

A check up and clean dentist visit is a structured preventive appointment involving a comprehensive clinical examination of the oral cavity, periodontal probing, oral cancer screening, and professional biofilm removal. This routine procedure diagnoses pathologies early and maintains optimal gingival health through targeted scaling and polishing.
Clinical Summary:
The comprehensive dental check-up and professional prophylaxis represent the cornerstone of preventive dentistry. This clinical protocol goes far beyond a simple visual inspection; it encompasses a systematic evaluation of hard and soft tissues, periodontal health assessment, and the mechanical disruption of pathogenic biofilm. By utilizing advanced diagnostic tools such as digital radiography and periodontal probing, clinicians can detect early-stage dental caries, gingival inflammation, and potentially malignant lesions before they progress into complex, irreversible conditions. The therapeutic phase—scaling and polishing—effectively removes calcified deposits (calculus) that cannot be eliminated through domestic oral hygiene practices. Regular visits to a check up and clean dentist are essential for mitigating the bidirectional risks associated with oral dysbiosis and systemic health conditions, ensuring long-term functional and aesthetic stability.
Key Takeaways:
- A comprehensive check-up includes medical history review, extraoral/intraoral exams, and oral cancer screening.
- Professional scaling utilizes ultrasonic cavitation and hand instrumentation to remove subgingival calculus.
- Periodontal probing measures gingival sulcus depth to objectively assess gum health and attachment loss.
- Digital radiographs are prescribed based on individualized risk assessments to detect hidden pathologies.
- Recall intervals should be customized (typically 3 to 12 months) based on a patient’s specific clinical risk profile.
The Clinical Scope of a Dental Check-Up and Clean
A comprehensive dental check-up and clean encompasses a systematic evaluation of hard and soft tissues, combined with professional prophylaxis to remove calcified deposits and bacterial biofilm.
The modern paradigm of dentistry has shifted decisively from a reactive, surgical model to a proactive, preventive approach. At the heart of this philosophy is the routine visit to a check up and clean dentist. While patients often perceive this appointment merely as a “teeth cleaning,” it is, in reality, a rigorous diagnostic and therapeutic intervention designed to preserve the integrity of the stomatognathic system. The oral cavity is a complex ecosystem harboring hundreds of bacterial species; when this microbiome falls into dysbiosis, it initiates a cascade of inflammatory responses leading to dental caries and periodontal disease [1].
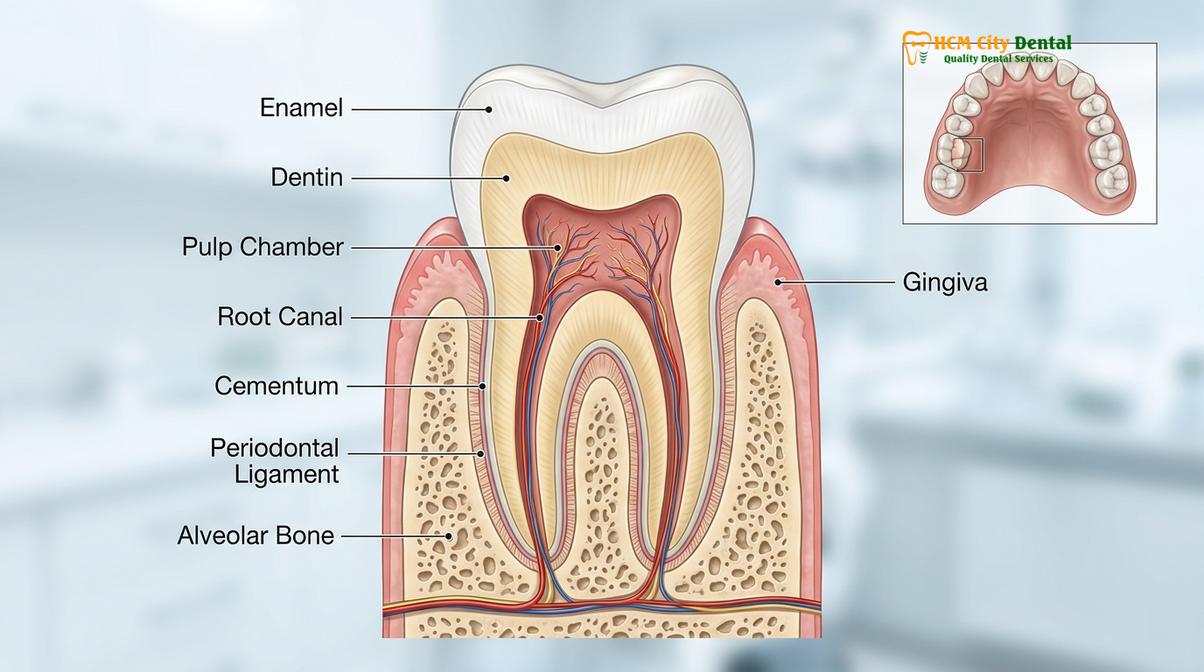
A comprehensive examination serves as the primary diagnostic gateway. It allows the clinician to establish a baseline of the patient’s oral health, monitor longitudinal changes, and intercept pathologies at their most nascent stages. For instance, detecting a non-cavitated carious lesion (early enamel demineralization) allows for conservative remineralization therapies rather than invasive restorative procedures. Similarly, identifying early signs of gingivitis prevents the progression to irreversible periodontitis, which involves the destruction of the alveolar bone supporting the teeth.

Furthermore, the systemic-oral connection cannot be overstated. Extensive clinical research has established robust links between chronic oral inflammation (such as periodontitis) and systemic conditions, including cardiovascular disease, poorly controlled diabetes mellitus, and adverse pregnancy outcomes [2]. Therefore, a thorough check-up is not just about preserving teeth; it is a vital component of holistic health management. When patients visit General Dentistry professionals at HCMC Dental Clinic in Ho Chi Minh City, they undergo a structured evaluation that integrates their systemic health profile with their localized oral findings.
Step-by-Step Diagnostic Workflow in the Dental Chair
The diagnostic phase follows a strict protocol, beginning with medical history review, followed by extraoral and intraoral examinations, periodontal charting, and oral cancer screening.
The clinical workflow of a comprehensive dental examination is highly structured to ensure no pathology is overlooked. This systematic approach begins before the clinician even examines the oral cavity. The first critical step is the acquisition and review of a detailed medical history. The dentist must evaluate the patient’s current medications, systemic illnesses, allergies, and previous surgical interventions. For example, a patient taking bisphosphonates for osteoporosis requires specific clinical considerations due to the risk of medication-related osteonecrosis of the jaw (MRONJ). Similarly, patients on anticoagulant therapy or those with poorly controlled diabetes require tailored treatment planning to manage bleeding risks and delayed wound healing.
Following the medical history review, the clinician performs an extraoral examination. This involves the visual inspection and bilateral palpation of the head and neck region. The dentist assesses the temporomandibular joint (TMJ) for signs of crepitus (clicking/popping), deviation upon opening, or muscular tenderness, which may indicate temporomandibular disorders (TMD) or bruxism. The submandibular, submental, and cervical lymph nodes are palpated to detect any lymphadenopathy, which could signify an active infection or, more concerningly, a malignant process.
The intraoral examination is a meticulous, tooth-by-tooth, and tissue-by-tissue assessment. The clinician evaluates the integrity of existing restorations (fillings, crowns, bridges), checking for marginal leakage, recurrent decay, or structural failure. The hard tissues are examined for primary carious lesions, non-carious cervical lesions (abfraction, abrasion, erosion), and occlusal wear facets indicative of parafunctional habits. If a patient presents with severe wear or a constricted maxillary arch, the clinician might discuss functional corrections, potentially referencing concepts related to Narrow Arch Teeth expansion or restorative rehabilitation.
A critical, yet often underappreciated, component of the intraoral exam is periodontal probing. Using a calibrated periodontal probe, the clinician measures the depth of the gingival sulcus (the space between the tooth and the gum tissue) at six specific sites around every tooth. This objective measurement, combined with the assessment of bleeding on probing (BOP) and clinical attachment loss (CAL), dictates the periodontal diagnosis.
| Probing Depth (mm) | Clinical Condition | Therapeutic Implication |
|---|---|---|
| 1 – 3 mm | Healthy Gingiva | Routine prophylaxis and standard home care maintenance. |
| 4 mm (with bleeding) | Gingivitis / Early Periodontitis | Requires targeted scaling, improved oral hygiene, and closer monitoring. |
| 5 – 6 mm | Moderate Periodontitis | Indicates active bone loss; requires scaling and root planing (deep cleaning). |
| 7+ mm | Severe Periodontitis | Advanced attachment loss; may require surgical intervention or specialist referral. |
Finally, a comprehensive oral cancer screening is conducted. The dentist systematically examines the lateral borders of the tongue, the floor of the mouth, the hard and soft palate, and the buccal mucosa. Any persistent ulcerations, leukoplakia (white patches), erythroplakia (red patches), or indurated (hardened) lesions are documented, and if necessary, referred for biopsy. This screening is a life-saving protocol, as early detection of oral squamous cell carcinoma drastically improves survival rates.
The Mechanics of Professional Teeth Cleaning (Prophylaxis)
Professional dental cleaning utilizes ultrasonic cavitation and precise hand instrumentation to disrupt pathogenic biofilm and remove calculus, followed by coronal polishing to smooth enamel surfaces.
Once the diagnostic phase is complete, the therapeutic phase—commonly referred to as the “clean”—commences. The primary objective of professional dental prophylaxis is the mechanical disruption and removal of dental plaque (a sticky, bacteria-laden biofilm) and dental calculus (tartar). Calculus is formed when the calcium and phosphate ions present in saliva precipitate into the plaque matrix, calcifying it into a hard, porous deposit. Because calculus is firmly adherent to the tooth surface, it cannot be removed by domestic toothbrushing or flossing; it requires professional instrumentation [3].
The cornerstone of modern calculus removal is the ultrasonic scaler. These devices operate by converting electrical energy into high-frequency mechanical vibrations (typically ranging from 25,000 to 42,000 cycles per second) at the instrument tip. There are two main types of ultrasonic scalers: magnetostrictive and piezoelectric. Regardless of the specific technology, ultrasonic scalers achieve calculus removal through a combination of mechanical chipping and acoustic microstreaming. As the tip vibrates, it shatters the calcified deposits. Simultaneously, a continuous stream of water acts as a coolant to prevent thermal damage to the tooth pulp. This water flow, combined with the high-frequency vibration, creates a phenomenon known as cavitation—the formation and rapid implosion of microscopic bubbles. The energy released by these imploding bubbles effectively lyses (ruptures) the cell walls of periodontal pathogens, providing a profound antimicrobial effect within the periodontal pocket.
“The true clinical value of a professional cleaning lies not just in the aesthetic removal of superficial stains, but in the meticulous debridement of subgingival calculus. Disrupting the biofilm below the gumline is essential for arresting the inflammatory cascade that leads to alveolar bone loss.”
— Dr. Nguyen Van Cuong, Clinical Director
Following ultrasonic debridement, the clinician utilizes specialized hand instruments, such as Gracey curettes and universal scalers, for fine detailing. Hand scaling allows for superior tactile sensitivity, enabling the dentist or hygienist to detect and remove residual calculus deposits, particularly in anatomically complex areas like root concavities and furcations. The precise adaptation, angulation, and activation of these instruments ensure that the root surfaces are rendered biologically acceptable for gingival reattachment.

The final step of the mechanical cleaning is coronal polishing. Using a slow-speed handpiece equipped with a soft rubber cup or bristle brush, the clinician applies a prophylaxis paste to the teeth. This paste contains mild abrasives (such as pumice or perlite) designed to remove extrinsic stains caused by coffee, tea, tobacco, and certain foods. Beyond aesthetics, polishing smooths the enamel surface, making it more difficult for new plaque biofilm to adhere. Depending on the patient’s caries risk profile, the appointment often concludes with the topical application of fluoride varnish. Fluoride ions integrate into the hydroxyapatite structure of the enamel, converting it into fluorapatite, which is significantly more resistant to acid dissolution by cariogenic bacteria.
Diagnostic Imaging: When and Why X-Rays Are Necessary
Dental radiographs are essential diagnostic tools that reveal interproximal caries, periapical pathology, and alveolar bone levels invisible to the naked eye during a standard clinical exam.
A clinical visual examination, no matter how thorough, is inherently limited to the visible surfaces of the teeth and soft tissues. To achieve a comprehensive diagnosis, a check up and clean dentist must often peer beneath the enamel and below the gingival margin. This is where dental radiography becomes indispensable. Radiographs allow clinicians to detect pathologies that are asymptomatic and clinically invisible, facilitating early intervention and preventing complex complications.
The most common radiographs taken during a routine check-up are bitewings. These images capture the crowns of both the upper and lower teeth in a specific region, focusing on the interproximal areas (the contact points between adjacent teeth). Because the contact areas are tight, visual inspection and tactile probing with an explorer often fail to detect early interproximal caries. Bitewings reveal the extent of enamel demineralization and dentinal involvement, allowing the dentist to determine whether a lesion can be remineralized or if it requires a restorative intervention. Furthermore, bitewings provide an excellent view of the crestal alveolar bone, aiding in the early detection of periodontal bone loss.
Periapical radiographs are utilized when a specific tooth requires detailed evaluation from the crown down to the root apex and surrounding supporting bone. These images are crucial for diagnosing periapical abscesses, cysts, granulomas, and assessing the morphology of the root canal system prior to endodontic therapy. For a broader overview, a panoramic radiograph (OPG) may be prescribed. An OPG captures the entire maxillofacial complex, including the maxilla, mandible, TMJs, and maxillary sinuses. It is particularly useful for evaluating the position of impacted third molars (wisdom teeth), assessing mixed dentition in pediatric patients, and screening for large osseous pathologies.
Clinical Safety Notice: Modern digital radiography utilizes highly sensitive sensors that reduce radiation exposure by up to 90% compared to traditional film. However, clinicians strictly adhere to the ALARA (As Low As Reasonably Achievable) principle. Radiographs are never taken as a “routine” mandate; they are prescribed based on an individualized clinical risk assessment. Pregnant patients should inform their dentist, as elective radiographs are typically deferred until after delivery, despite the minimal risk.
In complex cases, such as planning for dental implants or evaluating severe maxillofacial trauma, a Cone Beam Computed Tomography (CBCT) scan may be necessary. Unlike 2D radiographs, CBCT provides a three-dimensional volumetric reconstruction of the anatomical structures, offering unparalleled diagnostic precision. When discussing restorative options, such as comparing Enamel vs Porcelain restorations, accurate radiographic assessment ensures that the underlying tooth structure is sound enough to support the chosen prosthetic.
Frequency of Visits: Tailoring the Recall Schedule
While a six-month interval is standard for healthy individuals, recall frequencies must be customized based on individual caries risk, periodontal status, and systemic health factors.
The traditional recommendation of visiting a check up and clean dentist every six months is a widely accepted baseline, but it is not a universally applicable rule. Modern evidence-based dentistry emphasizes personalized medicine, meaning that the recall interval (the time between routine appointments) must be tailored to the individual patient’s specific clinical risk profile [4]. This risk assessment takes into account a multitude of factors, including oral hygiene efficacy, diet, salivary flow rate, history of dental disease, and systemic health conditions.
For a healthy adult with excellent home care, no active carious lesions, and probing depths consistently between 1-3mm with no bleeding, a six-month recall is generally sufficient to maintain oral health. During these visits, the clinician monitors for any subtle changes and removes the minor calculus deposits that inevitably form even with diligent brushing and flossing. In some exceptionally low-risk cases, the interval may even be extended to 9 or 12 months, though this requires careful clinical judgment.
Conversely, patients categorized as high-risk require more frequent interventions. Individuals with active periodontal disease, or those undergoing Supportive Periodontal Therapy (SPT) after deep cleaning, typically require a 3-to-4-month recall schedule. The rationale for this shorter interval is based on the repopulation kinetics of periodontal pathogens. Clinical studies demonstrate that pathogenic bacteria can recolonize the periodontal pocket and initiate the inflammatory cascade within 9 to 12 weeks following professional debridement. By intervening every 3 to 4 months, the clinician disrupts this biofilm before it can cause further attachment loss.
Clinical Case Review: A 45-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City with generalized moderate periodontitis (probing depths of 5-6mm and heavy subgingival calculus). Following initial non-surgical periodontal therapy (scaling and root planing), the patient was placed on a strict 3-month recall schedule. Over the course of 18 months, the frequent professional debridement, combined with improved home care, resulted in a reduction of probing depths to a stable 3-4mm. The patient was subsequently transitioned to a standard 6-month maintenance schedule, demonstrating the efficacy of customized recall intervals.
Other patient populations also benefit from customized recall schedules. Patients undergoing active orthodontic treatment (especially with fixed brackets) face significant challenges in maintaining oral hygiene, leading to a higher risk of decalcification (white spot lesions) and gingival hyperplasia. These patients often require quarterly cleanings. Similarly, patients with extensive restorative work, dental implants, or systemic conditions like diabetes should be monitored more closely. For expats and locals seeking reliable care, finding the Best Dental Clinic District 1 Saigon ensures access to clinicians who prioritize individualized risk assessment over one-size-fits-all scheduling.
When to See a Doctor: Urgent Clinical Indicators
While routine visits to a check up and clean dentist are designed to be preventive, certain clinical signs and symptoms necessitate immediate professional evaluation outside of the standard recall schedule. Ignoring these warning signs can lead to the rapid progression of dental disease, resulting in severe pain, systemic infection, or the irreversible loss of a tooth.
Patients should seek prompt clinical attention if they experience spontaneous, unprovoked dental pain, particularly if the pain awakens them from sleep or lingers long after exposure to hot or cold stimuli. This type of pain is a classic indicator of irreversible pulpitis, meaning the nerve tissue inside the tooth is actively inflamed or necrotic, often requiring endodontic therapy (root canal) or extraction. Similarly, localized swelling of the gingiva, face, or neck is a critical red flag. Swelling, especially when accompanied by a fever or difficulty swallowing (dysphagia), indicates an active, spreading bacterial infection (abscess) that requires immediate drainage and antibiotic management.
Unprovoked or profuse bleeding from the gums, beyond the minor bleeding occasionally seen during vigorous flossing, should also be evaluated. This can be a sign of acute periodontal conditions, such as Necrotizing Ulcerative Gingivitis (NUG), or it may indicate an underlying systemic hematological issue. Furthermore, any traumatic injury to the dentition—such as a fractured tooth, a tooth that has been luxated (moved out of position), or an avulsed (knocked-out) tooth—requires emergency intervention. Time is of the essence in dental trauma; for instance, an avulsed permanent tooth has the highest chance of successful reimplantation if it is repositioned within 30 to 60 minutes of the injury. For a comprehensive understanding of how to handle such situations, patients should refer to guidelines on Common Dental Emergencies.
Finally, any persistent lesion, ulcer, or lump in the oral cavity that does not resolve within two weeks must be examined by a dentist or oral surgeon. While most oral lesions are benign (such as aphthous ulcers or traumatic fibromas), the possibility of oral squamous cell carcinoma must be definitively ruled out through clinical examination and, if necessary, histopathological biopsy [5].

Maintaining optimal oral health is a lifelong commitment that requires a partnership between the patient and their dental care team. Whether you are seeking a routine prophylaxis, exploring aesthetic improvements, or considering options like How to Fix My Teeth Without Braces, a comprehensive examination is always the first step. By adhering to a customized recall schedule and prioritizing professional cleanings, patients can ensure the longevity of their natural dentition and support their overall systemic well-being. For those residing in or visiting Vietnam, establishing a relationship with a trusted provider, such as the Best Dental Clinic Thao Dien District 2, guarantees access to high-quality, evidence-based preventive care.
Frequently Asked Questions
Does a professional dental cleaning damage tooth enamel?
No, a professional dental cleaning performed by a qualified clinician does not damage tooth enamel. Dental professionals use specialized ultrasonic scalers and hand instruments designed specifically to remove calcified plaque (calculus) without harming the underlying healthy tooth structure. The coronal polishing phase utilizes a mildly abrasive prophylaxis paste that smooths the enamel surface, making it more resistant to future bacterial adhesion. When performed at appropriate intervals, professional scaling is a safe and essential procedure for maintaining optimal oral health.
How long does a comprehensive check-up and clean take?
A standard comprehensive check-up and clean typically requires between 45 to 60 minutes for an adult patient. This timeframe allows the clinician to conduct a thorough medical history review, perform extraoral and intraoral examinations, complete periodontal probing, take necessary radiographs, and execute the scaling and polishing procedures. Patients with extensive calculus buildup, active periodontal disease, or complex medical histories may require longer appointments or multiple visits to achieve optimal clinical outcomes.
Why do my gums bleed during a dental cleaning?
Gingival bleeding during a dental cleaning is primarily an indicator of underlying inflammation, commonly known as gingivitis or periodontitis. When bacterial biofilm accumulates along the gumline, it triggers an immune response, causing the gingival tissues to become engorged with blood vessels and highly friable. As the clinician instruments the area to remove the irritants (plaque and calculus), these fragile tissues bleed easily. As oral hygiene improves and inflammation subsides, bleeding during subsequent cleanings typically diminishes significantly.
Can a routine check-up detect oral cancer?
Yes, a comprehensive dental check-up includes a dedicated oral cancer screening as a standard component of the clinical examination. The dentist visually inspects and physically palpates the soft tissues of the oral cavity, including the tongue, floor of the mouth, palate, and buccal mucosa, looking for abnormal lesions, ulcerations, or indurations. Early detection of precancerous or cancerous changes significantly improves the prognosis, making routine dental visits a critical aspect of overall systemic health monitoring.
Is it necessary to have X-rays at every dental check-up?
No, dental radiographs are not strictly required at every single check-up; their frequency is determined by an individualized clinical risk assessment. Clinicians follow the ALARA (As Low As Reasonably Achievable) principle, prescribing X-rays only when clinically indicated to diagnose interproximal caries, evaluate alveolar bone levels, or investigate specific symptoms. A patient with a high risk of dental caries may require bitewing radiographs more frequently than a patient with excellent oral hygiene and no history of restorative work.
References
- Journal of the American Dental Association. Evidence-based clinical practice guideline on the nonrestorative treatments for carious lesions. (2018).
- Periodontology 2000. The oral microbiome in health and disease. (2020).
- Clinical Oral Investigations. Efficacy of ultrasonic versus hand instrumentation in non-surgical periodontal therapy. (2019).
- Journal of Clinical Periodontology. Supportive periodontal therapy and recall intervals: a systematic review. (2021).
- International Dental Journal. Global guidelines for oral cancer screening in routine dental practice. (2022).



