Common dental emergencies encompass acute conditions requiring immediate clinical intervention to alleviate severe pain, halt active bleeding, or resolve spreading infections. Prompt diagnostic evaluation and targeted treatment are critical to preserving dentition and preventing life-threatening systemic complications.
Clinical Summary:
According to Dr. Nguyen Van Cuong, dental emergencies are broadly classified into traumatic injuries, acute odontogenic infections, and post-procedural complications. Immediate stabilization of the affected tissues, appropriate pharmacological management, and definitive restorative or surgical interventions form the cornerstone of emergency dental care. Rapid triage and accurate diagnosis are essential to differentiate between localized dental issues and potentially life-threatening systemic infections, ensuring optimal patient outcomes and the preservation of oral health.
Key Takeaways:
- Avulsed permanent teeth have the highest survival and reattachment rate if replanted within 30 to 60 minutes of the injury.
- Acute dental infections can rapidly progress to facial cellulitis, potentially threatening the patient’s airway if left untreated.
- Severe, unprovoked throbbing pain is a hallmark clinical sign of irreversible pulpitis, typically requiring prompt endodontic therapy.
- Post-extraction bleeding that persists beyond 12 hours necessitates immediate clinical hemostatic intervention and evaluation.
- Lost restorations or crowns should be evaluated promptly to prevent pulpal exposure, bacterial contamination, and structural collapse.
Classification of Common Dental Emergencies
Dental emergencies are broadly categorized into traumatic, infectious, and post-procedural etiologies, each requiring distinct diagnostic protocols and targeted therapeutic interventions to stabilize the patient.
The management of acute oral conditions requires a systematic approach to triage, diagnosis, and treatment. In the context of general dental care, emergencies present a unique challenge as they often involve severe pain, high patient anxiety, and the potential for rapid clinical deterioration. Healthcare providers must be adept at recognizing the underlying etiology of the emergency to implement the most effective treatment workflow. The spectrum of emergencies in dental practice ranges from minor restorative failures to severe maxillofacial trauma and life-threatening fascial space infections.
Understanding the primary categories of dental emergencies helps clinicians streamline their diagnostic process. Traumatic injuries involve direct physical impact to the dentition and surrounding periodontium. Infectious emergencies arise from the proliferation of oral pathogens, typically secondary to untreated dental caries or periodontal disease. Post-procedural complications occur as adverse events following dental treatments, such as extractions or restorative work. Regardless of the category, the primary objectives in any primary health care dental setting are to secure the airway, achieve hemostasis, manage acute pain, and eliminate active infection[1].

Traumatic Dental Injuries: Avulsions, Luxations, and Fractures
Traumatic injuries to the dentition demand rapid clinical assessment to preserve tooth vitality, stabilize the surrounding alveolar bone, and restore the structural integrity of the smile.
Traumatic dental injuries frequently result from sports-related accidents, falls, or physical altercations. The anterior maxilla is the most commonly affected region due to its prominent position in the facial structure. When a patient presents with dental trauma, a comprehensive evaluation is mandatory to rule out concurrent head injuries, cervical spine trauma, or maxillofacial fractures before focusing on the localized dental injury. Providing gentle dental care during these high-stress situations is crucial for patient cooperation and optimal clinical outcomes.
Tooth Avulsion (Knocked-Out Tooth) Workflow
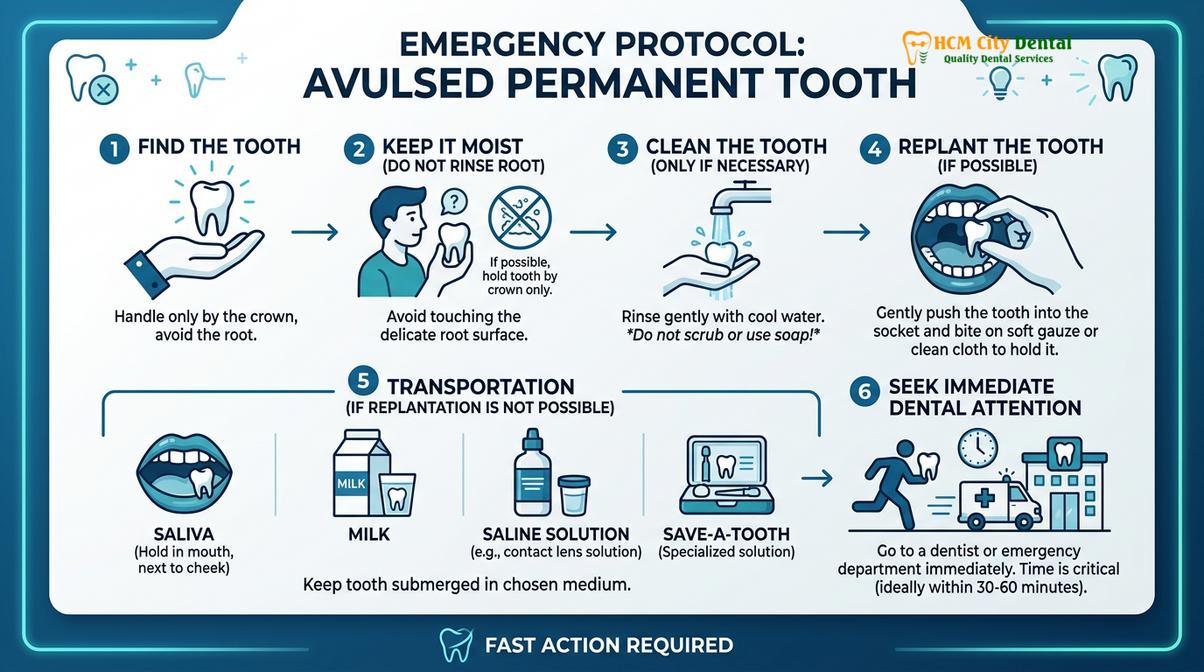
Tooth avulsion, the complete displacement of a tooth from its alveolar socket, is one of the most time-sensitive common dental emergencies. The prognosis of an avulsed permanent tooth depends heavily on the viability of the periodontal ligament (PDL) cells remaining on the root surface. Immediate replantation at the site of injury is the treatment of choice. If immediate replantation is not feasible, the tooth must be stored in a physiological medium to prevent PDL cell necrosis. Hank’s Balanced Salt Solution (HBSS), cold milk, or the patient’s saliva are acceptable storage media; water should be avoided as its hypotonicity causes rapid cell lysis[1].
Clinical Warning: Never handle an avulsed tooth by its root. Always hold the tooth by the clinical crown to avoid crushing the delicate periodontal ligament cells, and do not scrub the root surface, as this will drastically reduce the chances of successful replantation and increase the risk of replacement resorption (ankylosis).
Upon arrival at the clinic, the practitioner will gently irrigate the socket with saline, replant the tooth, and apply a flexible splint for approximately two weeks to allow for initial PDL healing. Endodontic therapy (root canal treatment) is typically initiated within 7 to 10 days post-replantation for teeth with closed apices to prevent infection-related inflammatory resorption.
Crown Fractures and Luxations
Dental fractures are classified based on the extent of tissue involvement. Uncomplicated crown fractures involve only the enamel or enamel and dentin, presenting primarily with thermal sensitivity. These can often be managed conservatively with bonded composite restorations. Complicated crown fractures involve pulpal exposure, necessitating direct pulp capping, partial pulpotomy, or complete root canal therapy, depending on the size of the exposure and the time elapsed since the injury. Proper dental mirror use is essential during the examination to identify subtle fracture lines and assess the extent of the damage.
Luxation injuries involve the displacement of the tooth within the socket without complete avulsion. These include concussions, subluxations, extrusions, lateral luxations, and intrusions. Management typically involves repositioning the displaced tooth under local anesthesia, followed by flexible splinting and rigorous clinical and radiographic follow-up to monitor pulpal vitality[5].
Infectious Dental Emergencies: Abscesses and Severe Pulpitis
Odontogenic infections typically originate from untreated caries or necrotic pulp tissue, presenting with severe localized pain, swelling, and the potential for dangerous systemic involvement.
Infectious dental emergencies are among the most frequent reasons patients seek urgent care at a dental care clinic. The oral cavity harbors a complex polymicrobial microbiome. When the physical barriers of the tooth (enamel and dentin) are breached by decay or trauma, bacteria invade the sterile pulp chamber, initiating a profound inflammatory response. If left untreated, this localized inflammation can progress to pulpal necrosis and spread into the periapical tissues, leading to abscess formation.
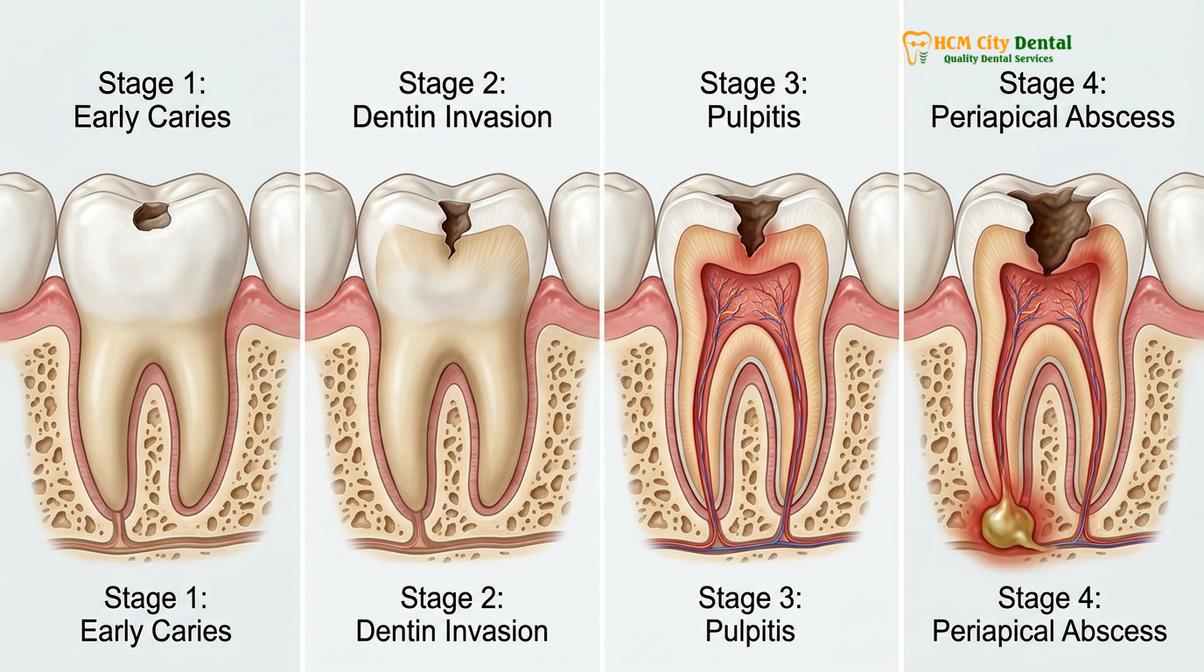
Irreversible Pulpitis Management
Irreversible pulpitis is characterized by severe, spontaneous, and lingering pain that is often exacerbated by thermal stimuli, particularly cold or heat. The pain may radiate to the ear, temple, or jaw, making it difficult for the patient to localize the offending tooth. At this stage, the pulpal tissue is inflamed beyond the point of recovery. The definitive treatment for irreversible pulpitis is the complete removal of the inflamed tissue via endodontic therapy (root canal treatment) or, if the tooth is unrestorable, extraction[2].
Patients seeking relief at a smile care dental clinic will often require profound local anesthesia, which can be challenging to achieve in the presence of acute inflammation due to the altered tissue pH. Techniques such as intraligamentary or intraosseous injections may be necessary to ensure patient comfort during the emergency extirpation of the pulp.
Acute Apical Abscess and Cellulitis Risk
An acute apical abscess occurs when the infection spreads beyond the root apex into the surrounding alveolar bone, resulting in localized purulent exudate (pus) accumulation. Clinical signs include severe pain on biting or percussion, tooth mobility, and localized mucosal swelling. Treatment involves establishing drainage, either through the tooth (by opening the pulp chamber) or via surgical incision and drainage of the soft tissue swelling.
“The rapid progression of an odontogenic infection from a localized abscess to diffuse facial cellulitis represents a critical medical emergency. Immediate intervention to establish drainage and remove the source of infection is paramount to prevent airway compromise.” — Dr. Nguyen Van Cuong
If the infection breaches the cortical bone and spreads into the fascial spaces of the head and neck, it can cause cellulitis—a diffuse, rapidly spreading inflammation of the soft tissues. This is a serious condition that may require aggressive antibiotic therapy, hospitalization, and intravenous medications, particularly if the swelling threatens the airway (e.g., Ludwig’s angina)[4]. For patients exploring options for General Dentistry, understanding the importance of early intervention for dental decay is crucial to preventing these severe infectious complications.
Prosthodontic and Post-Procedural Complications
Complications following restorative or surgical procedures, such as lost crowns, broken prostheses, or alveolar osteitis, require prompt palliative and corrective care to restore function.
Even with meticulous clinical technique, post-procedural complications can arise, prompting patients to seek emergency care. These situations require a calm, systematic approach to diagnose the failure and implement a corrective strategy. A well-equipped hub dental practice must be prepared to handle everything from minor restorative debonding to severe post-surgical bleeding.
Lost Crowns, Fillings, and Broken Dentures
The dislodgement of a dental restoration, such as a filling, crown, or bridge, exposes the underlying prepared dentin to the oral environment. This can cause significant thermal and tactile sensitivity. Furthermore, prolonged loss of a restoration can lead to the drifting of adjacent teeth, altering the occlusion and complicating the eventual replacement of the prosthesis. Emergency management involves cleaning the preparation, assessing the tooth for secondary caries, and recementing the restoration or placing a temporary filling material (such as Glass Ionomer Cement) to protect the tooth.
For older adults, particularly those utilizing dental plans for seniors, broken removable prosthetics (dentures or partials) constitute a significant functional emergency, impairing their ability to eat and speak. Repairing these prostheses quickly and accurately is essential for maintaining the patient’s quality of life and nutritional intake. Patients often inquire about replacing extracted teeth with implants, bridges, or partials after experiencing repeated failures with older, ill-fitting removable appliances.

Alveolar Osteitis (Dry Socket) and Post-Extraction Bleeding
Alveolar osteitis, commonly known as “dry socket,” is a painful complication that occurs when the blood clot at an extraction site fails to form or is prematurely dislodged, exposing the underlying alveolar bone. It typically presents 3 to 5 days post-extraction with severe, radiating pain and a foul odor or taste. Management is palliative, involving gentle irrigation of the socket with chlorhexidine or saline and the placement of a medicated dressing (e.g., Alvogyl) to soothe the exposed nerve endings[3].
| Clinical Feature | Normal Extraction Healing | Alveolar Osteitis (Dry Socket) |
|---|---|---|
| Pain Profile | Mild to moderate, decreasing daily | Severe, radiating, worsening after 3-5 days |
| Socket Appearance | Filled with a dark red/brown organized clot | Empty socket, exposed grayish bone visible |
| Odor/Taste | Normal oral environment | Distinct halitosis and foul taste present |
| Surrounding Tissue | Mild inflammation, resolving normally | Highly inflamed, tender gingival margins |
Post-extraction bleeding is another common post-procedural emergency. While slight oozing is normal for the first 24 hours, active, pulsatile bleeding or the formation of large “liver clot” hematomas requires intervention. The clinician will typically administer local anesthesia with a vasoconstrictor, remove the poorly formed clot, and apply hemostatic agents (such as oxidized regenerated cellulose or gelatin sponges) followed by figure-of-eight suturing to achieve primary closure and hemostasis.
Diagnostic Protocols in the Emergency Dental Setting
Accurate diagnosis of acute dental conditions relies on a combination of thorough clinical examination, detailed patient history, and targeted radiographic imaging to identify the source of pathology.
When a patient presents with a dental emergency, the diagnostic process must be efficient yet comprehensive. The clinician begins by gathering a detailed history of the chief complaint, focusing on the onset, duration, intensity, and nature of the pain. Understanding what exacerbates or relieves the symptoms provides critical clues. For instance, pain that wakes a patient from sleep is highly indicative of irreversible pulpitis.
Clinical Evaluation and Radiographic Imaging
The clinical examination involves a visual inspection of the oral cavity, looking for signs of swelling, erythema, sinus tracts (fistulas), or gross decay. A dental clinic smile care team will utilize specific diagnostic tests to pinpoint the offending tooth. Percussion testing (tapping the tooth) assesses the status of the periapical tissues, while palpation of the overlying gingiva checks for localized abscesses. Vitality testing, using cold sprays (Endo-Ice) or an electric pulp tester (EPT), evaluates the health of the pulpal nerve fibers.
Radiographic imaging is indispensable in emergency dentistry. Periapical radiographs provide a detailed view of the entire tooth and surrounding bone, revealing periapical radiolucencies (infections), root fractures, or deep caries. In cases of maxillofacial trauma or complex infections, a Cone Beam Computed Tomography (CBCT) scan may be necessary to provide a three-dimensional view of the anatomical structures, allowing for precise surgical planning and risk assessment. Patients seeking a gentle dental approach appreciate when clinicians explain these diagnostic steps clearly, reducing anxiety associated with the unknown.
Clinical Case Study: Managing Acute Trauma
A 24-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City following a bicycle accident, exhibiting a complicated crown-root fracture of the maxillary right central incisor. The patient was experiencing severe pain due to pulpal exposure. Dr. Nguyen Van Cuong performed an immediate clinical and radiographic assessment. Due to the subgingival extent of the fracture, the tooth was deemed unrestorable. The emergency protocol involved atraumatic extraction, immediate placement of a dental implant, and the fabrication of a provisional crown to restore aesthetics and function on the same day, demonstrating the efficacy of advanced emergency prosthodontic workflows.
When to Seek Immediate Medical or Dental Attention
While many dental issues can wait for a scheduled appointment, certain symptoms indicate a severe, potentially life-threatening condition that requires immediate intervention. It is crucial for patients to understand the difference between a standard toothache and a medical emergency. If you experience any of the following red flag symptoms, you should seek immediate care at an emergency room or an advanced dental facility equipped to handle severe maxillofacial infections.
Rapidly spreading facial swelling, particularly swelling that extends beneath the lower jaw or down the neck, is a critical warning sign. This can indicate Ludwig’s angina, a rapidly progressive cellulitis that can compromise the airway. Difficulty swallowing (dysphagia), difficulty breathing (dyspnea), or a severe inability to open the mouth (trismus) are also signs that an infection has spread into the deep fascial spaces of the head and neck. Furthermore, a high fever accompanied by chills and lethargy suggests systemic involvement of the infection.
“Patients must never ignore swelling that affects their breathing or swallowing. In such instances, bypassing the dental office and heading straight to a hospital emergency department is the safest and most appropriate course of action.” — Clinical Consensus
For non-life-threatening but highly painful conditions, finding a gentle dental near me or a primary dental care provider who offers emergency appointments is the best approach. Clinics that prioritize gentle smile dental techniques can manage acute pain effectively while planning definitive treatment. For those exploring dental career services, understanding emergency triage is a fundamental skill taught in advanced dental assisting and hygiene programs. Whether you visit a specialized smile o care dental clinic or a general practice like gentle dental az, prompt evaluation is key to preventing further complications.
If you are experiencing severe dental pain, trauma, or swelling, do not delay treatment. Contact HCMC Dental Clinic in Ho Chi Minh City immediately for a comprehensive emergency evaluation. Our team is equipped to provide rapid diagnostics, pain relief, and definitive care to protect your oral health. You can also explore our guide on the Best Dental Clinic District 1 Saigon for more information on accessing top-tier emergency services in the city.

Frequently Asked Questions
What should I do if my tooth is completely knocked out?
Pick up the tooth by the crown, rinse it gently without scrubbing the root, and attempt to reinsert it into the socket. If replantation is not possible, store the tooth in milk or Hank’s Balanced Salt Solution and seek immediate emergency dental care. Time is the most critical factor; replanting the tooth within 30 to 60 minutes significantly increases the chances of saving it and preserving the periodontal ligament.
How can I temporarily manage severe toothache pain at home?
Take over-the-counter anti-inflammatory medications such as ibuprofen, apply a cold compress to the outside of your cheek to reduce swelling, and avoid hot, cold, or sweet stimuli until you can be evaluated by a dentist. Do not place aspirin directly on the gums, as this can cause a severe chemical burn. Rinse your mouth with warm salt water to help keep the area clean and reduce localized inflammation.
Is a lost filling or dental crown considered a true emergency?
While not typically life-threatening, a lost filling or crown is an urgent dental issue that requires prompt attention to prevent bacterial contamination of the exposed dentin, severe thermal sensitivity, and potential damage to the remaining tooth structure. If left untreated for an extended period, the adjacent teeth may shift, or the exposed tooth may decay further, potentially necessitating a root canal or extraction instead of a simple recementation.
What are the signs that a dental infection is spreading dangerously?
Red flag symptoms include rapid facial swelling, difficulty swallowing (dysphagia), difficulty breathing (dyspnea), restricted jaw opening (trismus), and a high fever. These indicate a spreading fascial space infection requiring immediate medical intervention. If you experience any of these symptoms, you should proceed to the nearest hospital emergency department immediately, as the infection could compromise your airway.
Can I go to a hospital emergency room for a severe toothache?
Hospital emergency rooms can provide antibiotics and strong analgesics for pain and swelling, but they rarely have dentists on staff to perform definitive treatments like root canals or extractions. You will still need to follow up with a dental professional. Therefore, unless you are experiencing life-threatening symptoms like airway compromise or severe facial trauma, it is generally more effective to seek care directly from an emergency dental clinic.
References
- Journal of Endodontics. Management of traumatic dental injuries and avulsions. (2020).
- American Association of Endodontists. Diagnostic protocols for irreversible pulpitis and acute apical abscesses. (2021).
- International Journal of Oral and Maxillofacial Surgery. Pathophysiology and clinical management of alveolar osteitis. (2019).
- Journal of the American Dental Association. Antibiotic stewardship in the management of odontogenic infections. (2022).
- Dental Traumatology. Splinting protocols and periodontal ligament healing following luxation injuries. (2018).