To understand how to brush teeth correctly, you must use a soft-bristled toothbrush and fluoride toothpaste for two full minutes twice daily. Angle the bristles at 45 degrees toward the gumline, employing gentle, circular sweeping motions to effectively remove plaque without damaging enamel or gingival tissues.
Clinical Summary:
Proper tooth brushing is a foundational preventive dental protocol designed to mechanically disrupt bacterial biofilm before it calcifies into calculus. The clinically recommended method, known as the Modified Bass Technique, requires angling a soft-bristled brush at 45 degrees to the gingival margin to clean the sulcus effectively. Combined with appropriately formulated fluoride toothpaste and a strict two-minute duration, this technique mitigates the risk of dental caries, periodontal disease, and associated systemic health complications. Regular professional evaluations and personalized hygiene instructions complement this daily regimen to ensure long-term, optimal oral health.
Key Takeaways:
- Brush for a minimum of 120 seconds, dividing the mouth into four 30-second quadrants for even coverage.
- Maintain a 45-degree bristle angle directed toward the gumline to clean the critical gingival sulcus.
- Utilize ultra-soft or soft bristles to prevent irreversible enamel abrasion and gingival recession.
- Incorporate clinically proven fluoride toothpaste to remineralize enamel and resist bacterial acid attacks.
- Replace your manual toothbrush or electric brush head every three to four months, or immediately when bristles fray.
The Clinical Importance of Proper Brushing Mechanics
Effective brushing mechanically disrupts bacterial biofilm before it calcifies into hard calculus, preventing localized oral diseases and reducing systemic inflammatory burdens.
The oral cavity is a complex, dynamic ecosystem harboring hundreds of distinct bacterial species. Within minutes after a professional dental cleaning, a glycoprotein layer known as the acquired pellicle forms over the enamel. This pellicle acts as a biological adhesive, allowing primary bacterial colonizers, such as Streptococcus sanguinis and Streptococcus mutans, to attach to the tooth surface. If these bacteria are not mechanically removed through proper brushing, they rapidly multiply, creating a sticky, highly organized matrix known as dental plaque or biofilm.
Understanding how to brush teeth correctly is fundamentally about biofilm management. When you consume fermentable carbohydrates—such as sugars and starches—the cariogenic bacteria within the plaque metabolize these substrates and excrete lactic acid as a byproduct. This acid lowers the local pH of the oral environment. When the pH drops below the critical threshold of 5.5, the hydroxyapatite crystals that make up your tooth enamel begin to demineralize, initiating the process of dental caries (cavities).

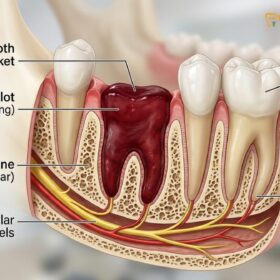
Furthermore, if plaque is allowed to stagnate along the gingival margin (the gumline) for more than 48 to 72 hours, it begins to absorb calcium and phosphate ions from your saliva. This biochemical process calcifies the soft plaque into a hardened substance known as calculus, or tartar. Unlike soft plaque, calculus cannot be removed by any toothbrush or home care device; it requires professional scaling using specialized ultrasonic and hand instruments. Calculus provides a rough, porous surface that attracts even more plaque, driving the bacteria deeper into the gingival sulcus (the shallow crevice between the tooth and the gum).
The presence of subgingival bacteria triggers a robust immune response. The body sends inflammatory cells to the area to fight the bacterial invasion, resulting in gingivitis—characterized by red, swollen, and bleeding gums. If left untreated, this localized inflammation can progress to periodontitis, a severe chronic inflammatory disease that destroys the periodontal ligament and alveolar bone supporting the teeth. Recent clinical literature strongly links this chronic oral inflammation to broader systemic health issues, including cardiovascular disease, poor glycemic control in diabetes, and even neurodegenerative conditions [1]. Therefore, mastering the mechanics of brushing is not merely a cosmetic endeavor; it is a critical component of comprehensive preventive medicine.
“The mechanical disruption of dental biofilm through meticulous daily brushing is the single most effective preventive measure against both dental caries and periodontal disease, serving as the first line of defense for systemic health.”
For patients seeking comprehensive care, establishing a baseline of oral health through General Dentistry is the first step in ensuring that home care efforts are effective and that any existing calculus is professionally removed.
Step-by-Step Clinical Protocol: The Modified Bass Technique
The optimal brushing method involves the Modified Bass Technique, utilizing a 45-degree angle and gentle circular motions for two minutes to clean both tooth surfaces and the gingival sulcus.
While many individuals brush their teeth daily, clinical observations reveal that a significant majority employ an improper, horizontal scrubbing motion. This aggressive technique not only fails to clean the critical areas where gum disease originates but also causes physical trauma to the oral tissues. The gold standard in dental hygiene instruction is the Modified Bass Technique. This method is specifically designed to clean the cervical third of the tooth and the gingival sulcus, which are the primary stagnation areas for pathogenic biofilm [2].
To execute the Modified Bass Technique correctly, follow this precise clinical workflow:
Step 1: Preparation and Dispensation
Begin with a dry or slightly moistened soft-bristled toothbrush. Apply a pea-sized amount of fluoridated toothpaste. Using excessive toothpaste creates excessive foam, which can cause premature spitting and reduce the actual brushing time. The goal is to maintain the fluoride concentration in the mouth for the full duration of the brushing cycle.
Step 2: Precise Angulation
Place the head of the toothbrush horizontally against the teeth. Tilt the brush so that the bristles are pointing toward the gumline at exactly a 45-degree angle. This specific angulation allows the longest bristles to gently slip beneath the gingival margin (into the sulcus) while the shorter bristles rest on the enamel surface. This is the most critical step in learning how to brush teeth correctly.
Step 3: The Micro-Vibratory Motion
Instead of long, horizontal scrubbing strokes, apply light pressure and move the brush in very short, micro-vibratory or circular motions. Keep the bristles in place while the handle moves. Vibrate the brush for about 10 to 15 seconds in one spot (covering two to three teeth at a time). After vibrating, use a sweeping or rolling motion to flick the bristles away from the gumline, sweeping the dislodged plaque toward the biting surface of the tooth.
Step 4: Systematic Progression
Move systematically through the mouth to ensure no areas are missed. A common clinical recommendation is to divide the mouth into four quadrants (upper right, upper left, lower left, lower right) and spend exactly 30 seconds on each. Clean the buccal (outer/cheek) surfaces first, then proceed to the lingual (inner/palatal) surfaces.
Step 5: Adapting to Anterior Lingual Surfaces
The inner surfaces of the front teeth (both upper and lower incisors) present an anatomical challenge due to the narrow arch curvature. To clean these areas effectively, hold the toothbrush vertically. Use the “heel” or “toe” (the very front or back) of the brush head to make gentle up-and-down strokes. The lingual surface of the lower front teeth is particularly prone to rapid calculus buildup because it sits directly opposite the submandibular salivary glands (Wharton’s duct), which constantly bathe the area in calcium-rich saliva.
Step 6: Occlusal Surfaces and Tongue Debridement
Finally, place the bristles flat against the occlusal (chewing) surfaces of the molars and premolars. Use a gentle back-and-forth scrubbing motion to clean the deep pits and fissures where food debris easily impacts. Conclude your routine by brushing the dorsum (top surface) of your tongue from back to front. The tongue’s papillae harbor immense amounts of bacteria and volatile sulfur compounds (VSCs), which are the primary culprits behind halitosis (bad breath).
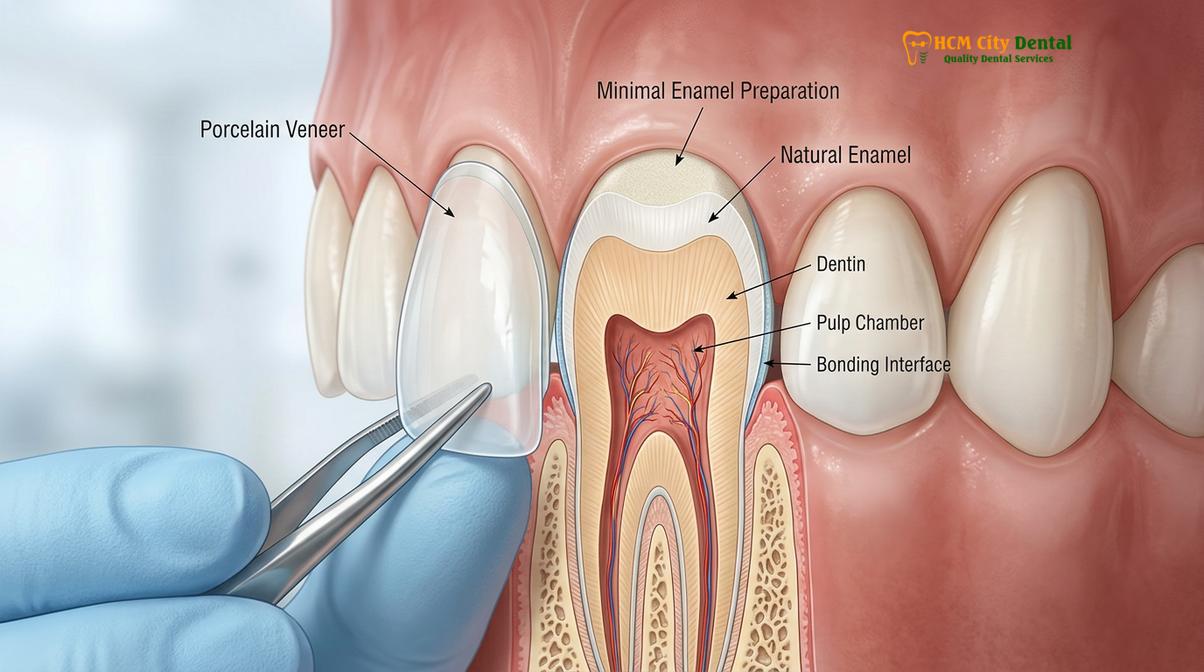
Understanding the structural differences in your teeth, such as the distinction between natural Enamel vs Porcelain: Clinical Differences & Uses | HCMC Dental, can also dictate how gentle you need to be, as aggressive brushing can scratch certain restorative materials over time.
Selecting the Optimal Dental Armamentarium
Choosing the right tools, including a soft-bristled brush and clinically proven fluoride toothpaste, is just as critical as the brushing technique itself for maintaining oral health.
The efficacy of your brushing routine is heavily dependent on the quality and design of the tools you utilize. The dental aisle can be overwhelming, but clinical guidelines simplify the selection process by focusing on evidence-based parameters.
Manual vs. Electric Toothbrushes
A frequent question in clinical practice is whether electric toothbrushes are superior to manual ones. While a patient with excellent manual dexterity can achieve optimal plaque removal with a standard toothbrush using the Modified Bass Technique, clinical studies consistently demonstrate that powered toothbrushes offer superior plaque reduction and gingivitis management for the average user [3].
Electric toothbrushes generally fall into two categories: oscillating-rotating and sonic. Oscillating-rotating brushes feature a small, round head that pulses and rotates back and forth, physically sweeping plaque away. Sonic toothbrushes vibrate at highly elevated frequencies (typically 30,000 to 62,000 brush strokes per minute). This rapid vibration not only scrubs the tooth surface but also creates fluid dynamics—microbubbles that are propelled deep into interproximal spaces and the gingival sulcus, disrupting biofilm beyond where the bristles actually touch.
| Feature | Manual Toothbrush | Electric Toothbrush (Sonic/Oscillating) |
|---|---|---|
| Plaque Removal Efficacy | Highly dependent on user technique and duration. | Clinically proven to remove up to 21% more plaque. |
| Built-in Timers | None; requires manual timing. | Standard 2-minute timers with 30-second quadrant pacers. |
| Pressure Sensors | None; high risk of aggressive brushing. | Often included; alerts user to prevent enamel abrasion. |
| Dexterity Requirements | Requires fine motor skills for proper angulation. | Ideal for patients with limited dexterity or arthritis. |
The Importance of Bristle Stiffness
Regardless of whether you choose manual or electric, the bristles must be categorized as “soft” or “ultra-soft.” Medium and hard bristles are a relic of the past and are strongly contraindicated in modern dentistry. Hard bristles do not clean teeth better; instead, they act like sandpaper against the delicate gingival tissues and the softer root surfaces (dentin and cementum) that may be exposed due to recession. Over time, the use of hard bristles leads to irreversible mechanical wear.

Toothpaste Pharmacology
Toothpaste (dentifrice) is not merely a cosmetic soap for the mouth; it is a topical pharmaceutical delivery system. The most critical active ingredient is fluoride (typically sodium fluoride or stannous fluoride). Fluoride ions integrate into the hydroxyapatite matrix of the enamel, converting it into fluorapatite, which is significantly more resistant to acidic dissolution. For patients with specific clinical needs, dentists may recommend toothpastes containing potassium nitrate for dentin hypersensitivity, or nano-hydroxyapatite for enhanced biomimetic remineralization.
It is also vital to consider the Relative Dentin Abrasivity (RDA) of the toothpaste. Highly abrasive whitening toothpastes can strip away stains but may also abrade the enamel if used continuously with heavy pressure. For personalized recommendations on dental tools and hygiene products, consulting with professionals at the Best Dental Clinic Thao Dien District 2: Expat Guide & Direct Billing ensures you receive advice tailored to your specific oral anatomy.
Common Brushing Errors and Their Clinical Consequences
Aggressive brushing, insufficient duration, and using hard bristles are frequent errors that lead to irreversible enamel wear, dentin hypersensitivity, and gingival recession.
Even patients with the best intentions often inadvertently cause harm to their oral structures through improper brushing habits. Recognizing and correcting these mechanical errors is essential for long-term preservation of the dentition.
Toothbrush Abrasion and Abfraction
The most prevalent clinical error is applying excessive lateral force combined with a horizontal scrubbing motion. This aggressive technique leads to toothbrush abrasion, a form of non-carious cervical lesion (NCCL). Abrasion manifests as V-shaped or U-shaped notches at the cementoenamel junction (CEJ)—the area where the enamel of the crown meets the root. Because the root surface is composed of dentin, which is significantly softer than enamel, it wears away rapidly under mechanical stress [4].
This structural loss exposes the dentinal tubules, microscopic channels that lead directly to the tooth’s nerve pulp. When these tubules are exposed to thermal changes (hot or cold beverages) or tactile stimuli (brushing), the fluid inside the tubules shifts, triggering a sharp, shooting pain known as dentin hypersensitivity. Furthermore, aggressive brushing physically traumatizes the gingival margin, causing the gums to recede and expose even more of the vulnerable root surface.
Inadequate Duration and Missed Zones
Clinical studies indicate that the average person brushes for only 45 to 70 seconds, falling drastically short of the required 120 seconds. This abbreviated duration typically results in “missed zones,” most commonly the lingual (inner) surfaces of the mandibular molars and the distal (back) surfaces of the last molars in the arch. Plaque left undisturbed in these posterior regions rapidly matures into highly pathogenic, anaerobic biofilm, leading to localized periodontal pockets and hidden interproximal cavities.
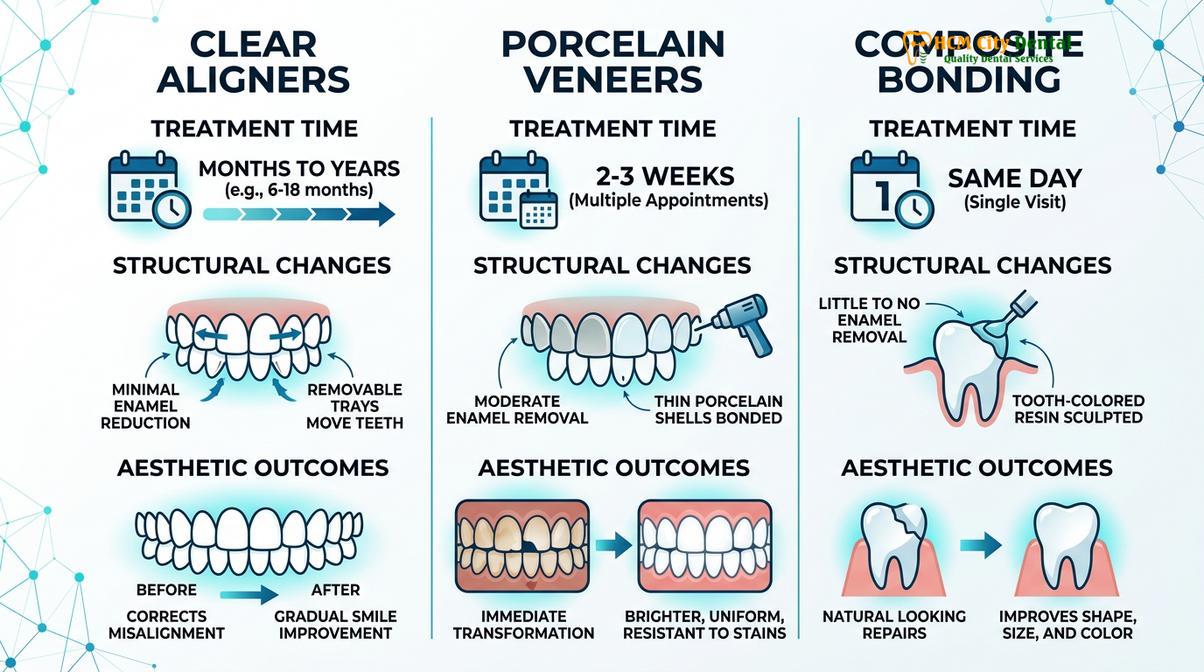
For patients undergoing orthodontic treatments or those exploring How to Fix My Teeth Without Braces | HCMC Dental, meticulous brushing technique becomes even more critical, as clear aligners can trap residual plaque and acid against the teeth if oral hygiene is not perfectly maintained prior to insertion.
Adjunctive Oral Hygiene Measures: Beyond the Toothbrush
Brushing alone cleans only 60% of the tooth surface; interdental cleaning via flossing or water flossers is mandatory to remove biofilm from the remaining 40% between teeth.
A common misconception is that mastering how to brush teeth correctly is sufficient for total oral health. However, the anatomy of a tooth consists of five exposed surfaces: buccal (front), lingual (back), occlusal (top), mesial (side facing the front), and distal (side facing the back). A toothbrush, regardless of its technological sophistication, can only effectively clean the buccal, lingual, and occlusal surfaces. The mesial and distal surfaces—the tight contact points between adjacent teeth—are completely inaccessible to toothbrush bristles.
The Necessity of Interdental Cleaning
The interproximal space houses the interdental papilla (the triangle of gum tissue between teeth) and the “col,” a saddle-like depression of non-keratinized tissue connecting the facial and lingual papillae. The col is highly vulnerable to bacterial invasion and is the most common initiation site for periodontal disease. To disrupt biofilm in this critical zone, interdental cleaning is non-negotiable [5].
Traditional dental floss remains a highly effective tool when used with the correct “C-shape” technique. The floss must be gently guided through the contact point and wrapped around the side of the tooth in a C-shape, then moved up and down to scrape the biofilm off the root surface, extending slightly below the gumline. Snapping the floss straight down and pulling it out does little to clean the tooth and can actually slice the delicate gingival attachment.
“The integration of interdental cleaning is not an optional adjunct but a mandatory requirement; neglecting the interproximal spaces leaves nearly half of the dental anatomy vulnerable to silent, progressive decay and bone loss.”
For patients with wider embrasure spaces, periodontal disease history, or complex restorative work, interdental brushes (small, cylindrical brushes) are often more effective than floss at filling the space and sweeping away plaque. Water flossers (oral irrigators) are another excellent adjunct, utilizing a pulsating stream of water to flush out non-adherent bacteria and food debris from deep periodontal pockets. Patients with anatomical challenges, such as those requiring treatment for Narrow Arch Teeth: Clinical Diagnosis & Expansion | HCMC Dental, often find water flossers indispensable for navigating crowded or overlapping dentition.
Real-World Clinical Application and Patient Education
Personalized oral hygiene instruction based on individual anatomical variations ensures that patients can effectively manage their plaque control at home.
Theoretical knowledge of brushing mechanics must be translated into daily, sustainable habits. In clinical practice, dental professionals do not merely hand out toothbrushes; they perform tailored plaque control records and provide hands-on hygiene instruction. At HCMC Dental Clinic in Ho Chi Minh City, preventive care is heavily emphasized, ensuring that every patient understands the specific nuances of their own oral anatomy.
A 34-year-old patient presented to Dr. Nguyen Van Cuong at HCMC Dental Clinic in Ho Chi Minh City with severe dentin hypersensitivity and localized gingival recession on the maxillary canines. The clinical examination revealed classic signs of toothbrush abrasion caused by a hard-bristled brush and a horizontal scrubbing technique. Dr. Cuong transitioned the patient to an ultra-soft sonic toothbrush and provided hands-on instruction in the Modified Bass Technique. Within four weeks, the gingival inflammation subsided, and the hypersensitivity was successfully managed with a prescription fluoride varnish, highlighting the critical importance of proper mechanical technique.
Dr. Cuong frequently notes that patient compliance increases significantly when they understand the “why” behind the technique. Visual aids, such as disclosing tablets that dye invisible plaque a bright pink or purple color, are excellent educational tools. By chewing a disclosing tablet after brushing, patients can immediately see the areas they have missed, providing real-time biofeedback to correct their angulation and duration.

For expatriates and locals alike seeking high-quality preventive education, visiting the Best Dental Clinic District 1 Saigon: Clinical Comparison & Expat Guide can connect you with professionals who prioritize comprehensive hygiene instruction over reactive treatments.
When to See a Doctor for Periodontal Evaluation
While mastering how to brush teeth correctly is your primary defense against oral disease, home care has its limitations. It is imperative to recognize the clinical signs that indicate your home hygiene routine is failing or that professional intervention is required. You should schedule a comprehensive periodontal evaluation if you experience any of the following symptoms:
- Persistent Gingival Bleeding: Healthy gums do not bleed. If your gums bleed consistently during brushing or flossing for more than two weeks, it is a definitive sign of active gingival inflammation or periodontitis.
- Chronic Halitosis: Persistent bad breath or a metallic taste in the mouth, despite thorough brushing and tongue scraping, often indicates deep subgingival bacterial reservoirs that require professional scaling.
- Visible Calculus Accumulation: If you notice hard, yellow, brown, or black deposits along the gumline or on the back of your lower front teeth, this is calculus. It cannot be brushed away and must be removed by a hygienist or dentist.
- Gingival Recession or Tooth Mobility: Gums that appear to be pulling away from the teeth, making the teeth look longer, or any sensation of teeth feeling loose, are severe warning signs of advanced bone loss.
- Sudden Hypersensitivity: A sharp, sudden increase in sensitivity to hot, cold, or sweet stimuli may indicate that aggressive brushing has exposed dentin, or that a carious lesion has breached the enamel.
Regular professional prophylaxis (cleanings) every six months is the standard clinical recommendation. However, patients with a history of periodontal disease, systemic conditions like diabetes, or heavy calculus formers may require maintenance visits every three to four months. If you experience acute pain, swelling, or trauma related to your oral hygiene routine, consult the Common Dental Emergencies: Clinical Guide | HCMC Dental and seek immediate professional care.
Frequently Asked Questions
Should I brush my teeth before or after breakfast?
It is clinically recommended to brush before breakfast. Brushing beforehand removes morning plaque and coats your teeth with protective fluoride, whereas brushing immediately after eating acidic foods can damage softened enamel. If you prefer brushing after, wait at least 30 minutes to allow saliva to neutralize oral acids.
Is it better to use an electric or a manual toothbrush?
Both are effective if used correctly, but electric toothbrushes generally remove more plaque. Oscillating-rotating or sonic models provide automated sweeping motions that compensate for poor manual brushing techniques. They are particularly beneficial for patients with limited dexterity, orthodontic appliances, or a history of aggressive brushing.
How often should I replace my toothbrush?
You should replace your toothbrush or electric brush head every three to four months. If the bristles become visibly frayed, splayed, or if you have recently recovered from an illness, replace it sooner. Worn bristles lose their structural integrity, drastically reducing their ability to sweep plaque from the gingival sulcus.
Why do my gums bleed when I brush my teeth?
Bleeding gums are a primary clinical sign of gingival inflammation (gingivitis) caused by inadequate plaque removal. Consistent, gentle brushing and daily interdental cleaning will typically resolve mild gingivitis within two weeks. If bleeding persists beyond this timeframe, professional periodontal evaluation is required to rule out advanced disease.
Can I brush my teeth too much or too hard?
Yes, aggressive brushing or brushing more than three times a day can cause toothbrush abrasion. This leads to irreversible enamel wear, receding gums, and heightened dentin hypersensitivity. Always use a soft-bristled brush, apply light pressure, and rely on the mechanical sweeping motion rather than forceful scrubbing.
References
- Journal of Clinical Periodontology. The efficacy of the Modified Bass technique in plaque removal and gingivitis reduction. (2021).
- American Dental Association (ADA). Oral health topics: Toothbrushes and brushing techniques. (2022).
- Cochrane Database of Systematic Reviews. Manual versus powered toothbrushes for oral health. (2019).
- Journal of Dentistry. The role of toothpaste abrasivity (RDA) in non-carious cervical lesions. (2020).
- International Journal of Dental Hygiene. Interdental cleaning methods and their impact on periodontal health. (2023).