A “dental heart attack” refers to the systemic cardiovascular events, such as myocardial infarction, triggered or exacerbated by severe oral infections like periodontitis. Pathogenic oral bacteria enter the bloodstream, promoting arterial inflammation, plaque rupture, and blood clot formation that can obstruct coronary arteries.
Clinical Summary:
The correlation between periodontal disease and cardiovascular events is driven by systemic inflammation and transient bacteremia. Oral pathogens such as Porphyromonas gingivalis can enter the bloodstream, elevating C-reactive protein (CRP) levels and accelerating atherosclerosis. Clinical management requires a multidisciplinary approach, combining rigorous periodontal therapy with cardiovascular risk assessment to mitigate the potential for a dental-induced heart attack. Regular professional cleanings, early intervention, and strict adherence to clinical protocols are critical for high-risk patients.
Key Takeaways:
- Oral bacteria can breach the gingival barrier, entering the bloodstream and contributing to arterial plaque formation.
- Chronic gum inflammation elevates systemic markers like CRP, significantly increasing cardiovascular risk.
- Treating periodontitis through mechanical debridement may help reduce the systemic inflammatory burden on the heart.
- Patients with existing heart conditions require specialized dental protocols, including stress reduction and possible antibiotic prophylaxis.
- Routine dental examinations are a vital component of comprehensive cardiovascular care and systemic health maintenance.
The Pathophysiology: How Oral Bacteria Reach the Heart
The connection between oral health and cardiovascular disease is primarily mediated through transient bacteremia and chronic systemic inflammation originating from infected periodontal pockets.
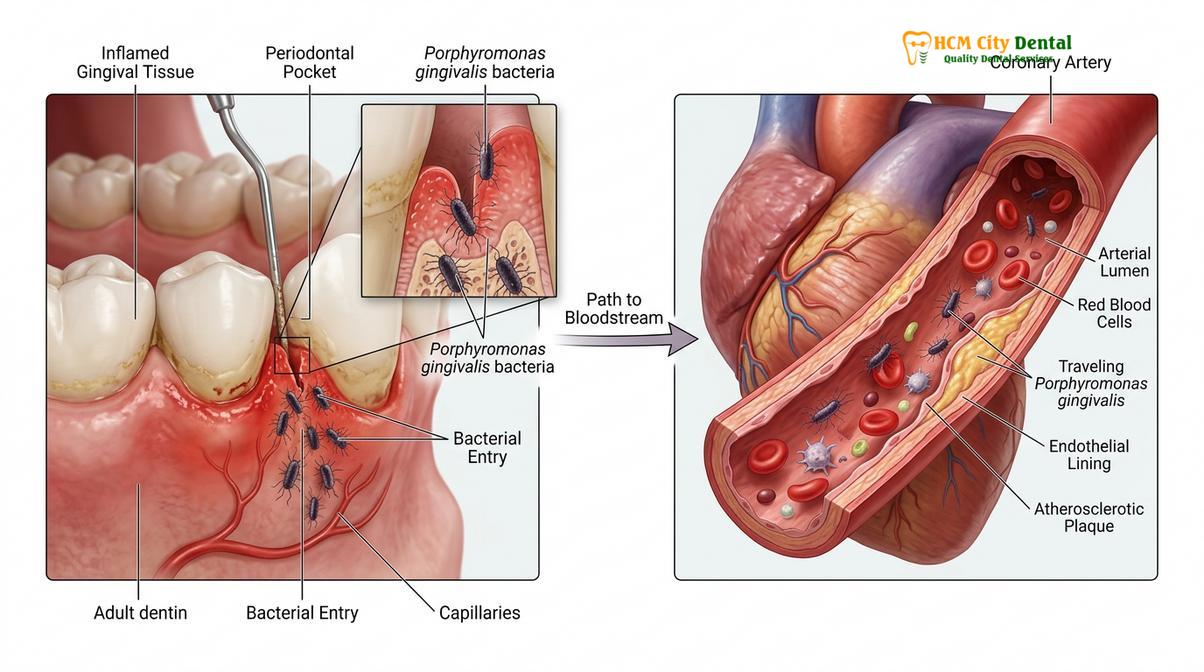
The oral cavity is a complex ecosystem harboring hundreds of bacterial species. In a state of health, these microorganisms exist in a symbiotic balance. However, when oral hygiene is compromised, pathogenic biofilms accumulate, leading to gingivitis and, eventually, severe periodontitis. The concept of a “dental heart attack” stems from the systemic dissemination of these localized oral infections. The highly vascularized nature of inflamed gingival tissue provides a direct portal of entry for bacteria into the systemic circulation, a phenomenon known as transient bacteremia[1].
Once in the bloodstream, specific periodontal pathogens, most notably Porphyromonas gingivalis and Streptococcus mutans, exert profound effects on the cardiovascular system. These bacteria possess virulence factors that allow them to adhere to the endothelial lining of blood vessels. P. gingivalis, for instance, secretes enzymes called gingipains that degrade host proteins and activate coagulation pathways. This bacterial presence induces platelet activation and aggregation, which are critical early steps in thrombus (blood clot) formation[2]. If a thrombus forms in a coronary artery, it can obstruct blood flow to the myocardium, precipitating a myocardial infarction.
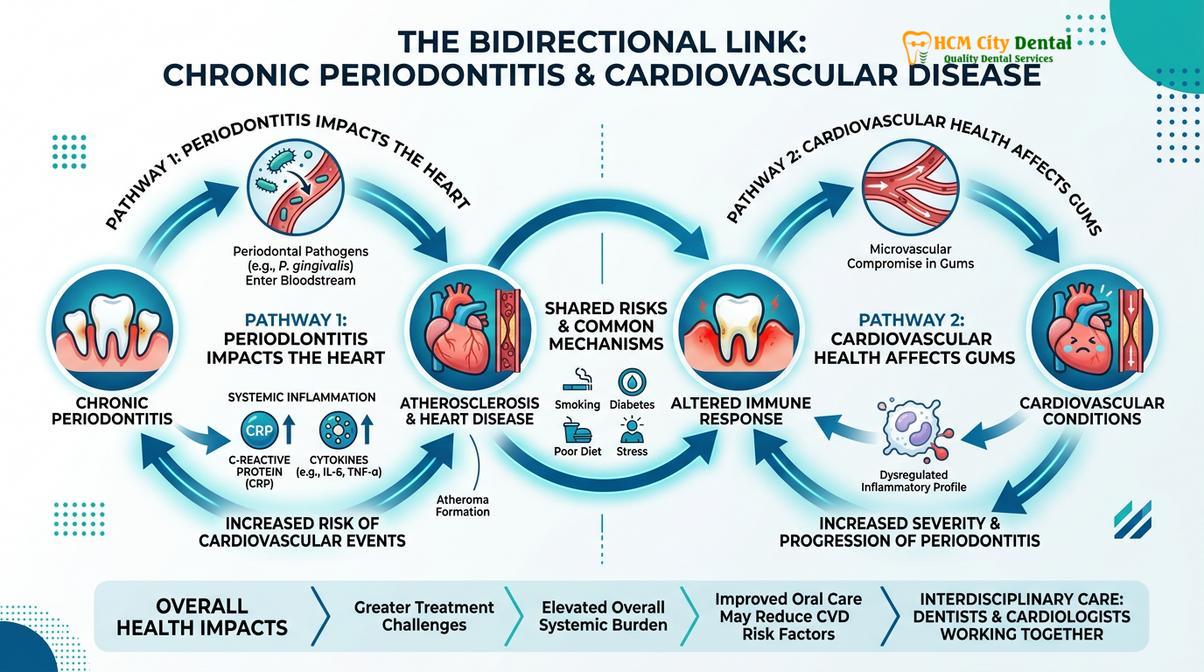
Beyond direct bacterial invasion, the systemic immune response plays a pivotal role. Chronic periodontitis acts as a persistent reservoir of inflammatory mediators. The localized immune response in the gums results in the spillover of pro-inflammatory cytokines—such as Interleukin-1 (IL-1), Interleukin-6 (IL-6), and Tumor Necrosis Factor-alpha (TNF-α)—into the systemic circulation. The liver responds to these cytokines by producing acute-phase reactants, particularly C-reactive protein (CRP)[3]. Elevated high-sensitivity CRP is a well-established independent risk factor for cardiovascular disease. This systemic inflammation promotes endothelial dysfunction, increases the uptake of low-density lipoproteins (LDL) by macrophages, and accelerates the formation of atherosclerotic plaques. Furthermore, inflammation destabilizes existing plaques, making them more prone to rupture, which is the primary mechanism behind acute coronary syndromes.
“The oral cavity is not an isolated system; chronic periodontal inflammation acts as a systemic burden, continuously challenging the cardiovascular endothelium and accelerating atherogenic processes.”
Understanding this intricate pathophysiology underscores the importance of comprehensive comprehensive general dentistry. Routine examinations and cleanings are not merely cosmetic procedures; they are essential interventions designed to disrupt pathogenic biofilms before they can exert systemic cardiovascular effects.
Recognizing the Warning Signs in the Oral Cavity
Identifying early signs of severe gum disease, such as persistent bleeding and deep periodontal pockets, is crucial for preventing systemic bacterial dissemination and reducing cardiovascular risk.
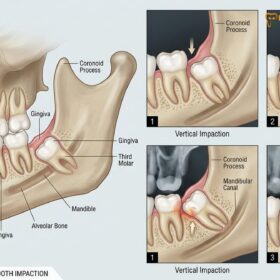
Preventing a systemic crisis begins with recognizing the localized signs of periodontal breakdown. Gingivitis, the earliest stage of gum disease, is characterized by red, swollen gums that bleed easily during brushing or flossing. While gingivitis is reversible, if left untreated, it progresses to periodontitis. In periodontitis, the inflammatory response destroys the connective tissue and alveolar bone supporting the teeth, creating deep periodontal pockets. These pockets become anaerobic environments, ideal for the proliferation of highly virulent, gram-negative bacteria.
Clinical indicators of advanced periodontal disease include persistent halitosis (bad breath), gingival recession, purulent exudate (pus) expressing from the gumline, and progressive tooth mobility. Dr. Nguyen Van Cuong frequently emphasizes during clinical consultations that bleeding gums should never be considered normal; they are a definitive sign of an open wound in the mouth, allowing bacteria direct access to the vascular system. When evaluating patients, dental professionals meticulously measure pocket depths using a periodontal probe. Pockets exceeding 4 millimeters, especially those that bleed upon probing, indicate active disease and a higher risk for systemic bacterial translocation.

Clinical Red Flags for Systemic Risk:
- Spontaneous gingival bleeding or profuse bleeding during routine oral hygiene.
- Deep periodontal pockets (≥ 5mm) with clinical attachment loss.
- Purulent discharge (pus) from the gingival sulcus.
- Sudden changes in the fit of partial dentures or shifting of teeth.
- Chronic, unresolved oral inflammation despite basic home care.
Patients exhibiting these symptoms require immediate clinical intervention. The presence of severe, generalized periodontitis significantly elevates the patient’s inflammatory burden. In some cases, severely compromised teeth that cannot be saved through periodontal therapy may require extraction to eliminate the source of chronic infection. When planning such procedures, clinicians must carefully evaluate evaluating whether complex extractions require a hospital setting, particularly for patients with known cardiovascular comorbidities who may require advanced monitoring.
Clinical Management and Preventive Dental Workflows
Effective clinical management involves mechanical debridement, antimicrobial therapy, and rigorous maintenance protocols to eradicate pathogenic biofilms and reduce systemic inflammatory markers.
The cornerstone of mitigating the cardiovascular risks associated with periodontal disease is non-surgical periodontal therapy, primarily scaling and root planing (SRP). This meticulous procedure involves the mechanical removal of calcified plaque (calculus) and bacterial biofilms from the tooth surfaces, both above and below the gumline. Ultrasonic scalers, which utilize high-frequency vibrations and water irrigation, are employed to disrupt the biofilm and flush out bacteria, followed by hand instrumentation to smooth the root surfaces. Smoothing the roots prevents further bacterial adherence and facilitates the reattachment of healthy gingival tissue[4].
The execution of these therapies relies heavily on highly trained dental professionals. Students pursuing a dental hygienist major learn early in their academic careers that systemic health is deeply tied to oral hygiene. The curriculum is intensely focused on microbiology, head and neck anatomy, and systemic pathology. A typical day in the life of a dental hygienist involves far more than polishing teeth; it requires meticulous calculus removal, periodontal charting, and educating patients on the systemic implications of their oral health. Patients often ask how long does it take to become a dental hygienist; this rigorous training, typically requiring two to four years of specialized education, ensures they possess the clinical acumen to identify systemic risk factors and perform complex debridement procedures safely.

Following active therapy, patients are placed on a strict periodontal maintenance schedule, usually requiring visits every three to four months. This frequency is critical because pathogenic bacteria can repopulate periodontal pockets within 90 to 120 days. During these maintenance visits, clinicians reassess pocket depths, monitor bleeding indices, and perform targeted debridement to maintain a stable, non-inflammatory state. In some cases, adjunctive therapies such as localized antibiotic delivery or antimicrobial mouth rinses (e.g., chlorhexidine gluconate) are prescribed to further suppress the bacterial load.
| Periodontal Stage | Clinical Presentation | Systemic Inflammatory Burden | Cardiovascular Risk Implication |
|---|---|---|---|
| Gingivitis | Gingival erythema, bleeding on probing, no bone loss. | Mild, localized inflammation. | Low, but requires intervention to prevent progression. |
| Stage I-II Periodontitis | Pocket depths 4-5mm, mild to moderate bone loss. | Moderate systemic cytokine release. | Elevated risk; early endothelial stress possible. |
| Stage III-IV Periodontitis | Pocket depths ≥ 6mm, severe bone loss, tooth mobility. | High systemic CRP and pro-inflammatory markers. | Significant risk factor for atherogenesis and thrombotic events. |
It is also vital to educate patients on the risks of unverified dental trends that can compromise gingival health. For instance, the use of highly abrasive substances can damage the enamel and irritate the gums, exacerbating inflammation. Clinicians frequently advise against abrasive cosmetic trends like charcoal teeth whitening, advocating instead for evidence-based, professionally supervised treatments that preserve the integrity of the periodontium.
Evaluating the Risks: Dental Procedures for Cardiac Patients
Treating patients with a history of cardiovascular disease requires strict adherence to clinical guidelines, including stress reduction protocols and appropriate antibiotic prophylaxis.
When treating patients who have already experienced cardiovascular events or possess significant cardiac risk factors, the dental workflow must be meticulously adapted. The primary goals are to prevent infective endocarditis, manage bleeding risks associated with anticoagulant therapy, and minimize cardiovascular stress during procedures. A comprehensive medical history review is mandatory before initiating any treatment.
For patients with specific cardiac conditions—such as prosthetic heart valves, previous infective endocarditis, or certain congenital heart defects—the American Heart Association mandates antibiotic prophylaxis prior to dental procedures that involve manipulation of gingival tissue or the periapical region of teeth[5]. This premedication prevents transient bacteremia from colonizing vulnerable cardiac structures. However, it is equally important to note that routine antibiotic use is not recommended for patients with simple coronary artery disease or stents, highlighting the need for precise clinical judgment.
Pharmacological considerations also play a major role. Many cardiac patients are prescribed antithrombotic medications (e.g., warfarin, clopidogrel, or novel oral anticoagulants). Dental professionals must balance the risk of postoperative bleeding against the risk of a thromboembolic event if the medication is altered. Generally, most routine dental procedures, including simple extractions, can be performed safely without altering anticoagulant regimens, provided local hemostatic measures are employed. Furthermore, the use of local anesthetics containing epinephrine must be carefully titrated. While epinephrine provides profound anesthesia and local hemostasis, excessive amounts can induce tachycardia and elevate blood pressure, stressing the myocardium.
Clinical Case Review: Managing a High-Risk Cardiac Patient
A 62-year-old male patient presented to HCMC Dental Clinic in Ho Chi Minh City with severe generalized periodontitis and a history of a myocardial infarction two years prior. He was currently taking a daily antiplatelet medication and a beta-blocker. The clinical objective was to eliminate oral infection without triggering a cardiovascular event.
Dr. Nguyen Van Cuong developed a phased treatment plan. Instead of a single, lengthy appointment, the periodontal debridement was divided into four shorter sessions to minimize physical and psychological stress. A stress-reduction protocol was implemented, utilizing profound local anesthesia with a cardiac-safe dosage of epinephrine. Local hemostatic agents were prepared to manage any prolonged bleeding due to his antiplatelet therapy. Over six months, the patient’s periodontal pockets reduced significantly, bleeding on probing was eliminated, and his cardiologist noted a concurrent stabilization in his systemic inflammatory markers.
Surgical interventions in cardiac patients require even greater scrutiny. Understanding the dangers of dental implants in patients with uncontrolled cardiovascular disease is paramount, as surgical stress, prolonged chair time, and potential postoperative infection can trigger adverse systemic events. Thorough preoperative cardiovascular clearance is often required before embarking on complex procedures like full mouth dental reconstruction or extensive surgical extraction planning.
Differential Diagnosis: Odontogenic Pain vs. Referred Cardiac Pain
A critical aspect of the “dental heart attack” concept is the diagnostic overlap between severe dental pain and the referred pain of a myocardial infarction. The sensory innervation of the lower jaw and the heart share complex neural pathways. During an ischemic cardiac event (angina or a heart attack), the brain can misinterpret the pain signals originating from the heart muscle as coming from the mandible, teeth, or neck[6].
Dental professionals are trained to differentiate between odontogenic (tooth-related) pain and referred cardiac pain. Odontogenic pain is typically localized, easily reproduced by thermal stimuli (hot or cold) or percussion (tapping the tooth), and often associated with a specific, identifiable dental pathology such as deep decay or an abscess. In contrast, referred cardiac pain in the jaw is usually bilateral, described as a deep, aching pressure or tightness, and is not exacerbated by chewing or thermal changes. Crucially, cardiac jaw pain often worsens with physical exertion and improves with rest or the administration of nitroglycerin.
“The sudden onset of bilateral mandibular pain, especially when accompanied by diaphoresis, shortness of breath, or chest pressure, must be treated as a cardiac emergency until proven otherwise, regardless of the patient’s dental status.”
If a patient presents to the dental office complaining of jaw pain that lacks a clear dental etiology, the clinician must maintain a high index of suspicion for a cardiovascular event, immediately assess the patient’s vital signs, and activate emergency medical services if necessary. This diagnostic vigilance is a fundamental component of patient safety in the dental setting.
When to See a Doctor
Distinguishing between a routine dental issue and a medical emergency is vital for patient safety. You should seek immediate emergency medical attention (call an ambulance or go to the nearest emergency room) if you experience jaw pain that is accompanied by any of the following symptoms:
- Crushing, squeezing, or heavy pressure in the center of the chest.
- Pain radiating down the left arm, into the neck, or between the shoulder blades.
- Shortness of breath, severe dizziness, or unexplained sweating (diaphoresis).
- Nausea, vomiting, or a feeling of impending doom.
- Jaw pain that worsens with physical exertion and subsides with rest.
Conversely, you should schedule a prompt evaluation with a dental professional if you notice signs of severe oral infection that could increase your systemic risk profile. These include:
- Gums that bleed profusely during normal brushing or flossing.
- Visible pus or a persistent foul taste/odor in the mouth.
- Teeth that feel loose or are shifting position.
- Swelling in the gums, face, or neck accompanied by a fever.
For patients requiring extensive dental work, such as structural orthodontic corrections or periodontal surgery, a collaborative approach between your dentist and cardiologist is highly recommended to ensure all treatments are performed safely and effectively.
Frequently Asked Questions
Can a tooth infection directly cause a heart attack?
A tooth infection does not directly cause a heart attack, but it significantly increases systemic risk. Chronic oral infections release bacteria and inflammatory cytokines into the bloodstream, which can accelerate atherosclerosis and promote blood clot formation in coronary arteries. Over time, this systemic inflammatory burden destabilizes arterial plaques, making a cardiovascular event more likely.
What are the dental symptoms that indicate a high risk for systemic health issues?
Severe periodontal symptoms indicate a higher systemic risk profile. These include persistent bleeding gums, deep periodontal pockets, purulent exudate (pus) around the gumline, chronic halitosis, and progressive tooth mobility, all of which suggest a high bacterial load. If you experience these symptoms, it is critical to seek professional periodontal therapy to reduce the risk of systemic bacterial dissemination.
Do I need antibiotics before a dental cleaning if I have a heart condition?
Antibiotic prophylaxis is required only for specific high-risk cardiac conditions. Patients with prosthetic heart valves, a history of infective endocarditis, or certain congenital heart defects typically require premedication to prevent bacterial colonization on heart tissues. However, patients with standard coronary artery disease, pacemakers, or stents generally do not require antibiotics prior to routine cleanings. Always consult your cardiologist and dentist for personalized guidelines.
How does treating gum disease improve cardiovascular health?
Treating gum disease reduces the systemic inflammatory burden on the cardiovascular system. By eradicating periodontal pathogens through deep cleaning, systemic markers of inflammation like C-reactive protein (CRP) decrease, potentially improving endothelial function and arterial health. Effective periodontal maintenance helps stabilize the immune response, thereby lowering the indirect risks associated with atherogenesis.
Is it safe to undergo oral surgery after a recent heart attack?
Elective oral surgery is generally postponed following a recent myocardial infarction. Dentists and cardiologists typically recommend waiting a specific recovery period, often several months, while managing acute dental infections conservatively with antibiotics and pain relief. When surgery is eventually performed, strict stress-reduction protocols, careful monitoring of vital signs, and precise management of local anesthetics and anticoagulants are mandatory.

References
- Journal of Periodontology. Systemic inflammation and cardiovascular risk in severe periodontitis. (2021).
- American Heart Association Journal. Periodontal disease and atherosclerotic vascular disease: scientific statement. (2020).
- International Journal of Cardiology. Porphyromonas gingivalis and its role in endothelial dysfunction. (2019).
- Journal of Clinical Periodontology. The impact of non-surgical periodontal therapy on systemic inflammatory markers. (2022).
- Journal of the American Dental Association. Antibiotic prophylaxis for infective endocarditis: clinical practice guidelines. (2021).
- British Dental Journal. Differentiating odontogenic pain from referred cardiac angina in dental practice. (2018).
For personalized advice regarding periodontal health and cardiovascular risk management, please contact the clinical team at HCMC Dental Clinic.