A narrow dental arch occurs when the upper or lower jaw lacks sufficient transverse width to accommodate all teeth, leading to severe crowding, crossbites, and potential airway restriction. Clinical intervention involves orthodontic expansion or surgical widening to restore proper occlusion, facial symmetry, and functional respiratory dynamics. Addressing this condition requires a deep understanding of craniofacial growth, biomechanics, and the intricate relationship between the oral cavity and the nasal airway.
Clinical Summary:
Narrow arch teeth present a complex orthodontic and skeletal challenge characterized by transverse maxillary or mandibular deficiency. This condition frequently results in dental crowding, posterior crossbites, and compromised respiratory function due to a narrowed nasal floor. Treatment modalities range from early interceptive orthodontics using rapid palatal expanders (RPE) in growing children to surgically-assisted rapid palatal expansion (SARPE) or miniscrew-assisted rapid palatal expansion (MARPE) in skeletally mature adults. Comprehensive diagnostic imaging, including Cone Beam Computed Tomography (CBCT), and multidisciplinary planning are essential to achieve stable, functional, and aesthetic outcomes while minimizing periodontal risks such as buccal bone fenestration and gingival recession.
Key Takeaways:
- A narrow dental arch restricts space for permanent teeth, causing severe crowding, ectopic eruptions, and complex malocclusions.
- Transverse maxillary deficiency is anatomically linked to a narrow nasal cavity, increasing the risk of chronic mouth breathing and sleep-disordered breathing.
- Early intervention in children utilizes natural skeletal growth for non-surgical sutural expansion, yielding highly predictable results.
- Adults with fused midpalatal sutures often require bone-anchored or surgically-assisted expansion to achieve stable skeletal widening without damaging the periodontium.
- Comprehensive multidisciplinary treatment improves dental alignment, respiratory function, and overall facial aesthetics, requiring careful coordination between orthodontists and oral surgeons.
Understanding Narrow Arch Teeth: Clinical Definition and Etiology
A narrow dental arch is a transverse skeletal or dentoalveolar deficiency where the jaw is too narrow to properly align the dentition. This condition stems from a combination of genetic predispositions, chronic mouth breathing, and prolonged childhood habits that disrupt normal craniofacial development.
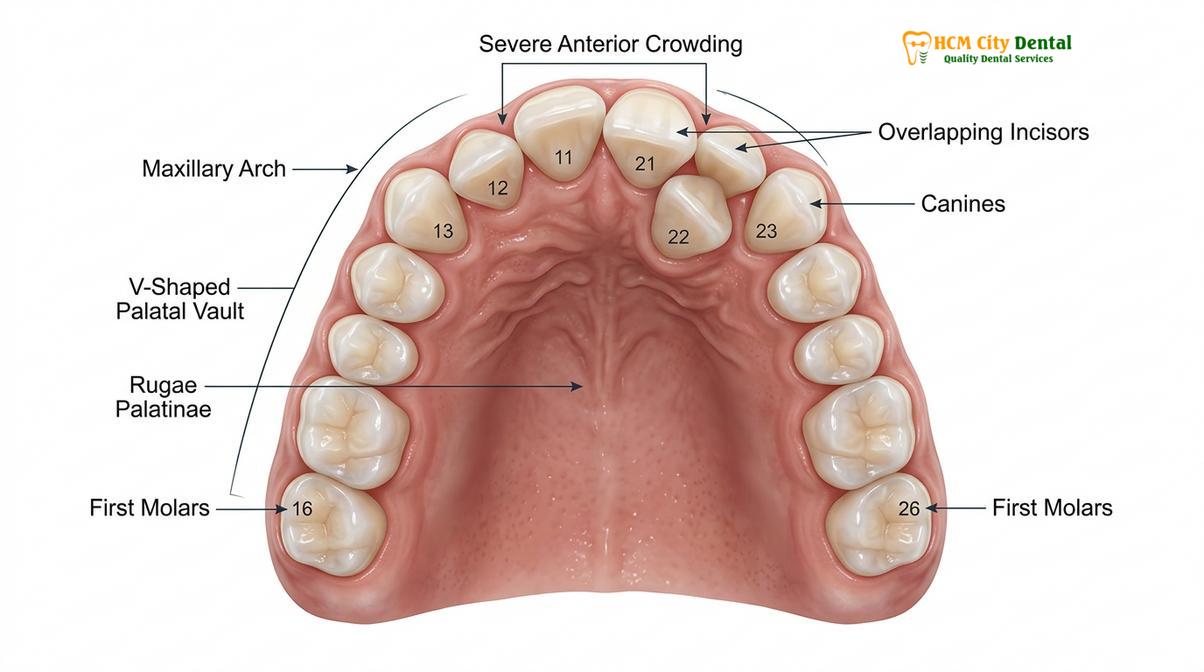
In the realm of orthodontics and craniofacial orthopedics, the comprehensive evaluation of structural anomalies is paramount. The formal dental arch definition encompasses the parabolic or U-shaped alveolar ridge and the teeth it supports. In a healthy, well-developed stomatognathic system, the arch is broad enough to house all permanent teeth without overlapping, allowing for a harmonious intercuspation between the maxillary and mandibular dentition. However, when transverse growth is stunted, the arch assumes a constricted, V-shaped morphology that severely limits the available arch perimeter.
Evaluating normal dental arch dimensions requires precise measurement of the intercanine and intermolar widths. Clinically, a transverse discrepancy is identified when the width of the maxillary arch is significantly narrower than that of the mandibular arch, often resulting in a unilateral or bilateral posterior crossbite. The etiology of a narrow arch is multifactorial, blending genetic inheritance with profound environmental influences during critical periods of craniofacial growth[1]. Understanding these root causes is essential for developing an effective, long-term treatment strategy.
Genetically, patients may inherit a skeletal Class II or Class III tendency that naturally predisposes them to transverse deficiencies. Familial traits often dictate the baseline size and shape of the basal bone. However, environmental factors and functional habits frequently exacerbate these genetic predispositions. The resting posture of the tongue plays a critical, continuous role in shaping the palate. In a normal physiological state, the tongue rests against the roof of the mouth, exerting a gentle, outward pressure that counterbalances the inward forces of the buccal (cheek) musculature. This equilibrium is known as the buccinator mechanism.
If a patient suffers from chronic allergic rhinitis, enlarged adenoids, hypertrophic tonsils, or a severe tongue tie (ankyloglossia), they are often forced into an obligatory mouth-breathing pattern to maintain an adequate airway. Consequently, the tongue drops to the floor of the mouth to allow air to pass over it, removing the internal expansive force against the palate. The unopposed pressure from the cheek muscles gradually constricts the maxilla during its formative years, leading to a high palatal vault, a narrow dental arch, and a subsequent lack of space for the erupting permanent dentition. Prolonged non-nutritive sucking habits, such as thumb or pacifier sucking, further distort the anterior maxilla, creating an open bite and exacerbating the transverse constriction.
Diagnostic Criteria and Clinical Complications
Diagnosing a narrow arch involves clinical evaluation of transverse discrepancies, posterior crossbites, and severe dental crowding. Untreated cases often lead to compromised periodontal health, temporomandibular joint (TMJ) dysfunction, and restricted airway volume.
The diagnostic workflow for a narrow dental arch extends far beyond a simple visual inspection of crowded teeth. Orthodontists and oral surgeons utilize a combination of comprehensive clinical examinations, digital study models, and Cone Beam Computed Tomography (CBCT) to assess the exact nature of the transverse deficiency. It is crucial to differentiate between a purely dentoalveolar constriction—where the teeth are tipped inward but the underlying skeletal base is of normal width—and a true skeletal transverse deficiency, where the maxillary bone itself is physically too narrow[2].
CBCT imaging has revolutionized the diagnosis of transverse discrepancies. It allows clinicians to measure the exact width of the basal bone, evaluate the thickness of the buccal cortical plates, and assess the degree of ossification of the midpalatal suture. This three-dimensional perspective is vital for determining whether a patient is a candidate for traditional orthodontic expansion or if they require surgical intervention to prevent iatrogenic damage to the periodontium.
When a patient presents with a narrow arch, several cascading clinical complications typically arise. The most immediate and visible issue is severe dental crowding. Because the perimeter of the arch is insufficient, erupting permanent teeth are forced into ectopic positions, leading to overlapping, rotation, and impaction. Attempting to resolve dental crowding in these scenarios without addressing the underlying skeletal width often results in unstable outcomes, an increased risk of orthodontic relapse, and potential damage to the roots of the teeth.
“Transverse maxillary deficiency is not merely an orthodontic dilemma; it is a fundamental airway issue. Expanding the maxilla increases the volume of the nasal cavity, significantly reducing airway resistance and playing a critical role in the multidisciplinary management of pediatric and adult obstructive sleep apnea.”
Beyond the dentition, the anatomical relationship between the maxilla and the nasal cavity makes a narrow arch a significant medical concern. The roof of the mouth is simultaneously the floor of the nasal cavity. Therefore, a constricted maxilla directly correlates with increased nasal airway resistance and a narrowed nasal passage. Patients with untreated narrow arches are highly susceptible to sleep-disordered breathing, ranging from upper airway resistance syndrome (UARS) to severe obstructive sleep apnea (OSA)[4]. The chronic lack of restorative sleep impacts cognitive development and behavioral patterns in children, while in adults, it is linked to hypertension and cardiovascular strain. Educating patients on these systemic impacts is a core component of Ethical Dental Ads: Clinical Marketing & Patient Education | HCMC Dental.
Furthermore, a narrow arch often forces the lower jaw to shift laterally upon closure to achieve maximum intercuspation, creating a functional shift. Over time, this asymmetric loading can lead to temporomandibular joint (TMJ) disorders, muscular pain, and asymmetric wear of the dental enamel. Addressing the transverse dimension is therefore the foundational first step in comprehensive orthodontic rehabilitation.

Non-Surgical Orthodontic Expansion Workflows
Non-surgical expansion utilizes orthodontic appliances like rapid palatal expanders (RPE) or clear aligners to gradually widen the maxilla. This approach is highly effective in growing children and adolescents before the midpalatal suture fully ossifies.
The timing of intervention is the most critical factor in non-surgical palatal expansion. The maxilla is composed of two halves joined centrally by the midpalatal suture. In children and early adolescents, this suture is composed of fibrous connective tissue and is highly responsive to orthopedic forces. As the patient matures, the suture undergoes heavy interdigitation and eventually ossifies, making traditional non-surgical expansion highly unpredictable and potentially harmful in adults.
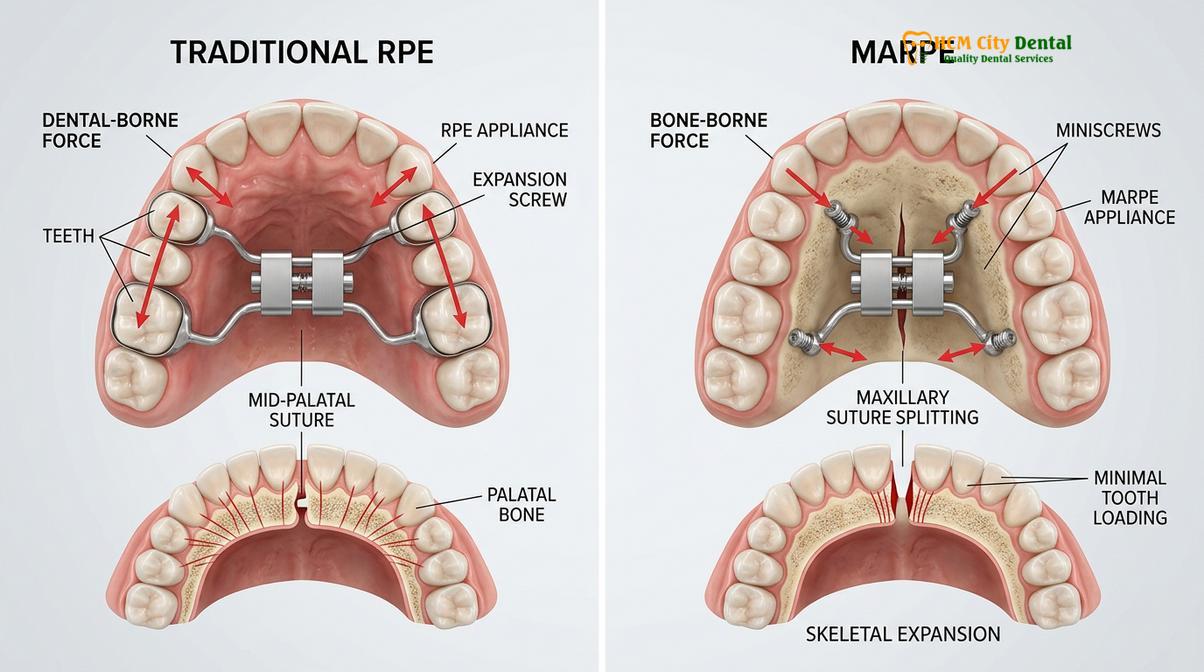
For growing patients, the Rapid Palatal Expander (RPE) remains the gold standard. This custom-made appliance is typically banded or bonded to the posterior teeth (usually the first molars and premolars) and features a central jackscrew positioned against the palate. The screw is activated daily by the patient or parent, delivering heavy, intermittent orthopedic forces that separate the two halves of the maxilla. As the suture opens, a temporary diastema (gap) appears between the upper central incisors—a definitive clinical sign of successful skeletal expansion. Once the desired width is achieved, the appliance is left in place for several months to allow new bone to fill the sutural gap.
Recently, Miniscrew-Assisted Rapid Palatal Expansion (MARPE) has revolutionized non-surgical expansion for late adolescents and young adults. MARPE utilizes temporary anchorage devices (TADs)—small titanium micro-implants—placed directly into the palatal bone alongside a central expansion screw. By anchoring the expander to the dense palatal bone rather than relying solely on the teeth, MARPE delivers forces directly to the midpalatal suture. This biomechanical advantage minimizes the unwanted buccal tipping of the posterior teeth, reduces stress on the periodontal ligament, and expands the limits of non-surgical treatment in skeletally mature patients[3].
For patients with mild dentoalveolar constriction rather than true skeletal deficiency, clear aligner therapy can be an effective tool. Aligners can predictably upright lingually tipped posterior teeth, broadening the smile arch and creating space for anterior alignment. This approach is particularly popular among adults seeking aesthetic improvements without the need for bulky palatal appliances. Understanding the nuances of tooth morphology, such as Line Angle Dental Anatomy: Clinical Guide to Esthetics | HCMC Dental, helps clinicians design aligner treatments that maximize the visual impact of a broadened arch.
| Expansion Modality | Primary Mechanism | Ideal Patient Demographic | Clinical Advantages |
|---|---|---|---|
| Traditional RPE | Tooth-borne skeletal expansion | Children and early adolescents | Highly predictable sutural separation; utilizes natural growth potential. |
| Clear Aligners | Dentoalveolar uprighting (tipping) | Adults with mild to moderate crowding | Aesthetic, comfortable; excellent for minor arch broadening and alignment. |
| MARPE | Bone-anchored skeletal expansion | Late adolescents and young adults | Direct skeletal force; minimizes periodontal stress on posterior teeth. |
| SARPE | Surgically-assisted skeletal expansion | Skeletally mature adults | Overcomes fused sutures; highly stable for severe transverse discrepancies. |
Surgically-Assisted Rapid Palatal Expansion (SARPE)
SARPE is a combined orthodontic and surgical procedure designed to widen the maxillary arch in skeletally mature adults. By surgically releasing the fused midpalatal suture, the jaw can be expanded predictably without excessive tipping of the teeth.
When a skeletally mature adult presents with a severe transverse maxillary deficiency, traditional tooth-borne expanders are generally contraindicated. Applying heavy expansive forces to a fused maxilla will not open the suture; instead, it may push the roots of the posterior teeth through the buccal cortical bone. This iatrogenic movement can cause severe periodontal fenestrations, gingival recession, and potential tooth loss[5]. In these complex scenarios, Surgically-Assisted Rapid Palatal Expansion (SARPE) is the definitive and safest treatment protocol.
The SARPE workflow is a meticulously coordinated effort between the orthodontist and the oral maxillofacial surgeon. The process begins with a pre-surgical orthodontic phase to align the teeth, level the arches, and remove any dental compensations that have developed over time. Once the dentition is prepared, the patient undergoes the surgical phase, typically performed under general anesthesia or deep intravenous sedation in an outpatient surgical setting.
During the procedure, the surgeon performs a modified Le Fort I osteotomy. This involves making precise bone cuts along the lateral walls of the maxilla and releasing the pterygomaxillary junctions to free the upper jaw from its cranial attachments. Crucially, a conservative osteotomy is also performed along the midpalatal suture to release the primary area of skeletal resistance. A custom-fitted palatal expander is placed either before or during the surgery.
Important Clinical Considerations for SARPE:
While SARPE is highly effective, it is a major surgical intervention. Patients must be thoroughly evaluated for contraindications such as severe bleeding disorders, uncontrolled systemic diseases, or compromised bone density. Post-operative risks include transient epistaxis (nosebleeds), sinus congestion, and temporary neurosensory deficits in the infraorbital region. Strict adherence to post-operative hygiene, soft dietary protocols, and prescribed medication regimens is mandatory to prevent complications and ensure optimal healing.
Following a brief latency period of a few days to allow initial soft tissue healing, the activation phase begins. The patient turns the expander screw daily, gradually widening the maxilla at a rate of approximately 0.5mm to 1.0mm per day. Once the desired transverse width is achieved, the expander is locked in place for a consolidation period of four to six months. This extended retention phase is critical; it allows the newly formed osteoid tissue within the expanded suture to mineralize and mature into solid, stable bone.
Following the consolidation phase, the expander is removed, and comprehensive orthodontic treatment continues to detail the occlusion, close the anterior diastema, and establish proper intercuspation. In cases where previous extractions were performed due to severe crowding, or if teeth were congenitally missing, the newly created space might require multidisciplinary prosthodontic planning. Procedures such as Replacing Extracted Teeth: Implants, Bridges & Partials | HCMC Dental may be integrated to stabilize the expanded arch and restore full masticatory function.
When to Consult a Specialist and Important Clinical Considerations
Early diagnosis is critical for managing transverse discrepancies effectively. Identifying signs of a narrow arch during childhood allows for interceptive treatments that guide proper skeletal growth and prevent complex surgical needs later in life.
In alignment with recommendations from health authorities and the Vietnam Odonto-Stomatology Association (VOSA), early orthodontic evaluation is highly encouraged to identify transverse discrepancies before skeletal maturation occurs. VOSA guidelines suggest that children should undergo their first comprehensive orthodontic screening during the early mixed dentition phase. This proactive approach allows clinicians to detect skeletal imbalances while the craniofacial sutures are still highly adaptable.
Parents should actively monitor their children for clinical signs such as chronic mouth breathing, audible snoring, prolonged thumb-sucking habits, or visible crowding of the primary teeth. If a child exhibits a crossbite, a noticeably V-shaped upper jaw, or difficulty chewing, a consultation with an orthodontic specialist is strongly warranted. Interceptive treatment at this stage can often resolve the transverse deficiency entirely using simple, non-invasive appliances, thereby guiding the permanent teeth into favorable positions and improving nasal airway volume.
For adults, symptoms such as chronic jaw pain, difficulty chewing, severe dental crowding, or diagnosed obstructive sleep apnea should prompt a comprehensive dental evaluation. While adult treatment is inherently more complex due to skeletal maturity, modern surgical and bone-anchored techniques offer highly viable pathways to achieve a functional and aesthetic smile. Patients must be prepared for a longer treatment duration and a multidisciplinary approach, but the functional and aesthetic rewards are substantial.
Multidisciplinary Treatment: Orthodontics and Oral Surgery
Complex narrow arch cases require seamless collaboration between orthodontists, oral maxillofacial surgeons, and prosthodontists to achieve optimal skeletal and dental harmony. Comprehensive digital planning ensures precise execution of both expansion and subsequent tooth alignment.
Dr. Nguyen Van Cuong emphasizes that treating a narrow arch requires a holistic view of the patient’s craniofacial anatomy, periodontal health, and functional occlusion. By applying the advanced principles of General Dentistry tại HCMC Dental Clinic, Dr. Cuong and his clinical team integrate state-of-the-art 3D imaging and digital smile design to ensure precise execution of both expansion and subsequent tooth alignment. This comprehensive, patient-centered approach helps mitigate surgical risks, protects the periodontium, and promotes stable, long-term functional outcomes.
Digital treatment planning allows the clinical team to simulate the expansion vectors, predict soft tissue changes, and design custom surgical guides and appliances. This level of precision is particularly vital when combining SARPE with subsequent orthognathic surgeries to correct complex Class II or Class III malocclusions. In some instances, severely impacted or ectopic teeth that cannot be salvaged during the expansion process may require removal. In such cases, protocols for Tooth Extraction Saigon: Safe Outpatient Oral Surgery | HCMC Dental are seamlessly integrated into the treatment plan to ensure patient comfort and safety.
“The synergy between orthodontics and oral surgery ensures that the biological limits of the bone are respected. By expanding the skeletal base rather than merely tipping the teeth, we prevent iatrogenic damage, enhance airway dynamics, and ensure long-term occlusal stability.”
Clinical Case Review: Adult Maxillary Expansion
A 28-year-old male presented to HCMC Dental Clinic in Ho Chi Minh City with a chief complaint of severe upper crowding, a unilateral posterior crossbite, and chronic mouth breathing. Clinical examination and CBCT evaluation revealed a 7mm transverse maxillary deficiency with a fully ossified midpalatal suture. The multidisciplinary treatment plan involved a SARPE procedure followed by clear aligner therapy. Post-surgery, the maxilla was successfully expanded by 8mm over a three-week activation period. Following a 5-month consolidation phase, aligners were utilized to detail the occlusion, upright the posterior segments, and close the central diastema. The patient reported not only a dramatically improved aesthetic smile but also a significant enhancement in nasal breathing and overall sleep quality.

References
- American Journal of Orthodontics and Dentofacial Orthopedics. Transverse maxillary deficiency: Diagnosis and treatment planning. (2021).
- Journal of Oral and Maxillofacial Surgery. Surgically assisted rapid palatal expansion: A comprehensive review of techniques and outcomes. (2020).
- Angle Orthodontist. Miniscrew-assisted rapid palatal expansion (MARPE) in late adolescents and adults. (2019).
- Sleep Medicine Reviews. The impact of rapid maxillary expansion on the nasal airway and obstructive sleep apnea. (2022).
- International Journal of Periodontics & Restorative Dentistry. Periodontal implications of orthodontic expansion in adults. (2018).
If you are experiencing symptoms of a narrow arch, severe dental crowding, or related airway issues, contact HCMC Dental Clinic in Ho Chi Minh City for a comprehensive evaluation. Our multidisciplinary team utilizes advanced diagnostics and evidence-based protocols to design personalized expansion treatments. Discover more about our comprehensive approach by visiting our guide to General Dentistry tại HCMC Dental Clinic.