Root canal treatment is a highly effective clinical procedure designed to eliminate infection from the innermost layer of a tooth, known as the dental pulp. By carefully removing inflamed tissue, disinfecting the root canal system, and sealing the space, this therapy preserves the natural tooth structure and restores optimal oral function.
Clinical Summary:
Endodontic therapy, commonly referred to as a root canal, is a vital dental intervention utilized to salvage teeth compromised by deep decay, trauma, or severe pulpitis. The procedure involves the meticulous mechanical debridement and chemical disinfection of the internal root canal system, followed by a hermetic three-dimensional obturation to prevent bacterial reinfection. Modern advancements in endodontic technology, including rotary instrumentation, 3D cone-beam computed tomography (CBCT), and surgical operating microscopes, have dramatically elevated the precision, comfort, and long-term success rates of this treatment. Preserving the natural dentition through root canal therapy is generally preferred over extraction, as it maintains alveolar bone integrity, ensures proper masticatory function, and supports overall maxillofacial harmony.
Key Takeaways:
- Root canal therapy removes infected or necrotic pulp tissue to save the natural tooth structure.
- The procedure relies on profound local anesthesia, making it a comfortable and virtually painless experience.
- Advanced technologies like CBCT imaging and operating microscopes ensure precise cleaning of complex root anatomies.
- Following treatment, a definitive coronal restoration, typically a crown, is essential to prevent tooth fracture.
- Timely intervention prevents the spread of infection to the periapical bone and surrounding systemic tissues.
Understanding the Pathophysiology of Root Canal Infections
The dental pulp contains vital nerves and blood vessels that can become irreversibly inflamed due to bacterial invasion, requiring immediate endodontic intervention to prevent systemic spread and localized bone destruction.
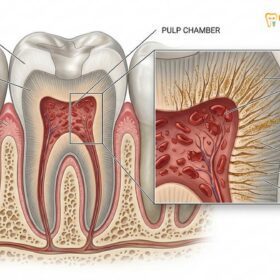
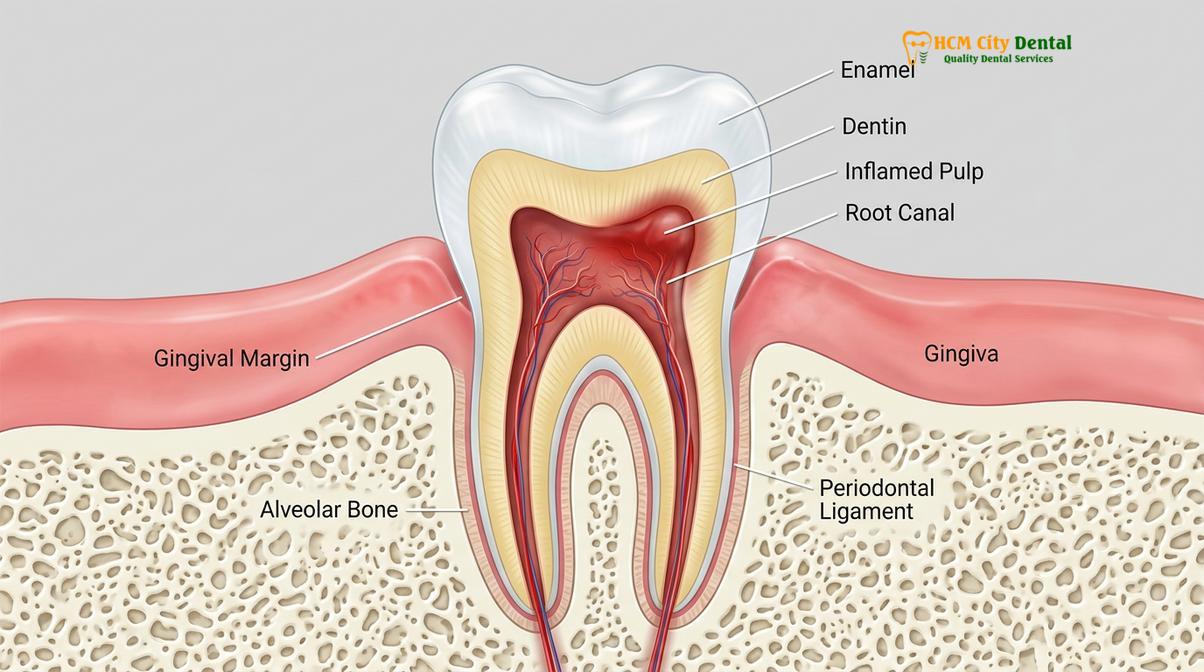
To fully comprehend the necessity of root canal treatment, one must first understand the complex microanatomy of the human tooth. A tooth is not a solid block of calcified tissue; rather, it is a highly structured organ composed of several distinct layers. The outermost layer, the enamel, is the hardest substance in the human body and serves as the primary defense against mechanical wear and bacterial acid attacks. Beneath the enamel lies the dentin, a porous, yellowish tissue containing thousands of microscopic tubules that communicate directly with the innermost core of the tooth.
This central core is known as the pulp chamber, which extends down through the roots via narrow pathways called root canals. The dental pulp is a specialized connective tissue rich in blood vessels, lymphatic vessels, and nerve fibers. During the developmental stages of a tooth, the pulp is responsible for forming the surrounding dentin. Once the tooth is fully mature, the pulp’s primary functions shift to sensory perception (detecting temperature and pressure) and providing hydration and nutrients to the dentin.
When the protective layers of enamel and dentin are compromised—most commonly through extensive dental caries (cavities), repeated invasive dental procedures, or traumatic injuries—the sterile environment of the pulp chamber is breached. Oral bacteria, which naturally inhabit the mouth in the form of plaque and biofilm, rapidly colonize the exposed pulp tissue. This bacterial invasion triggers an intense inflammatory response known as pulpitis. Because the pulp is encased within rigid dentinal walls, the inflammatory swelling leads to a dramatic increase in intrapulpal pressure. This pressure compresses the delicate blood vessels, eventually strangulating the blood supply and leading to ischemic necrosis (death) of the pulp tissue.[1]
Once the pulp tissue becomes necrotic, it serves as a fertile breeding ground for anaerobic bacteria. These microorganisms metabolize the necrotic tissue and produce toxic byproducts that seep out through the apical foramen (the opening at the tip of the root) into the surrounding periapical tissues. This process initiates a periapical inflammatory response, leading to the destruction of the alveolar bone and the formation of a periapical abscess or granuloma. Without professional endodontic therapy services, the infection will continue to spread, potentially causing severe localized pain, facial swelling, and in rare cases, life-threatening systemic infections.
The Microbiology of Endodontic Disease
Root canal infections are polymicrobial in nature, driven by complex bacterial biofilms that adhere tightly to the dentinal walls, necessitating rigorous chemical and mechanical disinfection protocols.
The success of root canal treatment hinges on the clinician’s ability to effectively eradicate the microbial load within the root canal system. The microbiology of primary endodontic infections is highly complex and predominantly involves a diverse consortium of anaerobic bacteria. These microorganisms do not exist as free-floating (planktonic) entities; rather, they organize themselves into highly structured, resilient communities known as biofilms. Biofilms adhere tenaciously to the walls of the root canal and can even penetrate deep into the dentinal tubules, making them exceptionally difficult to eliminate using mechanical instrumentation alone.[2]
Common bacterial species isolated from infected root canals include Enterococcus faecalis, Porphyromonas gingivalis, Prevotella species, and Fusobacterium nucleatum. These bacteria exhibit synergistic relationships, sharing nutrients and genetic material to enhance their collective survival and virulence. Furthermore, the biofilm matrix provides a protective barrier that shields the bacteria from the host’s immune system and systemic antibiotics. This is why prescribing oral antibiotics alone is fundamentally ineffective at curing a root canal infection; the source of the infection—the necrotic tissue and biofilm within the avascular canal space—must be physically removed.
To combat these resilient biofilms, modern endodontic therapy employs a dual approach of mechanical debridement and chemical irrigation. Mechanical instrumentation physically disrupts the biofilm and removes the bulk of the infected tissue, while chemical irrigants, such as sodium hypochlorite (NaOCl) and ethylenediaminetetraacetic acid (EDTA), dissolve organic debris, flush out bacteria, and remove the smear layer created during instrumentation. The synergistic use of these techniques is paramount to achieving a biologically acceptable level of disinfection, allowing the periapical tissues to heal.
Clinical Indicators and Diagnostic Criteria
Accurate diagnosis relies on identifying specific clinical symptoms, such as spontaneous pain or prolonged thermal sensitivity, combined with advanced radiographic imaging to assess periapical health.
Identifying the need for root canal treatment requires a comprehensive clinical and radiographic evaluation. Patients often present with a variety of subjective symptoms that indicate varying stages of pulpal and periapical disease. One of the most classic signs of irreversible pulpitis is spontaneous, unprovoked pain. This pain is often described as a deep, throbbing ache that may radiate to the jaw, ear, or temple, making it difficult for the patient to pinpoint the exact offending tooth. The pain frequently exacerbates at night or when lying down, due to increased blood flow and pressure in the head.
Another hallmark symptom is prolonged sensitivity to thermal stimuli, particularly cold or hot liquids. While transient sensitivity (lasting only a few seconds) may indicate reversible pulpitis or exposed dentin, pain that lingers for several minutes after the stimulus is removed is a strong indicator that the pulp is irreversibly damaged and requires intervention. Additionally, patients may experience severe pain upon mastication (chewing) or when pressure is applied to the tooth, which suggests that the inflammation has extended beyond the root apex into the periodontal ligament (acute apical periodontitis).
In cases where the pulp has become completely necrotic and a chronic periapical abscess has formed, the patient may not experience acute pain. Instead, they might notice a localized swelling on the gums adjacent to the affected tooth. This swelling, often resembling a small pimple, is known as a sinus tract or fistula. It serves as a drainage pathway for the purulent exudate (pus) accumulating in the bone. Addressing this specific presentation requires comprehensive dental fistula treatment alongside the primary endodontic therapy to ensure the complete resolution of the infectious pathway.
Clinical Warning: Ignoring the symptoms of an infected tooth can lead to severe complications. An untreated dental abscess can spread rapidly into the fascial spaces of the head and neck, resulting in conditions such as cellulitis or Ludwig’s angina, which can compromise the airway and require emergency hospitalization. Never rely solely on pain medication to manage a dental infection.
The Comprehensive Root Canal Procedure: A Clinical Workflow
Modern endodontic therapy follows a strict, multi-step protocol involving profound anesthesia, precise isolation, mechanical debridement, chemical disinfection, and hermetic obturation of the canal system.
The clinical execution of a root canal treatment is a meticulous process that demands a high level of technical skill and an intimate understanding of root canal anatomy. The procedure is typically completed in one or two visits, depending on the complexity of the tooth, the presence of active infection, and the clinician’s assessment. For patients undergoing endodontic care in Vietnam, understanding this step-by-step workflow can significantly alleviate dental anxiety and set appropriate clinical expectations.
Step 1: Diagnostic Imaging and Profound Anesthesia
The procedure begins with a thorough review of the patient’s medical history and the acquisition of high-resolution digital radiographs. In complex cases, a 3D Cone-Beam Computed Tomography (CBCT) scan may be utilized to visualize the exact number, curvature, and location of the root canals. Once the diagnosis is confirmed, the clinician administers profound local anesthesia. Modern anesthetic agents, such as Articaine or Lidocaine with epinephrine, ensure that the tooth and surrounding tissues are completely numb, rendering the procedure virtually painless.
Step 2: Isolation and Access Preparation
To maintain a sterile operating field and protect the patient’s airway from small instruments and chemical irrigants, a rubber dam is placed over the target tooth. This thin sheet of latex or non-latex material isolates the tooth from the oral cavity’s saliva and bacteria. Using a high-speed dental handpiece, the clinician then creates a precise access cavity through the biting surface of the tooth (or the back surface for anterior teeth) to expose the pulp chamber.

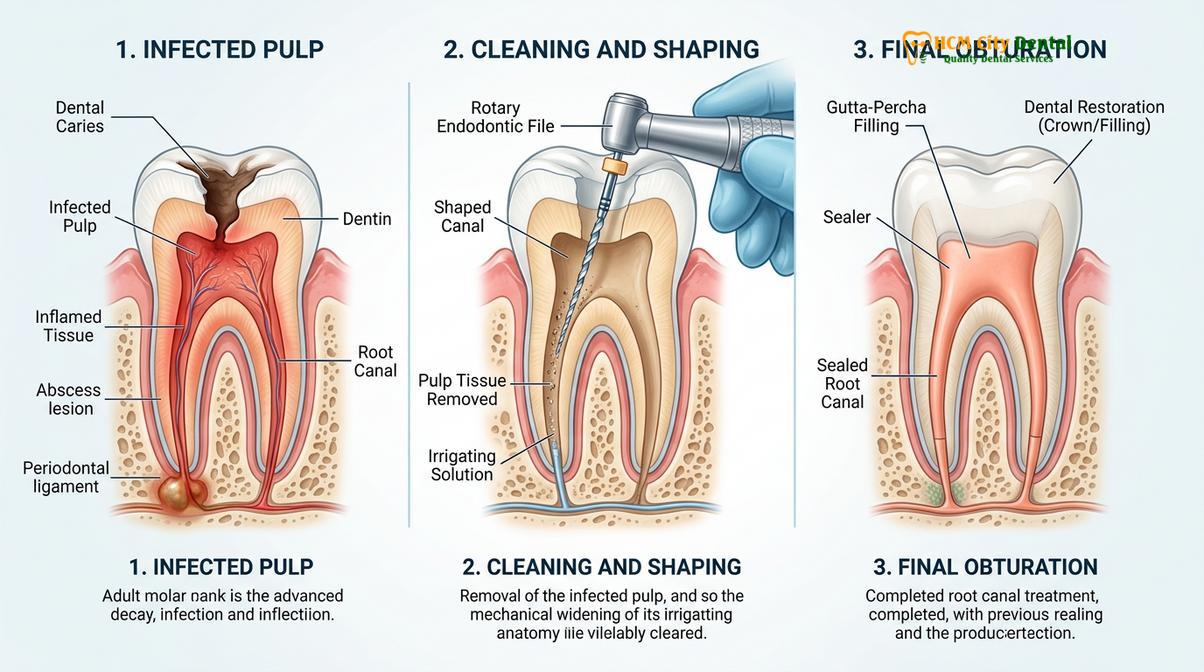
Step 3: Cleaning and Shaping (Biomechanical Preparation)
Once the pulp chamber is accessed, specialized endodontic instruments called files are used to navigate the root canals. Historically, this was done entirely with stainless steel hand files. Today, clinicians utilize engine-driven nickel-titanium (NiTi) rotary files, which are highly flexible and conform to the natural curvature of the canals. These files systematically remove the infected pulp tissue, shape the canal walls to a continuous taper, and create sufficient space for the disinfecting solutions. Copious irrigation with sodium hypochlorite is performed continuously to chemically dissolve organic debris and eradicate bacterial biofilms.[3]
Step 4: Three-Dimensional Obturation
After the canal system has been thoroughly cleaned, shaped, and dried with sterile paper points, it must be sealed to prevent future bacterial microleakage. This process is known as obturation. The most common obturation material is gutta-percha, a biocompatible, rubber-like material derived from the sap of certain trees. The gutta-percha cones are coated with an endodontic sealer and precisely placed into the canals. Heat is often applied to soften the gutta-percha, allowing it to flow and adapt intimately to the complex internal anatomy, creating a hermetic seal from the apex to the coronal orifice.
Step 5: Coronal Restoration
The final, and arguably most critical, step for long-term success is the placement of a definitive coronal restoration. The access cavity is initially sealed with a core build-up material, often a composite resin. Because endodontically treated teeth are structurally weakened and more prone to fracture, a full-coverage dental crown is highly recommended, especially for posterior teeth (premolars and molars) that bear heavy masticatory forces. For a deeper understanding of the entire process, patients can review a detailed endodontic workflow to familiarize themselves with each clinical phase.
Materials Used in Modern Endodontic Obturation
The evolution of endodontic materials, particularly the shift toward biocompatible bioceramic sealers, has significantly improved the sealing ability and tissue healing response following root canal therapy.
The ultimate goal of obturation is to create a fluid-tight seal along the entire length of the root canal system, entombing any remaining microscopic bacteria and preventing the ingress of tissue fluids that could provide nutrients for microbial growth. While gutta-percha has remained the gold standard core obturation material for over a century due to its biocompatibility, radiopacity, and ease of removal if retreatment is necessary, the sealers used in conjunction with it have undergone significant technological advancements.
Historically, zinc oxide-eugenol (ZOE) or resin-based sealers were predominantly used. While effective, these materials can exhibit slight shrinkage upon setting and may provoke a mild inflammatory response if extruded beyond the root apex. In recent years, the paradigm has shifted toward the use of bioceramic (calcium silicate-based) sealers. These advanced materials are highly biocompatible, hydrophilic (utilizing the natural moisture in the dentinal tubules to initiate the setting reaction), and exhibit zero shrinkage. Furthermore, bioceramic sealers are highly alkaline, providing a sustained antibacterial effect and actively promoting the regeneration of periapical bone and cementum.[4]
The application of these advanced materials requires precise clinical technique. The sealer is typically injected directly into the canal using a specialized capillary tip, followed by the insertion of a master gutta-percha cone that has been precisely matched to the size and taper of the final shaping file. This single-cone technique with bioceramic sealer ensures a dense, void-free obturation that significantly enhances the long-term prognosis of the treated tooth.
Endodontic Therapy vs. Tooth Extraction: A Clinical Comparison
Preserving the natural dentition through endodontic therapy is almost always clinically superior to extraction, as it maintains alveolar bone volume, prevents adjacent tooth migration, and supports optimal mastication.
When faced with a severely infected or damaged tooth, patients often weigh the options between saving the tooth versus extraction. From a clinical perspective, preserving the natural tooth is always the primary objective whenever structurally and biologically feasible. The natural periodontal ligament provides essential proprioceptive feedback during chewing, allowing the brain to regulate the force exerted by the jaw muscles. This sensory mechanism is entirely lost when a tooth is extracted and replaced with an implant or bridge.
Furthermore, the roots of natural teeth stimulate the surrounding alveolar bone, maintaining its density and volume. When a tooth is extracted, the bone in that area immediately begins to resorb (shrink) due to the lack of mechanical stimulation. This bone loss can compromise the stability of adjacent teeth and alter the patient’s facial aesthetics over time. While tooth extraction may seem like a quicker or less expensive short-term solution, the long-term biological and financial costs of replacing the missing tooth—to prevent shifting, bite collapse, and bone loss—far exceed the investment of a root canal and crown.
| Clinical Factor | Root Canal Therapy (Endodontics) | Tooth Extraction & Replacement |
|---|---|---|
| Biological Preservation | Maintains the natural root, periodontal ligament, and surrounding alveolar bone. | Results in immediate loss of the tooth and initiates progressive alveolar bone resorption. |
| Masticatory Function | Retains natural proprioception and normal chewing efficiency. | Requires prosthetic replacement (implant/bridge) to restore function; proprioception is lost. |
| Treatment Timeline | Typically completed in 1-2 visits, followed by a crown placement within a few weeks. | Extraction is fast, but implant integration and final restoration can take 3-6 months. |
| Long-Term Cost | Highly cost-effective over a lifetime; prevents the need for complex prosthetics. | Initial extraction is cheap, but subsequent implant or bridge placement is significantly more expensive. |
Advanced Technologies Elevating Endodontic Success
The integration of surgical operating microscopes, 3D cone-beam computed tomography, and ultrasonic irrigation has revolutionized endodontics, allowing for unprecedented precision and significantly higher clinical success rates.
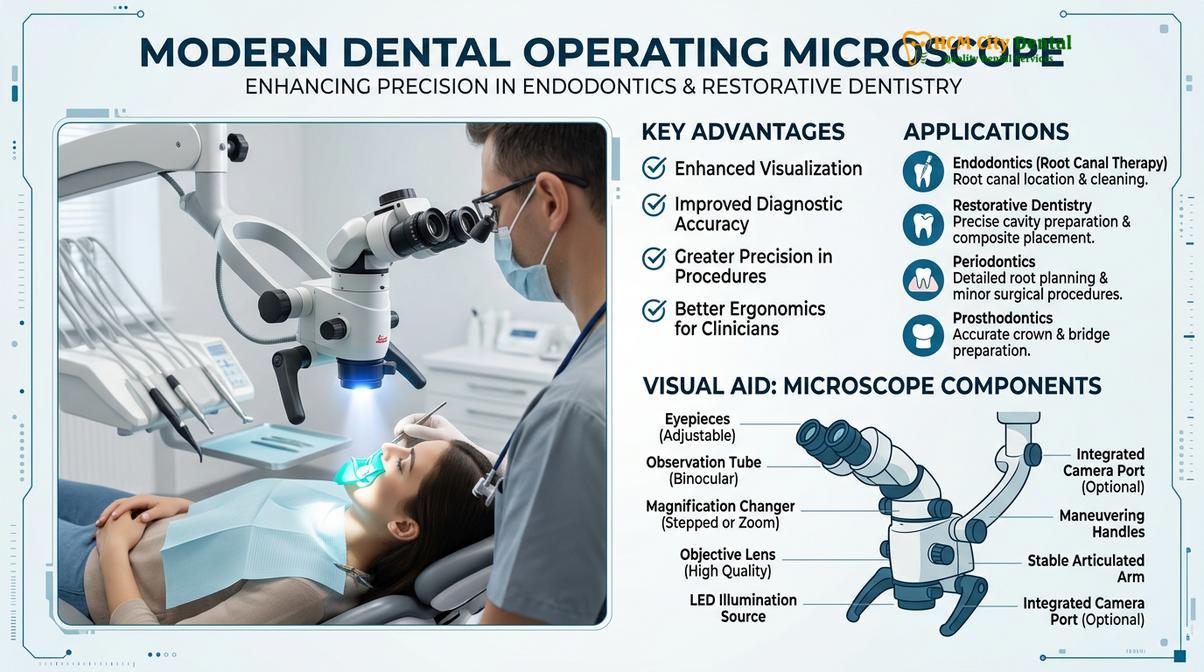
The field of endodontics has experienced a technological renaissance over the past two decades, transitioning from a procedure reliant heavily on tactile sensation to one driven by extreme visual precision. One of the most critical advancements is the widespread adoption of the Dental Operating Microscope (DOM). A microscope provides intense, coaxial illumination and magnification up to 25x, allowing the clinician to peer deep into the root canal system. This enhanced visualization is essential for locating hidden accessory canals, identifying micro-fractures, and safely removing calcifications that would otherwise compromise the treatment outcome.
In addition to enhanced magnification, 3D Cone-Beam Computed Tomography (CBCT) has become an invaluable diagnostic tool in complex endodontic cases. Unlike traditional 2D radiographs, which compress a three-dimensional structure into a flat image, CBCT provides high-resolution, cross-sectional views of the tooth and surrounding bone in all three planes of space. This allows the clinician to accurately assess the true extent of periapical lesions, navigate complex root curvatures, and plan the surgical approach with millimeter precision.
Electronic Apex Locators (EALs) have also standardized the accuracy of root canal shaping. These sophisticated devices use multi-frequency electrical impedance to precisely determine the location of the apical constriction (the narrowest point of the root canal, where the preparation and filling should terminate). By combining EAL readings with radiographic verification, clinicians can ensure that the entire canal is cleaned without over-instrumenting and damaging the delicate periapical tissues.
“The integration of the surgical operating microscope has fundamentally changed how we approach endodontic therapy. We are no longer working blindly by feel; we can visually confirm the complete debridement of the canal system, which directly translates to higher success rates and better long-term outcomes for our patients.”
— Dr. Nguyen Van Cuong, Clinical Director
Post-Operative Care and Long-Term Prognosis
Following endodontic therapy, patients must adhere to specific post-operative guidelines to manage transient inflammation and ensure the long-term structural integrity of the restored tooth.
The immediate post-operative phase following a root canal treatment is generally characterized by mild to moderate tissue inflammation. Because the instruments and chemical irrigants work precisely at the root apex, the surrounding periodontal ligament may become temporarily bruised or irritated. Patients often report a sensation of tenderness when biting down or applying pressure to the treated tooth. This is a normal physiological healing response and does not indicate that the procedure was unsuccessful.
To manage this transient discomfort, clinicians typically recommend a regimen of over-the-counter non-steroidal anti-inflammatory drugs (NSAIDs), such as Ibuprofen, taken on a scheduled basis for the first 48 to 72 hours. For patients seeking advice on managing severe toothache prior to or immediately following treatment, adhering strictly to the prescribed pharmacological protocol is crucial. It is also advised to avoid chewing hard or sticky foods on the treated side until the definitive coronal restoration (crown) has been placed, as the tooth is highly susceptible to fracture while only protected by a temporary filling.
The long-term prognosis for an endodontically treated tooth is exceptionally high, often exceeding 90-95% when the procedure is performed to modern standards and the tooth is properly restored.[5] In cases where a chronic sinus tract was present, the ongoing dental fistula treatment effect is usually observed as the tract heals and closes naturally within a few weeks, confirming that the source of the infection within the canal has been successfully eradicated. Regular dental check-ups and routine radiographic monitoring are essential to verify continuous periapical healing and to ensure the marginal integrity of the final crown.
Clinical Case Study: Complex Molar Rehabilitation
Complex anatomical variations, such as severely curved canals or calcified spaces, require specialized endodontic techniques and advanced instrumentation to achieve complete disinfection and successful preservation.
The true test of modern endodontic capabilities lies in the management of anatomically complex teeth. Mandibular molars, for instance, frequently present with intricate canal configurations, including sharp apical curvatures, C-shaped canal systems, or calcified orifices resulting from long-standing chronic irritation. Successfully navigating and disinfecting these challenging anatomies requires a combination of advanced technology, specialized flexible NiTi files, and extensive clinical experience.
Clinical Case Review: Severe Apical Periodontitis in a Mandibular Molar
A 45-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City complaining of severe, spontaneous throbbing pain localized to the lower right quadrant. Clinical examination and CBCT imaging revealed a large periapical radiolucency (infection) associated with the mandibular first molar (Tooth 46). The tooth exhibited complex anatomy with four distinct canals, two of which possessed severe 90-degree apical curvatures. Under the magnification of a surgical operating microscope, Dr. Nguyen Van Cuong meticulously negotiated the calcified orifices and utilized heat-treated, highly flexible rotary files to shape the curved canals without causing transportation or ledging. Copious ultrasonic irrigation was employed to dissolve the necrotic tissue deep within the isthmuses. The canals were successfully obturated using a warm vertical compaction technique with bioceramic sealer. At the 6-month follow-up, radiographic evaluation demonstrated complete bone regeneration and healing of the periapical lesion, allowing the patient to retain their natural tooth and avoid a complex extraction.
“Cases involving severe root curvatures demand immense patience and respect for the natural anatomy. By leveraging 3D imaging and advanced metallurgy in our files, we can now predictably save teeth that would have undoubtedly been slated for extraction just a decade ago.”
— Dr. Nguyen Van Cuong, reflecting on complex endodontic rehabilitation.
When to See a Doctor
While transient tenderness is expected following a root canal, certain clinical signs warrant immediate professional evaluation. Patients should contact their dental provider if they experience any of the following red flag symptoms:
- Severe, Unrelenting Pain: Pain that progressively worsens over several days and is not alleviated by maximum doses of over-the-counter analgesics.
- Visible Facial Swelling: Any swelling that extends beyond the immediate gum area, particularly swelling of the cheek, jawline, or under the eye, indicating a spreading infection.
- Return of the Sinus Tract: The reappearance of a pimple-like bump on the gums weeks or months after treatment, suggesting a persistent or secondary infection.
- Loss of the Temporary Filling: If the temporary restorative material falls out, the canal system is immediately exposed to oral bacteria, requiring prompt resealing to prevent contamination.
- Systemic Symptoms: The onset of a fever, chills, or difficulty swallowing or breathing are medical emergencies that require immediate intervention, potentially involving intravenous antibiotics.
For patients experiencing deep decay or structural damage, understanding the nuances of deep decay restorations and seeking timely consultation at a specialized facility like HCMC Dental Clinic can prevent the need for more invasive procedures. A comprehensive clinical evaluation is always required to determine the most appropriate and personalized treatment plan.

If you are experiencing symptoms of pulpitis or require a second opinion regarding a failing tooth, we encourage you to seek a professional assessment. For more information on our comprehensive approach to oral health, please explore our general dental procedures and clinical resources.
Frequently Asked Questions
Is root canal treatment a painful procedure?
Modern root canal treatment is highly effective at relieving pain rather than causing it, utilizing profound local anesthesia to ensure a comfortable experience. Patients typically feel pressure rather than sharp pain during the procedure. Post-operative discomfort is usually mild and can be managed effectively with over-the-counter anti-inflammatory medications as the periapical tissues heal.
How long does a standard root canal procedure take?
A standard root canal procedure generally takes between 60 to 90 minutes per session, depending on the tooth’s anatomical complexity and the number of canals. Anterior teeth with single canals are treated faster, while multi-rooted molars with curved canals may require longer appointments or be completed across two separate clinical visits.
Why is a dental crown often required after endodontic therapy?
A dental crown is highly recommended after endodontic therapy to restore the tooth’s structural integrity and prevent catastrophic fractures during mastication. Because the tooth loses its internal blood supply, the remaining dentin becomes more brittle over time. A full-coverage crown distributes chewing forces evenly and provides a hermetic seal against bacterial microleakage.
Can a tooth become infected again after a root canal?
While root canal therapy has a very high success rate, secondary infections can occur if the coronal restoration fails, allowing bacteria to re-enter the canal system. Additionally, undetected accessory canals or complex root anatomy can harbor residual bacteria. In such cases, endodontic retreatment or apical surgery may be necessary to save the tooth.
What are the clinical alternatives to root canal treatment?
The primary clinical alternative to root canal treatment is the complete extraction of the infected tooth, followed by prosthetic replacement. To prevent adjacent teeth from shifting and to maintain alveolar bone volume, the extracted tooth must be replaced with a dental implant, a fixed dental bridge, or a removable partial denture.
References
- American Association of Endodontists. Endodontic diagnosis, treatment protocols, and clinical outcomes. (2021).
- Journal of Endodontics. Microbiology and pathogenesis of primary root canal infections. (2020).
- International Endodontic Journal. Long-term survival rates of non-surgical root canal treatment. (2019).
- Journal of the American Dental Association. The efficacy of bioceramic sealers in modern endodontic obturation. (2022).
- Clinical Oral Investigations. Biomechanical considerations for post-endodontic restorations and crowns. (2018).