Charcoal teeth whitening utilizes the abrasive and porous properties of activated carbon to scrub away surface stains. However, clinical evidence shows it cannot alter the intrinsic color of teeth and poses significant risks of irreversible enamel wear and heightened tooth sensitivity if used improperly.
Clinical Summary:
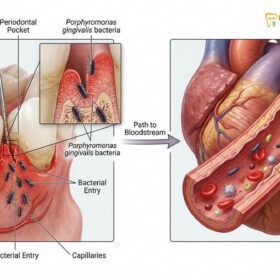
Activated charcoal has gained immense popularity as an over-the-counter dental cosmetic trend, heavily marketed for its purported ability to act as a natural dental detoxifier and stain remover. From a clinical perspective, the mechanism of charcoal relies entirely on mechanical abrasion and the adsorption of extrinsic chromophores (surface stains) caused by coffee, tea, or tobacco. Unlike professional peroxide-based bleaching agents, charcoal lacks the chemical capacity to penetrate the enamel matrix and oxidize intrinsic discoloration. Furthermore, dental professionals warn that the unregulated Relative Dentin Abrasivity (RDA) of many charcoal powders and toothpastes can lead to severe structural damage. Prolonged use frequently results in enamel thinning, dentinal hypersensitivity, gingival irritation, and an increased risk of dental caries due to the common omission of fluoride in these formulations. Patients seeking a brighter smile are strongly advised to undergo a comprehensive clinical assessment to determine the safest, evidence-based whitening protocol tailored to their specific oral anatomy.
Key Takeaways:
- Charcoal products only remove superficial extrinsic stains through physical abrasion and cannot lighten the intrinsic shade of the tooth.
- The high abrasivity of activated carbon can cause irreversible enamel loss, ultimately making teeth appear more yellow as the underlying dentin is exposed.
- Many charcoal toothpastes lack fluoride, significantly increasing the patient’s susceptibility to tooth decay and demineralization.
- Charcoal particles can become lodged in the gingival margins or microscopic cracks in teeth, causing localized inflammation and dark discoloration.
- Professional, supervised treatments using hydrogen or carbamide peroxide remain the only clinically proven methods for safe and effective intrinsic teeth whitening.
The Clinical Mechanism of Charcoal Teeth Whitening
Activated charcoal binds to surface deposits through adsorption and physically scrubs away extrinsic stains via abrasive action, but it lacks the chemical ability to bleach the internal tooth structure.
To understand how charcoal teeth whitening functions, it is essential to examine the physical and chemical properties of activated carbon. Activated charcoal is a fine, black powder created by super-heating natural sources—such as coconut shells, wood, or peat—in the presence of a gas. This activation process develops a highly porous internal structure, vastly increasing the material’s surface area. In medicine, this porosity is utilized in emergency toxicology to adsorb ingested toxins in the gastrointestinal tract. In dentistry, manufacturers have co-opted this concept, claiming that the material can “detoxify” the mouth and draw out stains.
When applied to the dentition, the mechanism of action is twofold: adsorption and mechanical abrasion. The acquired pellicle—a proteinaceous film that forms naturally on the enamel surface—often harbors extrinsic chromophores derived from dietary tannins, chromogenic foods, and tobacco. The porous nature of the charcoal allows it to bind to these surface deposits. Simultaneously, the gritty texture of the carbon particles acts as a mechanical exfoliant, physically scraping the stained pellicle away from the enamel surface during the brushing process.[1]

However, a critical clinical distinction must be made between stain removal and true tooth bleaching. The color of a human tooth is determined by the combination of the translucent outer enamel layer and the opaque, yellowish dentin layer beneath it. While charcoal can effectively remove superficial debris, its large molecular size and lack of oxidative properties prevent it from penetrating the enamel rods. Therefore, it cannot alter the intrinsic color of the dentin or reverse age-related yellowing. Patients often perceive an immediate brightening effect simply because the opaque surface debris has been scrubbed away, not because the tooth itself has been chemically lightened.
Efficacy: Does Activated Charcoal Actually Whiten Teeth?
Clinical trials indicate that charcoal-based products offer minimal whitening effects compared to standard peroxide treatments, primarily acting as aggressive mechanical exfoliants rather than true bleaching agents.
The efficacy of charcoal as a whitening agent has been extensively evaluated in modern dental literature. Randomized controlled clinical trials comparing activated charcoal powders and toothpastes against conventional fluoridated toothpastes and professional peroxide agents have yielded definitive results. According to these studies, charcoal-based products render significantly lower clinical esthetic outcomes when compared to established bleaching protocols.[2]
In a clinical setting, the efficacy of a whitening product is measured using objective colorimetry (such as the CIELAB color space) and subjective shade guides. Research demonstrates that while charcoal dentifrices may produce a slight reduction in surface yellowness (Δb* values) by removing extrinsic stains, they fail to produce the significant changes in lightness (ΔL* values) that characterize true whitening. In contrast, agents containing 10% carbamide peroxide consistently result in the highest prevalence of patient satisfaction and measurable whiteness effect.[3]
“Current clinical evidence does not support the efficacy of charcoal-based dentifrices for intrinsic tooth bleaching. Their action is limited to the mechanical removal of extrinsic stains, often at the unacceptable cost of irreversible enamel surface degradation.”
Furthermore, the perceived efficacy of charcoal is often short-lived. Because the abrasive action creates microscopic scratches on the enamel surface, the teeth actually become more susceptible to future staining. The roughened enamel provides a larger surface area for new chromophores and plaque to adhere to, creating a cyclical dependency where the patient feels compelled to use the abrasive powder more frequently to maintain the initial result. For patients seeking a reliable and lasting transformation, exploring professional teeth whitening protocols is the only evidence-based approach.
Dental Risks and Side Effects of Charcoal Products
The primary dangers of charcoal toothpaste include irreversible enamel abrasion, increased dentin hypersensitivity, gingival irritation, and the frequent absence of protective fluoride in these formulations.
The widespread adoption of charcoal teeth whitening has raised significant alarms within the global dental community due to the severe risks associated with its unregulated use. The most pressing clinical concern is the material’s abrasivity. Dental products are measured by their Relative Dentin Abrasivity (RDA). While the American Dental Association (ADA) recommends an RDA limit of 250 for safe daily use, many over-the-counter charcoal powders far exceed safe thresholds, acting more like sandpaper than a therapeutic dentifrice.[4]
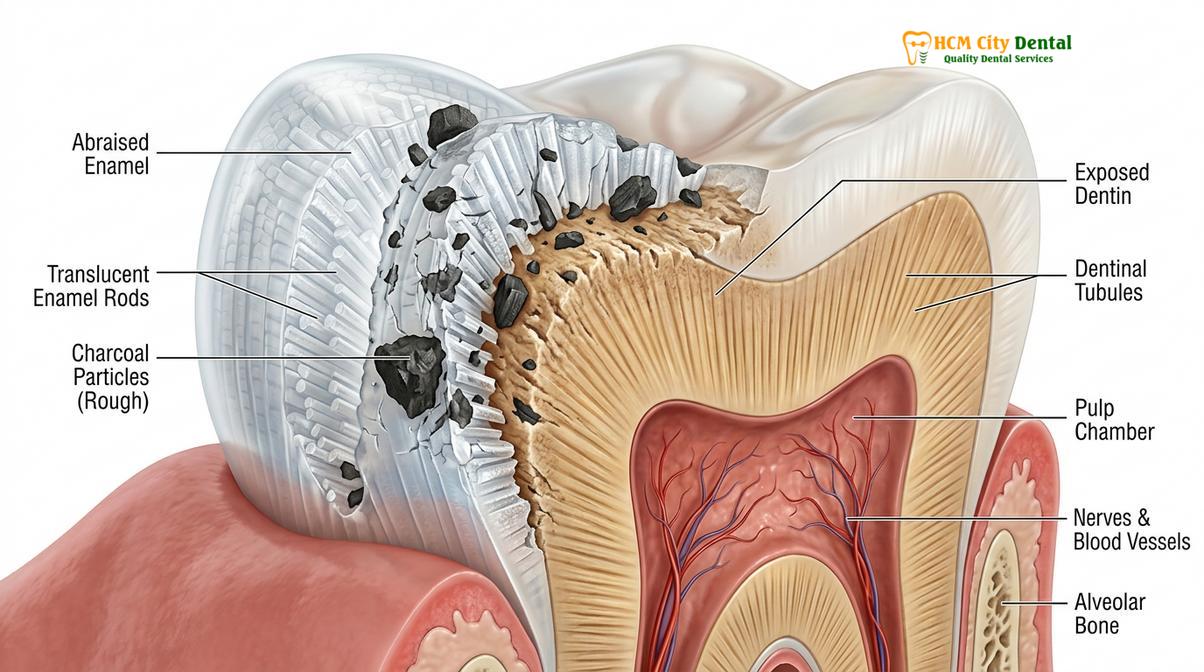
When highly abrasive substances are repeatedly applied to the teeth, they cause mechanical wear of the enamel layer. Enamel is the hardest substance in the human body, but it is acellular and cannot regenerate once lost. As the translucent enamel thins, the underlying dentin—which is naturally yellow—becomes more visible. Paradoxically, aggressive use of charcoal to achieve white teeth ultimately results in a permanently yellowed smile. Furthermore, the loss of enamel exposes the dentinal tubules, leading to severe dentinal hypersensitivity. Patients often report sharp, shooting pain when consuming hot, cold, or sweet stimuli.
Clinical Warning: The use of highly abrasive charcoal powders can cause irreversible enamel loss. Once enamel is worn away, it cannot grow back, leading to permanent tooth sensitivity, increased risk of decay, and a darker tooth appearance as the yellow dentin is exposed. Always consult a dental professional before using abrasive cosmetic products.
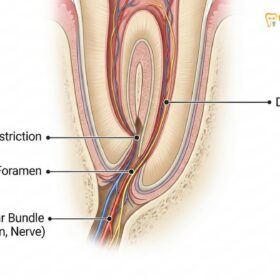
Beyond hard tissue damage, charcoal presents risks to the soft tissues and existing dental work. The insoluble carbon particles can become lodged in the gingival sulcus (the space between the tooth and the gum), causing localized inflammation, foreign body reactions, and a phenomenon known as “gingival tattooing,” where the gums take on a dark, grayish hue. Additionally, charcoal can scratch the polished surfaces of composite resins, porcelain veneers, and crowns, degrading their aesthetic appearance and structural integrity. Finally, a vast majority of charcoal toothpastes are marketed as “fluoride-free” or “natural.” The exclusion of fluoride deprives the teeth of essential remineralization, drastically increasing the patient’s risk of developing dental caries. Understanding the clinical safety of fluoride is crucial for maintaining long-term oral health.
Professional Alternatives to Charcoal Whitening
Evidence-based dentistry relies on hydrogen peroxide and carbamide peroxide formulations to safely penetrate enamel and oxidize intrinsic stains under professional supervision.
Given the limitations and risks associated with charcoal teeth whitening, dental professionals advocate for scientifically validated bleaching methods. Professional whitening relies on the oxidative power of hydrogen peroxide (H₂O₂) or its stable derivative, carbamide peroxide. When applied to the teeth, these chemical agents break down into water and reactive oxygen species (free radicals). These free radicals are small enough to diffuse through the enamel matrix and into the dentin, where they break the double bonds of large, pigmented chromophore molecules, rendering them colorless.[5]

Professional whitening is generally categorized into two main workflows:
- In-Office Power Bleaching: This procedure utilizes high-concentration hydrogen peroxide (typically 25% to 40%). Because of the high concentration, the dentist must carefully isolate the soft tissues using a light-cured gingival barrier to prevent chemical burns. The gel is applied to the teeth and may be accelerated using a specialized LED or halogen light source. This method provides immediate, dramatic results in a single visit.
- Custom Take-Home Trays: The dentist takes precise impressions or digital scans of the patient’s dentition to fabricate custom-fitting thermoplastic trays. The patient is provided with a lower-concentration carbamide peroxide gel (typically 10% to 16%) to wear at home for a specified duration (e.g., overnight or a few hours daily). The custom fit ensures the gel remains in contact with the teeth and away from the gums, providing gradual, highly effective, and safe whitening.
To clearly illustrate the differences between these approaches, the following table outlines the clinical parameters of charcoal versus professional peroxide treatments:
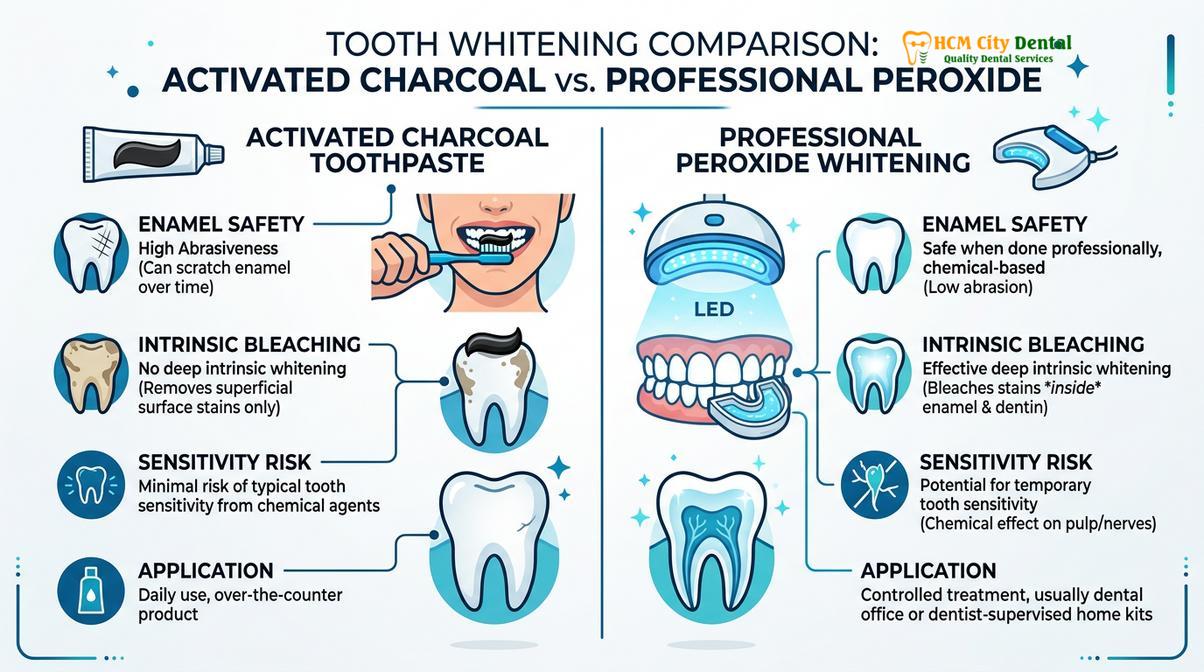
| Clinical Parameter | Activated Charcoal Products | Professional Peroxide Whitening |
|---|---|---|
| Mechanism of Action | Mechanical abrasion and surface adsorption | Chemical oxidation of intrinsic chromophores |
| Target Stains | Extrinsic (surface) stains only | Both extrinsic and intrinsic discoloration |
| Enamel Safety | High risk of irreversible abrasion and thinning | Safe when supervised; does not remove enamel |
| Sensitivity Risk | High (due to structural enamel loss and dentin exposure) | Moderate (transient chemical sensitivity, fully reversible) |
| Regulatory Approval | Rarely ADA approved; highly variable RDA levels | Strictly regulated; ADA approved formulations |
For patients seeking a comprehensive approach to their oral health, integrating safe cosmetic procedures with routine care is essential. Reviewing a comprehensive general dental care guide can help patients make informed decisions about their treatment options.
Clinical Case Study: Managing Enamel Wear from Charcoal Powder
Prolonged use of abrasive charcoal powders often leads to severe enamel thinning, requiring restorative interventions and professional desensitization protocols to repair the damaged dentition.
The theoretical risks of charcoal teeth whitening frequently manifest as severe clinical complications. At HCMC Dental Clinic in Ho Chi Minh City, our specialists frequently encounter patients who have inadvertently damaged their dentition through the misuse of trending cosmetic products.
Patient Profile: A 28-year-old female presented to HCMC Dental Clinic complaining of severe, sharp pain when drinking cold water and a noticeable yellowing of her anterior teeth over the past six months.
Clinical Assessment: Dr. Nguyen Van Cuong conducted a thorough clinical examination, utilizing transillumination and tactile assessment. The examination revealed significant loss of the labial enamel on the maxillary incisors, exposing the underlying dentin. The enamel surface appeared dull, scratched, and lacked its natural luster. The gingival margins showed mild inflammation with microscopic black particles embedded in the sulcus.
Diagnosis: Severe dentinal hypersensitivity and irreversible enamel abrasion secondary to the daily use of an unregulated, highly abrasive activated charcoal powder.
Treatment Protocol:
1. Immediate cessation of all charcoal-based products.
2. Application of a high-concentration in-office fluoride varnish to occlude the exposed dentinal tubules and provide immediate relief from hypersensitivity.
3. Prescription of a remineralizing toothpaste containing nano-hydroxyapatite and potassium nitrate for daily home use.
4. A follow-up restorative plan involving minimally invasive composite resin bonding to restore the lost enamel volume, protect the dentin, and re-establish the aesthetic white appearance of the incisors.
Outcome: Within two weeks, the patient’s sensitivity was fully resolved. The composite restorations successfully masked the yellow dentin, restoring her smile safely without further compromising her tooth structure.
This case highlights the critical importance of professional oversight. What begins as an attempt to achieve a brighter smile at home can quickly escalate into a complex restorative necessity. Patients must prioritize the structural integrity of their teeth over unverified cosmetic trends.
Safe Oral Hygiene Practices for Stain Prevention
Maintaining a bright smile safely involves using ADA-approved fluoridated toothpaste, practicing proper brushing techniques, and managing the intake of chromogenic foods and beverages.
Rather than resorting to aggressive abrasives, patients can maintain a naturally bright and healthy smile through evidence-based oral hygiene practices. The foundation of stain prevention is the effective, non-destructive removal of dental plaque before it can calcify into calculus (tartar), which is highly porous and rapidly absorbs stains.
Dental professionals recommend brushing twice daily using the Modified Bass technique. This involves placing a soft-bristled toothbrush at a 45-degree angle to the gingival margin and using gentle, short, circular motions. This technique effectively disrupts the plaque biofilm without traumatizing the soft tissues or abrading the enamel. Understanding optimal brushing duration and technique is far more effective for stain control than using harsh chemicals or powders.
“The preservation of enamel is paramount in cosmetic dentistry. A healthy, intact enamel layer is naturally glossy and reflects light beautifully. Destroying this layer with abrasives to remove a temporary stain is a clinical misstep that compromises the tooth for a lifetime.”
Dietary modifications also play a crucial role in preventing discoloration. Minimizing the frequency of exposure to highly chromogenic substances—such as black tea, red wine, coffee, and dark berries—can significantly reduce extrinsic staining. When consuming these beverages, using a straw can help bypass the anterior teeth. Furthermore, maintaining adequate salivary flow is essential, as saliva naturally cleanses the oral cavity and neutralizes acidic challenges. Chronic dry mouth can exacerbate staining and even contribute to managing oral malodor, making hydration a key component of oral aesthetics.
When to See a Doctor for Tooth Discoloration
While mild surface staining is a normal part of aging and dietary habits, sudden or severe changes in tooth color warrant professional evaluation. If you have been using charcoal teeth whitening products and experience any of the following symptoms, it is imperative to schedule a clinical examination immediately:
- Heightened Sensitivity: A new or worsening sharp pain when consuming hot, cold, sweet, or acidic foods indicates that the protective enamel layer has been compromised, exposing the nerve-rich dentin.
- Increased Yellowness: If your teeth appear to be getting darker or more yellow despite frequent brushing, you may be wearing away the white enamel and exposing the dentin.
- Translucency at the Edges: Enamel wear often manifests first at the incisal edges (the biting surfaces) of the front teeth, making them look thin, gray, or transparent.
- Gum Irritation or Bleeding: Persistent redness, swelling, or bleeding of the gums, especially if accompanied by dark lines along the gumline, suggests that abrasive particles are causing mechanical trauma or foreign body reactions.

A qualified dental professional possesses the diagnostic tools necessary to differentiate between extrinsic stains, intrinsic discoloration, and structural damage. Through transillumination, vitality testing, and radiographic imaging, a dentist can accurately diagnose the cause of the discoloration and recommend a safe, effective treatment plan. Knowing selecting a qualified dental professional is the first step toward achieving your aesthetic goals without compromising your health. Dr. Nguyen Van Cuong and the expert team at HCMC Dental Clinic in Ho Chi Minh City are dedicated to providing evidence-based cosmetic solutions that prioritize the long-term vitality of your smile. We encourage patients to maintain routine dental examinations to monitor enamel health and discuss safe whitening options.
Frequently Asked Questions
Does charcoal toothpaste actually whiten teeth?
Charcoal toothpaste only removes superficial extrinsic stains through mechanical abrasion. It does not contain bleaching agents capable of altering the intrinsic color of your teeth, meaning it cannot lighten the actual shade of your enamel. For true whitening, peroxide-based agents are required to penetrate the tooth structure and oxidize internal pigments.
Is it safe to brush with activated charcoal every day?
No, brushing with activated charcoal daily is highly discouraged by dental professionals. Its high abrasivity can rapidly wear down tooth enamel, leading to irreversible damage, dentin exposure, and severe tooth sensitivity over time. Daily oral hygiene should rely on low-abrasion, fluoridated toothpastes approved by dental associations.
Can charcoal powder damage my dental restorations?
Yes, charcoal powder can scratch and degrade the surface of dental restorations. Veneers, crowns, and composite fillings can lose their polished finish, and the dark particles may become permanently trapped in the margins of the restorations, leading to aesthetic failure and potential microleakage.
Why do my teeth look more yellow after using charcoal?
Teeth appear more yellow after prolonged charcoal use because the abrasive particles wear away the white, translucent enamel layer. This exposes the underlying dentin, which is naturally yellow, permanently altering the tooth’s appearance. Once this enamel is lost, it cannot be regenerated naturally.
What is the safest way to whiten sensitive teeth?
The safest method for whitening sensitive teeth is a professionally supervised treatment using low-concentration carbamide peroxide combined with desensitizing agents like potassium nitrate. A clinical evaluation is necessary to customize the protocol, ensuring the whitening process is effective without exacerbating existing hypersensitivity.
References
- Journal of Dentistry. Whitening efficacy of activated charcoal-based products: A randomized controlled clinical trial. (2024).
- Journal of the American Dental Association. Charcoal and charcoal-based dentifrices: A literature review. (2017).
- Clinical Oral Investigations. Abrasivity and whitening efficacy of charcoal toothpastes. (2019).
- Operative Dentistry. Effects of charcoal toothpaste on enamel surface roughness and microhardness. (2021).
- British Dental Journal. The risks of non-fluoridated charcoal toothpastes and gingival tattooing. (2020).