Dental reconstruction before and after results showcase the profound transformation of severely compromised dentition into a fully functional, aesthetically pleasing smile. This comprehensive clinical process involves restoring all teeth in both the upper and lower jaws to correct bite alignment, resolve pain, and rebuild structural integrity.
Clinical Summary:
Full mouth dental reconstruction is a complex, multi-disciplinary approach designed to rehabilitate patients with extensive tooth loss, severe wear, or advanced periodontal disease. By combining restorative dentistry, implantology, and orthodontics, clinicians can rebuild the occlusal foundation. The “before” phase requires meticulous 3D diagnostics and treatment planning, while the “after” results yield restored masticatory function, improved facial aesthetics, and long-term oral health stability. Success depends on precise execution, high-quality biomaterials, and rigorous post-operative maintenance to ensure the longevity of the restorations.
Key Takeaways:
- Reconstruction addresses severe decay, trauma, and occlusal collapse simultaneously.
- Diagnostic phases utilize CBCT scans and digital smile design for precise planning.
- Treatments often combine dental implants, crowns, bridges, and periodontal therapy.
- Functional restoration is prioritized alongside aesthetic improvements.
- Long-term success requires strict adherence to oral hygiene and regular clinical monitoring.
Understanding Full Mouth Dental Reconstruction
Full mouth reconstruction is a comprehensive restorative protocol that rebuilds or replaces all teeth in a patient’s mouth to restore optimal oral function, neuromuscular harmony, and facial aesthetics.
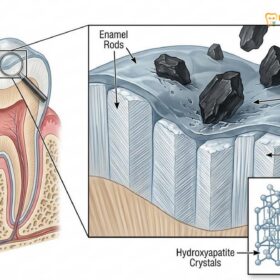
Unlike a standard smile makeover, which is primarily driven by cosmetic desires, a full mouth reconstruction is a medical necessity for patients suffering from severe dental degradation. This degradation can result from years of untreated decay, chronic acid erosion, severe bruxism (teeth grinding), or traumatic injury. The goal of this extensive treatment is not merely to create a visually appealing smile, but to re-establish the structural foundation of the mouth. This involves restoring the vertical dimension of occlusion (VDO)—the optimal distance between the upper and lower jaws when the teeth are in contact. When teeth are severely worn or missing, this dimension collapses, leading to temporomandibular joint (TMJ) disorders, facial sagging, and impaired masticatory (chewing) function[1].
The scope of full mouth reconstruction falls under advanced Comprehensive General Dental Guide: Clinical Care | HCMC Dental, requiring a highly coordinated approach. A single clinician rarely performs all aspects of the treatment independently; instead, it involves a symphony of specialists. Prosthodontists, oral surgeons, periodontists, and endodontists collaborate to ensure that every biological and mechanical requirement is met. The “before” state of a reconstruction patient is often characterized by chronic pain, difficulty eating, and profound psychological distress due to the appearance of their teeth. The “after” state represents a complete rehabilitation of the stomatognathic system, allowing the patient to function normally and smile with confidence.

The Biomechanics of Occlusal Collapse
To truly appreciate the transformation seen in dental reconstruction before and after cases, one must understand the biomechanics of occlusal collapse. The human dentition is designed to distribute the immense forces of chewing evenly across 28 to 32 teeth. When multiple teeth are lost or severely compromised, the remaining teeth are forced to bear a disproportionate amount of this load. This leads to accelerated wear, micro-fractures, and eventual mobility of the surviving teeth. Furthermore, the loss of tooth structure causes the lower jaw to over-close, placing unnatural stress on the TMJ and the associated masticatory muscles[2].
Reconstruction aims to halt this destructive cycle. By replacing missing teeth with implants or bridges and restoring worn teeth with crowns or onlays, the clinician redistributes the occlusal forces evenly. This stabilization is critical. Without it, any restorative work would be subjected to the same pathological forces that destroyed the natural dentition, leading to premature failure of the prosthetics.
Clinical Diagnostics: The ‘Before’ Phase
The initial diagnostic phase involves rigorous clinical evaluation, 3D imaging, and bite analysis to map out the exact structural deficits and biological health before any treatment begins.
The foundation of any successful full mouth reconstruction lies in the meticulousness of the diagnostic phase. Rushing into treatment without a comprehensive understanding of the patient’s unique anatomy and pathology is a recipe for clinical failure. Dr. Nguyen Van Cuong, a leading specialist in complex rehabilitations, emphasizes that the diagnostic phase is where the true success of the reconstruction is determined. He notes that meticulous planning ensures every subsequent intervention is predictable and safe. Under his guidance, patients undergoing General Dentistry tại HCMC Dental Clinic receive highly individualized care tailored to their specific anatomical needs.
The first step is a thorough clinical examination. The dentist evaluates the health of every remaining tooth, assessing for decay, structural integrity, and vitality. Periodontal health is equally critical; the gums and underlying alveolar bone must be free of active infection. Conditions such as Halitosis: Clinical Causes, Diagnostics & Treatment | HCMC Dental often serve as clinical indicators of deep periodontal pockets or hidden decay that must be addressed before any restorative work can commence. Placing a beautiful ceramic crown on a tooth with compromised periodontal support is akin to building a house on a crumbling foundation.
Advanced Imaging and Digital Smile Design
Modern dental reconstruction relies heavily on advanced imaging technologies. Cone Beam Computed Tomography (CBCT) provides a three-dimensional view of the maxillofacial structures. This is indispensable for evaluating bone volume and density, identifying hidden pathologies, and planning the precise placement of dental implants. Unlike traditional 2D X-rays, CBCT allows the surgeon to navigate the complex anatomy of the jaw, avoiding critical structures such as the inferior alveolar nerve and the maxillary sinus[3].
In addition to radiographic imaging, intraoral scanners are used to create highly accurate digital impressions of the patient’s current dentition. These digital models are then articulated in specialized software to analyze the patient’s bite. Through Digital Smile Design (DSD), clinicians can digitally simulate the proposed outcome, allowing the patient to visualize the “after” results before any physical alterations are made. This digital wax-up serves as the architectural blueprint for the entire reconstructive process.
Treatment Modalities and Collaborative Workflows
Reconstructive workflows integrate multiple dental disciplines, utilizing implants, prosthetics, and sometimes orthodontic alignment to rebuild the dental arch systematically and predictably.
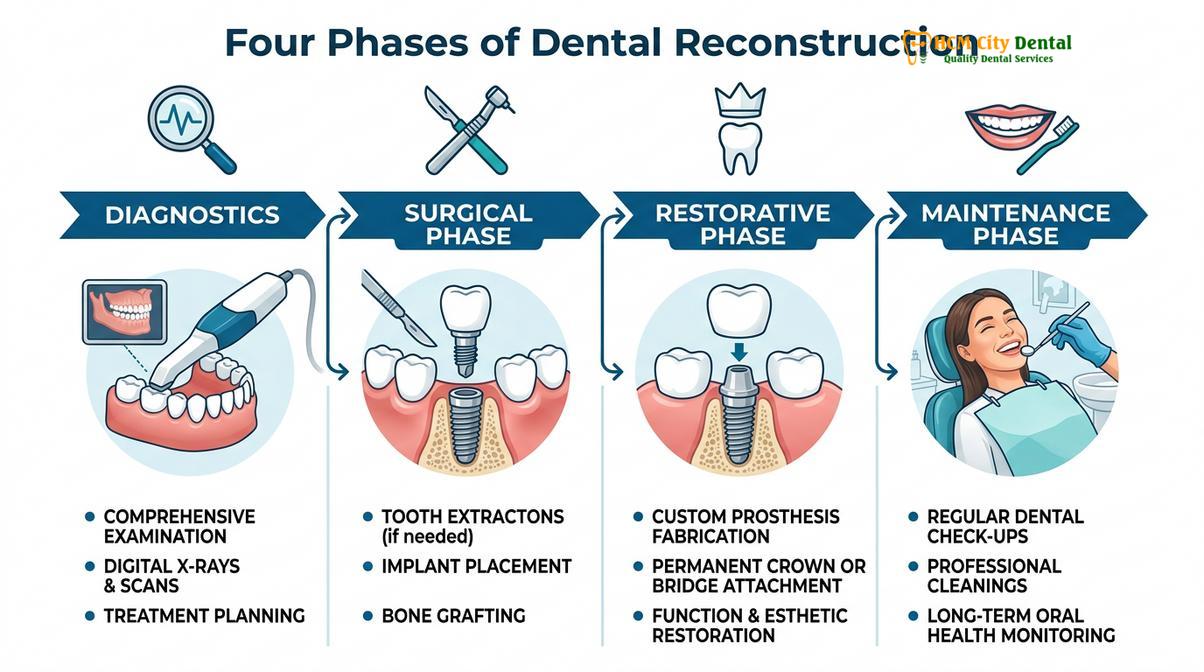
Because full mouth reconstruction addresses multiple complex issues simultaneously, the treatment plan is typically divided into distinct phases. This phased approach allows for proper healing between procedures and ensures that each step builds upon a stable foundation. The sequence of treatment is highly individualized, but it generally follows a logical progression from disease control to surgical intervention, and finally, to definitive restoration.
Phase 1: Disease Control and Preparatory Care
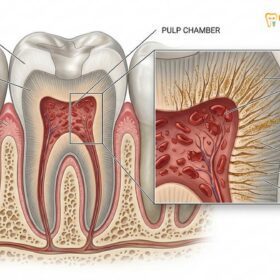
Before any permanent restorations are placed, the oral environment must be rendered healthy. This phase involves extracting teeth that are deemed unsalvageable, performing root canal therapy on teeth with pulpal infection, and executing deep periodontal cleanings (scaling and root planing) to arrest gum disease. In many cases, integrating orthodontic and prosthodontic treatment plans is necessary to move misaligned teeth into optimal positions before they are restored with crowns or veneers[5].
Phase 2: Surgical Interventions
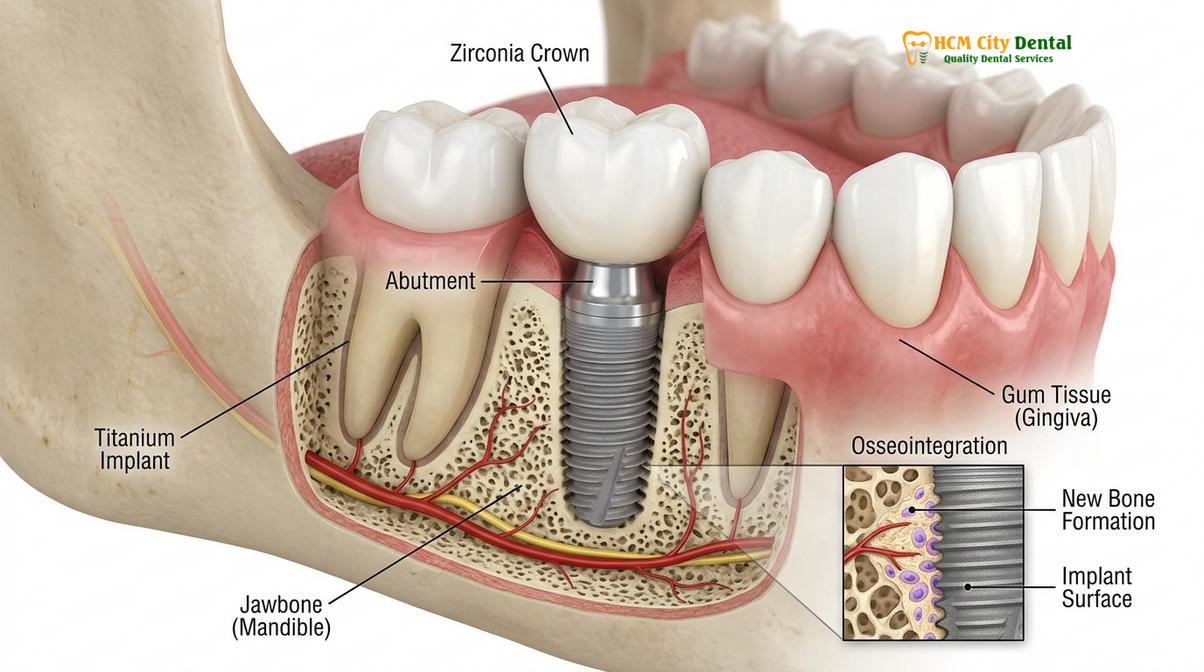
Once the mouth is free of active disease, the surgical phase begins. For patients missing multiple teeth, dental implants are the gold standard for replacement. Implants act as artificial tooth roots, surgically embedded into the jawbone. Over a period of several months, the titanium posts undergo osseointegration—a biological process where the bone fuses directly to the implant surface, providing unparalleled stability. If the patient lacks sufficient bone volume to support implants, bone grafting or sinus lift procedures may be performed concurrently or prior to implant placement[4].
Phase 3: Definitive Restorations
The final phase involves the fabrication and placement of the permanent prosthetics. Depending on the patient’s needs, this may include a combination of single crowns, multi-unit bridges, porcelain veneers, or implant-supported full-arch prostheses (such as All-on-4 or All-on-6). The choice of materials is critical. High-strength ceramics like Yttria-stabilized zirconia are often used for posterior teeth that endure heavy chewing forces, while highly aesthetic lithium disilicate (e.max) may be chosen for the anterior (front) teeth to mimic the natural translucency of enamel.
| Treatment Modality | Primary Clinical Indication | Functional Benefit | Estimated Longevity |
|---|---|---|---|
| Dental Implants | Missing individual or multiple teeth, edentulism | Prevents bone loss, restores full bite force, independent support | 20+ years to lifetime (with care) |
| Zirconia Crowns | Severely decayed, fractured, or endodontically treated teeth | Provides maximum structural protection and high fracture resistance | 10 – 15+ years |
| Porcelain Veneers | Anterior teeth with severe wear, discoloration, or minor misalignment | Restores anterior guidance and highly aesthetic facial profile | 10 – 15 years |
| Implant-Supported Bridges | Multiple consecutive missing teeth with sufficient bone | Eliminates the need for removable partial dentures, highly stable | 15+ years |

The ‘After’ Phase: Functional and Aesthetic Outcomes
Following completion, patients experience a stabilized bite, restored chewing capacity, and a natural-looking facial profile that resolves previous structural collapse and functional limitations.
The culmination of a full mouth reconstruction is a profound moment for the patient. The “after” phase is characterized by a complete reversal of the debilitating symptoms that prompted the treatment. Functionally, the restoration of the vertical dimension of occlusion allows the TMJ to rest in its natural, unstrained position, frequently alleviating chronic jaw pain, tension headaches, and muscle fatigue. The patient regains the ability to chew a diverse, nutrient-rich diet, which has cascading positive effects on their overall systemic health and gastrointestinal function.
Aesthetically, the transformation is equally dramatic. Severe tooth wear often leads to a collapsed lower third of the face, resulting in deep wrinkles around the mouth and a prematurely aged appearance. By rebuilding the teeth to their proper height and volume, the underlying facial musculature is supported once again. The lips appear fuller, the jawline is more defined, and the overall facial profile is rejuvenated. This structural support is a critical, yet often overlooked, benefit of comprehensive dental rehabilitation.
Clinical Case Review: Severe Attrition and Bite Collapse
A 55-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City with severe generalized attrition (wear) due to decades of untreated nocturnal bruxism. The patient’s vertical dimension had collapsed by nearly 4mm, causing chronic TMJ discomfort and aesthetic concerns. The reconstructive workflow involved a full-arch digital scan, followed by the placement of 24 monolithic zirconia crowns to re-establish the correct VDO. Post-treatment, the patient reported complete resolution of joint pain and demonstrated a highly aesthetic, stable occlusal relationship. A custom occlusal guard was fabricated to protect the new restorations during sleep.
“The transition from a collapsed bite to a fully reconstructed arch not only restores masticatory efficiency but also provides crucial support to the facial musculature, preventing premature aging and resolving chronic neuromuscular pain.”
The psychological impact of the “after” phase cannot be overstated. Patients who have spent years hiding their smiles or avoiding social situations due to dental embarrassment often experience a massive surge in self-confidence. The ability to speak clearly, laugh openly, and eat without pain or hesitation fundamentally improves their quality of life.
Navigating Financial Considerations and Global Care
Complex reconstructions require significant investment, prompting many patients to evaluate insurance benefits or explore high-quality international dental networks to manage out-of-pocket costs effectively.
Full mouth reconstruction is a major medical and financial undertaking. Because the treatment involves multiple specialists, advanced surgical procedures, and premium biomaterials, the total cost can be substantial. Navigating the landscape of dental insurance carriers can be frustrating for patients requiring extensive work. It is a common misconception that insurance will cover the entirety of the procedure. In reality, finding a policy that offers complete coverage for full mouth reconstruction is virtually impossible. Most plans have strict annual maximums and categorize many reconstructive procedures—particularly implants and advanced prosthetics—as elective or cosmetic, leaving the patient responsible for a significant portion of the bill.
Faced with these financial hurdles, patients often begin their journey by consulting local providers for an initial assessment. However, upon receiving the comprehensive treatment plan and cost estimate, many realize that completing the work domestically may be financially prohibitive. This realization drives a growing number of patients to explore options within a global dental clinic network.
Dental tourism has evolved significantly, with modern international clinics offering care that meets or exceeds Western standards. Facilities like HCMC Dental Clinic in Ho Chi Minh City utilize the exact same digital scanners, CBCT machines, and premium implant brands (such as Straumann or Nobel Biocare) as top-tier clinics in the US or Europe, but at a fraction of the cost. This allows patients to receive uncompromising clinical quality while managing their financial investment responsibly. When learning How to Find a Good Dentist: A Complete Clinical Guide | HCMC Dental abroad, it is imperative to verify their credentials, review their before-and-after case portfolios, and ensure they follow strict international sterilization protocols.
When to See a Doctor for Dental Reconstruction
Identifying the early warning signs of occlusal collapse and structural failure is critical to preventing irreversible damage to the jawbone and temporomandibular joints.
Recognizing the signs that you may need a full mouth reconstruction is the first step toward reclaiming your oral health. Unlike a single cavity or a minor chip, the indications for full reconstruction are systemic and progressive. If you are experiencing multiple, overlapping dental issues, it is crucial to seek a comprehensive evaluation rather than attempting to patch the problems one tooth at a time.
You should schedule a consultation with a reconstructive specialist if you experience any of the following symptoms:
- Extensive Tooth Loss: Missing multiple teeth in both the upper and lower arches, which impairs your ability to chew and causes remaining teeth to shift.
- Severe Tooth Wear: Teeth that appear unusually short, flat, or transparent at the edges, often a result of chronic bruxism or acid reflux.
- Chronic Jaw Pain: Persistent discomfort in the TMJ, frequent tension headaches, or clicking and popping sounds when opening and closing the mouth.
- Failing Dental Work: Multiple old crowns, large fillings, or bridges that are breaking down, leaking, or causing recurrent decay.
- Advanced Periodontal Disease: Loose teeth, receding gums, and chronic infections that threaten the stability of the entire dental arch.
According to the Vietnam Odonto-Stomatology Association (VOSA), timely intervention in cases of severe occlusal wear is essential to prevent the complete collapse of the vertical dimension, which can lead to severe functional impairment[6]. Delaying treatment often results in the need for more invasive and costly surgical procedures, such as extensive bone grafting, to rebuild the foundation before prosthetics can be placed.
“Comprehensive dental rehabilitation is not merely about aesthetics; it is a fundamental restoration of the stomatognathic system that directly impacts a patient’s systemic health and daily quality of life.”
Important Clinical Notes and Maintenance
The longevity of a full mouth reconstruction depends entirely on the patient’s commitment to meticulous daily oral hygiene and adherence to a strict professional maintenance schedule.
Achieving a beautiful “after” result is only half the journey; maintaining it requires lifelong dedication. Patients must adopt a rigorous home care routine. Understanding How Long Should You Brush Your Teeth? Clinical Guide | HCMC Dental is vital, as thorough plaque removal prevents peri-implantitis (infection around implants) and secondary decay around natural tooth margins. Using non-abrasive toothpaste is also recommended to avoid scratching the polished surfaces of ceramic crowns and veneers.
Furthermore, patients often wonder, Is Fluoride Bad for Your Teeth? Clinical Facts & Safety | HCMC Dental. In the context of reconstructive maintenance, topical fluoride remains a critical tool for protecting any remaining natural tooth structure from decay, ensuring the foundation of the reconstruction remains solid.
Professional maintenance is equally non-negotiable. Knowing How Often Should You Go to the Dentist? | HCMC Dental changes after a full mouth reconstruction. Patients are typically placed on a three-to-four-month recall schedule for professional cleanings and occlusal adjustments. During these visits, the clinician will verify that the bite remains balanced and that no excessive forces are being placed on individual restorations. For patients with a history of bruxism, wearing a custom-fitted occlusal night guard is mandatory to protect the ceramic restorations from fracture during sleep.

Conclusion
Dental reconstruction before and after transformations represent the pinnacle of modern restorative dentistry. By addressing complex functional and aesthetic deficits through a coordinated, multi-disciplinary approach, clinicians can rebuild a patient’s smile from the foundation up. While the process requires a significant investment of time and resources, the resulting improvements in masticatory function, facial aesthetics, and overall quality of life are truly life-changing. With proper planning, expert execution, and diligent maintenance, a fully reconstructed smile can provide decades of health and confidence.
If you are experiencing severe dental wear, chronic jaw pain, or multiple missing teeth, scheduling a comprehensive consultation is the first step toward a restored smile. Contact General Dentistry tại HCMC Dental Clinic in Ho Chi Minh City to explore your personalized reconstructive options and begin your journey toward optimal oral health.
References
- Journal of Prosthetic Dentistry. Biomechanics of full-arch implant-supported restorations. (2021).
- International Journal of Periodontics & Restorative Dentistry. Vertical dimension of occlusion in full mouth rehabilitation. (2020).
- Clinical Oral Implants Research. Long-term survival rates of dental implants in reconstructed maxillae. (2019).
- Journal of the American Dental Association. Multidisciplinary approaches to severe occlusal wear. (2022).
- Journal of Clinical Orthodontics. Integrating orthodontic and prosthodontic treatment plans. (2018).
- Vietnam Odonto-Stomatology Association (VOSA). National guidelines on comprehensive dental rehabilitation and prosthodontics. (2023).