizing diagnostic errors and optimizing long-term treatment outcomes.
The process of integrating a dentist new to your personal healthcare network requires careful consideration of their clinical methodologies, educational background, and commitment to continuing medical education. Dentistry is a rapidly evolving field where diagnostic paradigms and material sciences advance continuously. A practitioner who adheres to the latest evidence-based guidelines is better equipped to provide care that is not only effective but also minimally invasive. The initial consultation serves as a critical juncture where the clinician’s diagnostic acumen is demonstrated through a systematic evaluation of the stomatognathic system.
Continuity of care is a fundamental principle in medical and dental disciplines. When transitioning to a new provider, the transfer of historical clinical data—such as previous radiographs, periodontal charting, and records of restorative interventions—is vital. However, a meticulous clinician will always perform an independent, comprehensive assessment to verify the current physiological status of the oral cavity. This dual approach of reviewing historical data while conducting a fresh clinical evaluation prevents the propagation of previous diagnostic oversights and ensures that any newly developed pathologies are promptly identified[1].

Dr. Nguyen Van Cuong, a leading specialist at HCMC Dental Clinic, frequently emphasizes that the foundation of successful dental treatment lies in the precision of the initial diagnosis. A superficial examination that merely checks for gross carious lesions is insufficient in modern practice. Instead, a holistic approach that evaluates the interplay between the teeth, periodontium, temporomandibular joints (TMJ), and masticatory musculature is required. This comprehensive perspective allows the clinician to identify subtle biomechanical imbalances or early signs of systemic diseases that may manifest within the oral cavity.
“The initial clinical encounter is not merely an opportunity to chart existing restorations; it is a critical diagnostic window where we assess the patient’s overall risk profile, biomechanical stability, and physiological resilience, setting the trajectory for all future therapeutic interventions.”
Furthermore, the psychological aspect of transitioning to a new provider cannot be overlooked. Dental anxiety is a documented clinical phenomenon that can significantly impede a patient’s willingness to seek necessary care. A highly qualified dentist employs effective communication strategies, empathetic listening, and transparent explanations of clinical findings to build trust. By demystifying the diagnostic process and involving the patient in shared decision-making, the clinician fosters a collaborative environment that enhances treatment compliance and overall patient satisfaction.
Advanced Diagnostic Technologies in Modern Dentistry
Modern dental diagnostics rely on high-resolution imaging and digital scanning to detect micro-pathologies early, allowing for minimally invasive and highly predictable interventions.
The integration of advanced diagnostic technologies is a hallmark of a premier dental facility. When evaluating a dentist new to your care, it is imperative to assess the technological infrastructure of their practice. Traditional two-dimensional radiography, while still useful, has limitations in visualizing complex anatomical structures. Modern practices increasingly rely on digital radiography, which significantly reduces ionizing radiation exposure while providing high-contrast, manipulable images that enhance diagnostic accuracy.
For more complex diagnostic scenarios, such as endodontic retreatment, surgical implant planning, or the evaluation of impacted teeth, Cone Beam Computed Tomography (CBCT) has become the gold standard. CBCT generates a three-dimensional volumetric dataset of the maxillofacial region, allowing the clinician to visualize the exact spatial relationship between anatomical landmarks, such as the inferior alveolar nerve, the maxillary sinus, and the adjacent dentition. This level of precision is crucial for mitigating surgical risks and ensuring predictable clinical outcomes[2].
In addition to advanced imaging, intraoral digital scanners have revolutionized the way clinicians capture impressions of the dental arches. By utilizing optical scanning technology, these devices create highly accurate, full-color 3D models of the patient’s dentition in real-time. This eliminates the need for traditional elastomeric impression materials, which can be uncomfortable for patients with a strong gag reflex. The digital models are utilized for a variety of applications, including the fabrication of indirect restorations, the design of clear aligner therapy, and the longitudinal monitoring of occlusal wear or gingival recession. For a broader understanding of how these technologies fit into routine care, patients can review a comprehensive General Dentistry overview.

Another critical diagnostic tool is the intraoral camera. This device allows the clinician to capture high-definition images of specific teeth or mucosal areas, which can be displayed on a monitor for the patient to view. This visual aid is invaluable for patient education, as it allows the individual to see exactly what the dentist sees, whether it is a micro-fracture in a molar, a failing amalgam restoration, or localized gingival inflammation. By visualizing the pathology, patients are better equipped to understand the rationale behind proposed treatment plans.
Furthermore, advanced practices may utilize adjunctive diagnostic modalities such as laser fluorescence devices for the early detection of occlusal caries, or specialized light-based screening tools to identify dysplastic or malignant changes in the oral mucosa. The comprehensive utilization of these technologies ensures that the diagnostic process is objective, reproducible, and highly sensitive to early disease states, thereby facilitating proactive rather than reactive dental care.
Comprehensive Initial Examination: What to Expect
A thorough initial assessment establishes your clinical baseline, encompassing periodontal charting, hard tissue evaluation, and a meticulous screening for oral mucosal abnormalities.
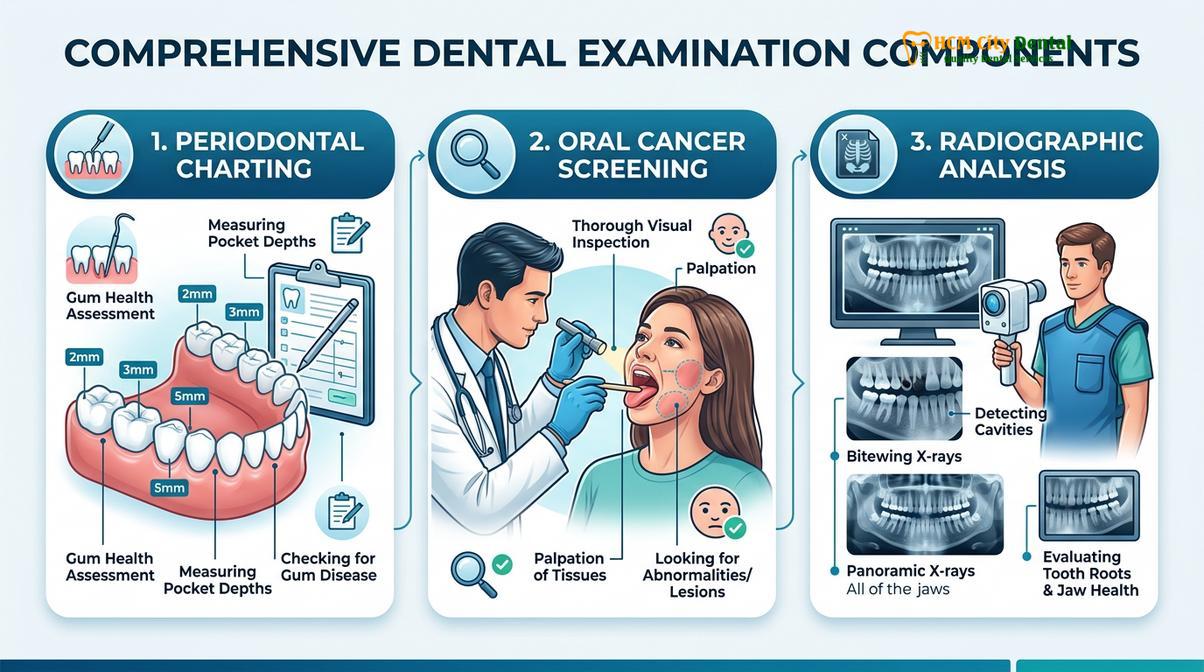
The initial comprehensive examination is the most critical appointment when establishing care with a new dental provider. This systematic evaluation goes far beyond a simple visual inspection; it is a rigorous data-gathering process designed to assess the health of all oral and maxillofacial structures. The workflow typically begins with a detailed review of the patient’s medical history, including systemic conditions, current medications, and known allergies, as many systemic diseases and pharmacological agents have direct implications for oral health and dental treatment protocols.
Following the medical history review, the clinician performs an extraoral examination. This involves the bimanual palpation of the head and neck region to assess the lymph nodes, salivary glands, and the temporomandibular joints. The dentist evaluates the TMJ for signs of crepitus, clicking, or restricted range of motion, which may indicate underlying temporomandibular disorders (TMD). The extraoral assessment also includes an evaluation of facial symmetry and the muscles of mastication for signs of hypertrophy or tenderness, often associated with bruxism.
The intraoral examination commences with a thorough oral cancer screening. The clinician systematically inspects the buccal mucosa, the hard and soft palate, the floor of the mouth, and the lateral borders of the tongue. Any mucosal abnormalities, such as leukoplakia, erythroplakia, or ulcerations that have not healed within a standard timeframe, are documented and may warrant a biopsy or referral to an oral pathologist. Early detection of oral squamous cell carcinoma significantly improves the prognosis, making this screening a non-negotiable component of the initial visit.

Subsequently, the clinician conducts a comprehensive periodontal assessment. Using a calibrated periodontal probe, the dentist or hygienist measures the depth of the gingival sulcus around each tooth at six specific sites. Healthy probing depths typically range from 1 to 3 millimeters. Depths of 4 millimeters or greater, especially when accompanied by bleeding on probing (BOP), indicate active periodontal inflammation and potential clinical attachment loss. The assessment also records gingival recession, tooth mobility, and furcation involvement. This meticulous charting is essential for diagnosing gingivitis or periodontitis and formulating an appropriate Comprehensive Oral Hygiene Steps protocol[3].
The hard tissue evaluation involves a tooth-by-tooth inspection to detect primary carious lesions, evaluate the integrity of existing restorations, and identify structural defects such as enamel infractions or attrition. The clinician correlates the clinical findings with the radiographic data to ensure no interproximal or subgingival pathologies are overlooked. Finally, an occlusal analysis is performed to assess the dynamic relationship between the maxillary and mandibular teeth during functional movements, identifying any premature contacts or occlusal interferences that could compromise the longevity of the dentition.
| Clinical Component | Standard Periodic Check-up | Comprehensive Initial Examination |
|---|---|---|
| Medical History | Brief update of changes | In-depth review of systemic health and medications |
| Radiographic Imaging | Bitewings (if due) | Full Mouth Series (FMX) or panoramic/CBCT |
| Periodontal Assessment | Basic screening (PSR) | Full-mouth 6-point probing, recession, and mobility charting |
| Oral Cancer Screening | Visual inspection | Detailed visual and bimanual palpation (intra/extraoral) |
| Occlusal Analysis | Basic bite check | Detailed evaluation of TMJ, wear facets, and functional pathways |
Evaluating Preventive and Restorative Treatment Protocols
Effective dental practices prioritize preventive strategies, such as customized prophylaxis and remineralization therapies, while utilizing biocompatible materials for necessary restorative procedures.
Once the comprehensive diagnostic data has been collected and analyzed, the clinician formulates a customized treatment plan. A hallmark of a high-quality dental practice is a strong emphasis on preventive dentistry. The goal is to intercept disease processes at their earliest stages, thereby minimizing the need for extensive restorative interventions. Preventive protocols are highly individualized, taking into account the patient’s specific caries risk assessment (CAMBRA) and periodontal phenotype.
For patients with a high susceptibility to dental caries, the preventive strategy may include the application of professional-grade topical fluorides, the placement of pit and fissure sealants on susceptible molars, and the prescription of high-concentration fluoride dentifrices for home use. The clinician will also provide targeted nutritional counseling, discussing the impact of fermentable carbohydrates and acidic beverages on the oral microbiome and enamel demineralization. Patients often inquire about dietary impacts, such as Is Milk Bad For Your Teeth, and a knowledgeable practitioner will explain the complex interactions between dietary calcium, lactose, and oral bacteria.
Periodontal maintenance is another critical component of the preventive paradigm. Based on the initial periodontal charting, the clinician will determine the appropriate frequency for professional prophylaxis. While a biannual schedule is standard for periodontally healthy individuals, patients with a history of periodontal disease may require more frequent interventions, such as quarterly scaling and root planing, to disrupt subgingival biofilms and maintain clinical attachment levels. Understanding How Often Should You Have Your Teeth Cleaned is essential for long-term tissue stability.
“The paradigm of modern dentistry has shifted from a surgical-restorative model to a medical-preventive model. Our primary objective is the preservation of natural tooth structure through proactive risk management and early, minimally invasive interventions.”
When restorative treatment is unavoidable, the selection of dental materials is of paramount importance. Modern dentistry utilizes a variety of biocompatible materials, including advanced composite resins, glass ionomers, and high-strength ceramics such as lithium disilicate and zirconia. A qualified dentist will select the appropriate material based on the specific biomechanical demands of the restoration site, the aesthetic requirements of the patient, and the principles of minimally invasive dentistry. For instance, direct composite restorations are often preferred for small to moderate lesions due to their ability to bond micromechanically to the tooth structure, thereby conserving healthy enamel and dentin[4].
In cases requiring indirect restorations, such as crowns or onlays, the integration of CAD/CAM (Computer-Aided Design and Computer-Aided Manufacturing) technology allows for the precise fabrication of highly aesthetic and durable prostheses. The clinician must ensure that the margins of these restorations are meticulously adapted to the tooth preparation to prevent microleakage and secondary caries. The overarching philosophy of restorative care should always prioritize the restoration of form, function, and aesthetics while maximizing the longevity of the natural dentition.
Orthodontic and Specialized Care Considerations
A comprehensive dental provider evaluates occlusal harmony and craniofacial development, identifying malocclusions early to prevent complex biomechanical complications and temporomandibular joint disorders.
While general dentists focus primarily on preventive and restorative care, a comprehensive practitioner also possesses a deep understanding of orthodontic principles and craniofacial growth. During the initial examination, the clinician evaluates the patient’s occlusal classification (Class I, II, or III), the degree of overjet and overbite, and the presence of any crossbites or crowding. Identifying these malocclusions is critical, as improper bite alignment can lead to uneven distribution of masticatory forces, resulting in accelerated occlusal wear, abfraction lesions, and periodontal trauma.
For pediatric patients, early interceptive orthodontics (Phase I treatment) can be highly beneficial. A vigilant dentist monitors the eruption sequence of the primary and permanent dentition, identifying potential space management issues or skeletal discrepancies early in development. Interventions such as palatal expansion or the use of space maintainers can guide the growth of the maxilla and mandible, potentially reducing the complexity of future orthodontic treatments. In rare cases, anomalies such as Natal Teeth may be identified in infants, requiring specialized pediatric management to ensure proper feeding and prevent aspiration risks.
In adult patients, the correction of malocclusion is often pursued not only for aesthetic enhancement but also for functional stability. The advent of clear aligner therapy has made orthodontic treatment more accessible and acceptable to the adult demographic. However, it is crucial that any orthodontic intervention is preceded by a thorough periodontal and restorative evaluation. Moving teeth in the presence of active periodontal inflammation can exacerbate bone loss and lead to irreversible complications. Patients must be educated on the clinical risks associated with improper orthodontic mechanics, often referred to colloquially as Bad Braces, which highlights the necessity of professional supervision during tooth movement[5].
When a patient’s clinical needs exceed the scope of general practice, a highly qualified dentist will seamlessly coordinate care with dental specialists, such as periodontists, endodontists, or oral and maxillofacial surgeons. This interdisciplinary approach ensures that complex cases, such as full-mouth rehabilitation or advanced implantology, are managed by a team of experts collaborating to achieve the optimal clinical outcome. The ability of a general dentist to act as the “quarterback” of the patient’s oral healthcare team is a defining characteristic of superior clinical practice.
When to See a Doctor: Recognizing Dental Emergencies
While establishing a routine with a new dental provider is focused on preventive and planned restorative care, patients must also be able to recognize the clinical signs of acute dental emergencies that require immediate professional intervention. Delaying treatment for severe oral pathologies can lead to systemic complications, irreversible tissue damage, and the loss of the affected dentition.
Acute odontogenic infections are a primary reason for emergency dental visits. Symptoms such as severe, throbbing pain that disrupts sleep, localized intraoral swelling, or extraoral facial asymmetry indicate a spreading infection that may have breached the cortical bone. If these symptoms are accompanied by systemic signs such as fever, lymphadenopathy, or difficulty swallowing and breathing (dysphagia and dyspnea), the patient must seek immediate emergency medical care, as the infection may be compromising the airway or spreading to fascial spaces.
Clinical Warning: Dental trauma, such as the avulsion (complete displacement) of a permanent tooth, requires immediate clinical action. The avulsed tooth should be handled only by the crown, gently rinsed without scrubbing the root surface, and ideally replanted in the socket or stored in a physiological medium (like cold milk or Hank’s Balanced Salt Solution). Seeking emergency dental care within 30 to 60 minutes significantly increases the probability of successful replantation and periodontal ligament reattachment.
Other conditions warranting prompt evaluation include severe spontaneous pain indicative of irreversible pulpitis, significant trauma resulting in complicated crown fractures that expose the dental pulp, and uncontrolled bleeding following a recent surgical extraction. A reliable dental practice will have established protocols for managing acute emergencies, ensuring that patients receive timely palliative care and definitive treatment to resolve the underlying pathology.
Case Study: Transitioning to a Comprehensive Care Model
Clinical case reviews demonstrate how transitioning to a technologically advanced practice can resolve chronic, previously undiagnosed oral health issues through meticulous diagnostic workflows.
The clinical impact of selecting a highly qualified dental provider is best illustrated through practical case outcomes. Consider the scenario of a patient who recently relocated and sought care from a dentist new to their routine. The patient presented with a history of chronic, low-grade discomfort in the posterior mandible and a generalized dissatisfaction with the aesthetic appearance of their aging composite restorations.
Clinical Case Review: Comprehensive Diagnostic Resolution
Patient Profile: A 45-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City for an initial comprehensive evaluation after experiencing intermittent masticatory pain.
Clinical Findings: Dr. Nguyen Van Cuong conducted a meticulous examination. While traditional bitewing radiographs appeared unremarkable, a CBCT scan revealed a subtle, previously undetected periapical radiolucency associated with a mesial root of the mandibular first molar, indicative of a failing endodontic treatment with a missed canal. Furthermore, occlusal analysis demonstrated severe working-side interferences contributing to the fracture of several existing restorations.
Treatment Protocol: The treatment plan involved targeted endodontic retreatment utilizing a dental operating microscope to locate and instrument the missed canal, thereby resolving the chronic infection. Subsequently, the occlusal scheme was harmonized through selective equilibration, and the failing restorations were replaced with highly durable, CAD/CAM-milled lithium disilicate onlays.
Outcome: The patient reported complete resolution of the masticatory pain. The integration of advanced diagnostics and a comprehensive biomechanical approach not only addressed the acute pathology but also established long-term occlusal stability, highlighting the profound benefits of transitioning to an evidence-based clinical practice.

This case underscores the necessity of moving beyond superficial examinations. By utilizing advanced imaging and applying a deep understanding of occlusal dynamics, the clinical team was able to diagnose the root cause of the patient’s symptoms rather than merely treating the superficial manifestations. For patients seeking to establish a new dental home, prioritizing practices that exhibit this level of diagnostic rigor and comprehensive treatment planning is essential for achieving enduring oral health.
Frequently Asked Questions
Clear answers to common patient inquiries help demystify the process of transitioning to a new dental provider and emphasize the importance of comprehensive clinical protocols.
What clinical records should I provide to a dentist new to my care?
You should provide your complete dental history, including recent radiographs, periodontal charting, and a list of current medications. Supplying these comprehensive records allows your new practitioner to establish an accurate clinical baseline, understand previous treatment modalities, and avoid unnecessary duplication of diagnostic imaging, thereby minimizing radiation exposure. It also provides context for any ongoing or chronic oral health conditions.
How does a comprehensive initial dental examination differ from a standard check-up?
A comprehensive examination involves a meticulous evaluation of all intraoral and extraoral structures, whereas a standard check-up typically focuses on routine maintenance. The comprehensive assessment includes full-mouth periodontal probing, an oral cancer screening, occlusal analysis, temporomandibular joint evaluation, and a detailed review of hard and soft tissues to formulate a long-term treatment strategy, establishing the foundation for all future care.
Why is full-mouth periodontal charting necessary during the first visit?
Periodontal charting is essential to quantitatively measure the health of the gingival tissues and alveolar bone support. By recording probing depths, clinical attachment loss, and bleeding indices, the clinician can accurately diagnose the presence and severity of periodontal disease, which is critical for determining the appropriate prophylactic or therapeutic interventions and preventing future tooth mobility or loss.
What advanced diagnostic technologies should a modern dental clinic utilize?
A modern clinical facility should utilize digital radiography, intraoral scanners, and Cone Beam Computed Tomography (CBCT) when indicated. These advanced modalities provide high-resolution, three-dimensional anatomical data, enabling the precise detection of micro-pathologies, accurate implant planning, and the formulation of minimally invasive treatment protocols that enhance overall clinical predictability and patient safety.
How often should I schedule preventive maintenance appointments with my new provider?
Preventive maintenance intervals should be customized based on your individual caries risk and periodontal health status. While a biannual schedule is common for healthy individuals, patients with a history of periodontitis, high cariogenic susceptibility, or complex restorative work may require more frequent clinical interventions, such as quarterly scaling and root planing, to maintain optimal oral health and prevent disease recurrence.
References
- Journal of the American Dental Association. Evidence-based clinical practice guideline on the comprehensive dental evaluation. (2021).
- International Journal of Dentistry. The role of Cone Beam Computed Tomography (CBCT) in modern dental diagnostics. (2020).
- Journal of Periodontology. Parameters of care and clinical protocols for periodontal charting and assessment. (2019).
- Clinical Oral Investigations. Biocompatibility and longevity of modern restorative dental materials. (2022).
- American Journal of Orthodontics and Dentofacial Orthopedics. Early detection and interceptive management of malocclusions. (2018).