Bad braces refer to improperly applied orthodontic appliances, unauthorized DIY aligners, or fake fashion braces that apply incorrect biomechanical forces to the teeth. This substandard treatment can lead to severe clinical complications, including irreversible root resorption, periodontal bone loss, and permanent occlusal trauma.
Clinical Summary:
Orthodontic treatment is a complex biomechanical process that requires precise calculation of forces to safely move teeth through alveolar bone. When patients receive “bad braces”—whether through inexperienced providers, direct-to-consumer DIY aligners, or counterfeit cosmetic appliances—the physiological limits of the periodontal ligament are often exceeded. This iatrogenic trauma can result in orthodontically induced inflammatory root resorption (OIIRR), severe gingival recession, alveolar bone dehiscence, and temporomandibular joint (TMJ) dysfunction. Correcting orthodontic damage requires a meticulous, interdisciplinary approach. Specialists must first halt the destructive forces, stabilize the periodontium, and utilize advanced 3D imaging to map a safe retreatment pathway. Patients experiencing excessive tooth mobility, unremitting pain, or bite discrepancies during treatment should seek immediate clinical evaluation to prevent irreversible structural loss.
Key Takeaways:
- Improper orthodontic forces can cause irreversible root shortening (resorption) and permanent bone loss.
- DIY aligners bypass critical clinical diagnostics, significantly increasing the risk of catastrophic tooth mobility.
- Signs of failing treatment include severe, unrelenting pain, rapid gum recession, and worsening bite alignment.
- Retreatment requires a comprehensive 3D CBCT analysis to assess remaining bone volume and root health.
- A mandatory “resting period” is often required before applying new, biologically compatible orthodontic forces.
The Clinical Reality of Bad Braces and Orthodontic Damage
Improperly planned orthodontic treatment applies uncontrolled forces that exceed the physiological tolerance of the periodontal ligament, leading to cellular necrosis rather than healthy bone remodeling.
To understand the profound impact of bad braces, one must first understand the delicate biology of tooth movement. Orthodontics is not merely about pushing teeth into a straight line; it is a highly controlled inflammatory process. When a biologically appropriate force is applied to a tooth, it creates zones of tension and compression within the periodontal ligament (PDL). On the compression side, osteoclasts break down bone, allowing the tooth to move. On the tension side, osteoblasts build new bone to stabilize the tooth in its new position[1]. This synchronized cellular activity requires light, continuous forces and adequate blood supply.
When a patient undergoes poor braces treatment, this delicate biological balance is violently disrupted. Excessive or poorly directed forces crush the blood vessels within the PDL, leading to a condition known as hyalinization—a form of localized sterile necrosis. Because the blood supply is cut off, osteoclasts cannot reach the area to resorb bone normally. Instead, the body must recruit cells from deeper within the bone marrow to clear away the necrotic tissue, a process called undermining resorption. This not only delays tooth movement but also causes severe, unremitting pain and significantly increases the risk of permanent orthodontic damage.

Furthermore, the vectors of force must be meticulously calculated. A common hallmark of substandard orthodontics is the failure to control the root apex. While the visible crown of the tooth may appear to be moving into alignment, the root may be forced against the dense cortical plates of the jawbone. Pushing a tooth root outside the alveolar housing inevitably leads to fenestrations (windows in the bone) or dehiscences (loss of the marginal bone), which manifest clinically as severe gum recession. This type of iatrogenic trauma is frequently seen in cases where expansion is attempted without adequate skeletal support, highlighting the critical need for comprehensive orthodontic care managed by qualified specialists.
Major Complications of Failed Orthodontics
Failed orthodontic interventions frequently result in severe structural damage, including apical root resorption, irreversible gingival recession, and widespread enamel decalcification.
The clinical manifestations of failed braces extend far beyond aesthetic dissatisfaction. When biomechanical principles are ignored, the resulting complications can compromise the long-term survival of the dentition. One of the most severe consequences is Orthodontically Induced Inflammatory Root Resorption (OIIRR). While microscopic root blunting occurs in almost all orthodontic treatments, excessive forces, prolonged treatment times, and heavy continuous mechanics can cause severe, irreversible shortening of the tooth roots[2]. Teeth with severely resorbed roots have a compromised crown-to-root ratio, making them highly susceptible to mobility and premature loss, especially if subjected to secondary occlusal trauma.
Periodontal degradation is another hallmark of poor braces treatment. The periodontium—comprising the gingiva, periodontal ligament, cementum, and alveolar bone—is highly sensitive to bacterial plaque and mechanical stress. Bad braces often feature poorly adapted bands, excess composite resin around brackets, or improper wire ligatures that act as massive plaque retentive factors. If the provider fails to monitor periodontal health during treatment, the patient can rapidly develop aggressive periodontitis. The combination of active inflammation and heavy orthodontic forces accelerates alveolar bone destruction at an alarming rate.
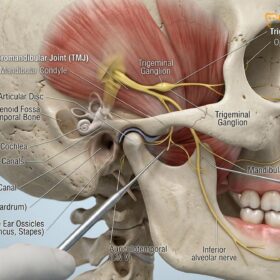
Additionally, improper bite alignment (malocclusion) resulting from failed orthodontics can trigger severe temporomandibular joint (TMJ) disorders. If the teeth are moved into positions that do not harmonize with the patient’s centric relation (the natural resting position of the jaw joints), the masticatory muscles must constantly overcompensate. This muscular hyperactivity often leads to bruxism (teeth grinding), chronic headaches, and morning jaw pain. In such cases, patients may require protective occlusal splints to manage the muscular symptoms before any retreatment can begin.

Enamel decalcification, commonly known as white spot lesions (WSLs), is a frequent aesthetic and structural complication. When brackets are placed poorly or oral hygiene protocols are not strictly enforced by the provider, cariogenic bacteria produce acids that leach calcium and phosphate from the enamel. Upon removal of the failed braces, the patient is left with permanent, chalky white squares on their teeth that may eventually cavitate into active decay.
| Clinical Complication | Primary Cause in Bad Braces | Interceptive Clinical Action |
|---|---|---|
| Apical Root Resorption | Excessive force, prolonged treatment time, jiggling forces. | Immediate cessation of active forces; radiographic monitoring. |
| Alveolar Bone Dehiscence | Expanding dental arches beyond the biological bony envelope. | Periodontal grafting; moving roots back into medullary bone. |
| White Spot Lesions (Decalcification) | Poor bracket adaptation; failure to monitor oral hygiene. | Remineralization therapy (fluoride/CPP-ACP); resin infiltration. |
| Occlusal Trauma / TMJ Pain | Failure to establish a mutually protected occlusal scheme. | Occlusal equilibration; splint therapy; comprehensive retreatment. |
The Dangers of DIY Aligners and Fake Fashion Braces
Direct-to-consumer aligners and cosmetic fake braces bypass essential clinical diagnostics, drastically increasing the risk of irreversible dental trauma and tooth loss.
In recent years, the rise of direct-to-consumer (DTC) clear aligners has introduced a new paradigm of orthodontic damage. The primary danger of these systems lies in the complete absence of comprehensive clinical diagnostics. Standard orthodontic care requires a thorough clinical examination, periodontal probing, and 3D Cone Beam Computed Tomography (CBCT) to assess the underlying bone architecture. DIY aligner companies typically rely solely on patient-taken photographs or basic at-home impression kits, completely ignoring the health of the roots and the surrounding bone[3].
The diy aligner risks are profound. Because the software algorithms design tooth movements based only on the visible crowns, they frequently program expansion or tipping movements that push the roots straight through the buccal or lingual cortical plates. Patients using these systems often report sudden, severe tooth mobility, acute pain, and changes in their bite that make chewing impossible. Furthermore, without a dentist to perform interproximal reduction (IPR) or place composite attachments, the aligners cannot achieve complex movements like root torquing or bodily translation, resulting in teeth that are merely tipped into unstable positions.
Clinical Warning: The use of unauthorized “fashion braces” or fake braces applied by non-professionals in unregulated settings poses a severe risk of acute dental trauma, toxic material exposure, and rapid tooth loss. These appliances utilize non-medical grade metals and toxic glues, and apply entirely random, uncontrolled forces that can extract a tooth from its socket in a matter of weeks.

Fake braces, often marketed as a fashion statement in certain demographics, represent an even more acute danger. These appliances are typically glued on by unlicensed individuals using toxic adhesives. The wires used are not calibrated orthodontic archwires; they are often rigid craft wires that apply massive, uncontrolled forces. This can lead to rapid pulpal necrosis (death of the tooth nerve) and acute periodontal abscesses. The damage inflicted by these counterfeit appliances is often so severe that extraction and prosthetic replacement become the only viable clinical options.
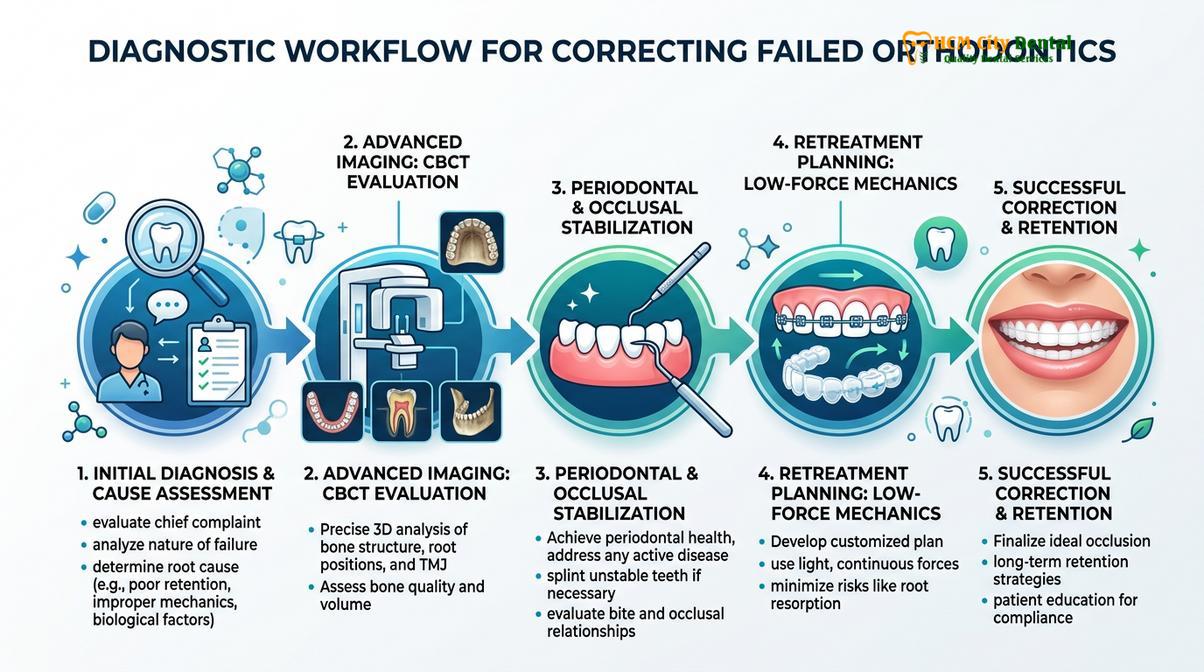
Diagnostic Workflow for Correcting Orthodontic Damage
Correcting previous orthodontic errors requires a comprehensive diagnostic approach utilizing 3D CBCT imaging, periodontal charting, and precise occlusal analysis to establish a safe retreatment baseline.
When a patient presents with complications from poor braces treatment, the immediate clinical objective is not to resume tooth movement, but to halt the damage and establish a precise diagnostic baseline. The retreatment of failed orthodontics is highly complex because the physiological reserve of the periodontium has already been depleted. The teeth have been subjected to trauma, the roots may be shortened, and the bone levels are often compromised.
The first step in the diagnostic workflow is the immediate removal of all active orthodontic forces. Wires are removed, and if clear aligners were used, the patient is instructed to stop wearing them. A comprehensive periodontal examination is then conducted to assess pocket depths, bleeding on probing, and the width of attached gingiva. This is crucial because moving teeth in the presence of active periodontal inflammation will rapidly accelerate bone loss[4].
Advanced imaging is non-negotiable in these scenarios. A 3D Cone Beam Computed Tomography (CBCT) scan is required to visualize the exact position of every tooth root in all three dimensions. The CBCT allows the clinician to measure the remaining bone thickness on the buccal and lingual aspects, assess the severity of root resorption, and identify any fenestrations. At HCMC Dental Clinic in Ho Chi Minh City, this 3D diagnostic approach is standard protocol for all retreatment cases, ensuring that no further harm is done to an already compromised dentition.
“When we evaluate a patient who has suffered from bad braces or DIY aligner complications, our primary focus shifts from aesthetics to biological preservation. We cannot force a tooth into alignment if the foundational bone and root structure have been critically compromised. A mandatory resting period and 3D radiographic mapping are essential before any new forces are applied.”
— Dr. Nguyen Van Cuong, HCMC Dental Clinic
Following the imaging and periodontal assessment, a detailed occlusal analysis is performed. The clinician must determine the discrepancy between the patient’s centric relation (jaw joint position) and maximum intercuspation (how the teeth fit together). Often, failed braces leave the patient with premature contacts—specific teeth that hit too early when closing. These interferences cause functional shifting of the mandible and contribute to the sleep apnea connection and nocturnal bruxism. Diagnostic models are mounted on an articulator to simulate jaw movements and plan the necessary occlusal corrections.
Retreatment Strategies for Poor Braces Treatment
Rehabilitating a compromised smile involves stabilizing periodontal health first, followed by the application of low-friction, biologically compatible orthodontic forces to safely correct the malocclusion.
The retreatment of orthodontic damage requires a highly customized, biologically respectful approach. Once the diagnostic phase is complete and any active periodontal disease has been controlled, the clinician must design a biomechanical plan that utilizes the lightest possible forces. The goal is to achieve the necessary corrections while minimizing any further stress on the shortened roots and thinned alveolar bone.
In many cases, a “resting period” of 3 to 6 months is prescribed before initiating retreatment. This allows the periodontal ligament to heal, localized inflammation to subside, and the mobility of the teeth to decrease. During this phase, patients may be provided with passive retainers or custom mouth guards to stabilize the teeth and protect them from occlusal trauma, especially if the patient exhibits signs of bruxism.
Clinical Case Study: Correcting DIY Aligner Trauma
A 28-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City with severe anterior tooth mobility and an open bite after 8 months of using a mail-order DIY aligner system. CBCT imaging revealed that the lower incisor roots had been pushed through the labial cortical plate, resulting in severe dehiscence and grade II mobility.
Intervention: All aligner use was immediately halted. The patient underwent a 4-month resting phase with a passive splint. Periodontal evaluation confirmed the need for a connective tissue graft to reinforce the thin gingival biotype. Following tissue maturation, Dr. Nguyen Van Cuong initiated a highly controlled retreatment using a customized clear aligner system with specific root-torquing attachments to slowly move the roots back into the medullary bone housing. After 14 months of low-force mechanics, the bite was stabilized, mobility was resolved, and the patient was transitioned to a strict retention protocol, including guidance on proper appliance hygiene to maintain long-term health.
When active retreatment begins, the choice of appliance is critical. Traditional heavy stainless steel wires are often contraindicated. Instead, clinicians may utilize thermally activated Nickel-Titanium (NiTi) wires that deliver continuous, ultra-light forces. Alternatively, custom-prescribed clear aligner therapy (managed by a specialist, not DIY) can be highly effective, as the software allows the doctor to limit the amount of movement per stage (e.g., 0.15mm instead of the standard 0.25mm) to protect compromised roots[5].
Anchorage control is another major challenge in retreatment. Because the teeth are already compromised, they cannot be used to pull against each other without risking further damage. In these scenarios, Temporary Anchorage Devices (TADs)—small titanium mini-screws placed temporarily into the jawbone—are frequently utilized. TADs provide absolute anchorage, allowing the clinician to move specific teeth without placing reactive forces on the vulnerable adjacent teeth.
When to See a Doctor for Orthodontic Complications
Recognizing the early warning signs of failing orthodontic treatment can mean the difference between a simple course correction and irreversible tooth loss. Patients currently undergoing treatment—whether with traditional brackets or clear aligners—must remain vigilant about their oral health and the physical sensations they experience.
You should seek an immediate clinical evaluation if you experience any of the following symptoms: severe, throbbing pain that does not subside within a few days of an adjustment; visible recession of the gums where the root surface becomes exposed; extreme tooth mobility where the tooth feels loose in its socket; or a sudden, drastic change in your bite that makes chewing difficult or painful. Additionally, if you notice chalky white spots developing around your brackets that cannot be brushed away, this indicates active enamel decalcification that requires immediate intervention.
“Patients must understand that mild discomfort after an adjustment is normal, but acute, localized pain or teeth that feel excessively loose are massive red flags. Never ignore these symptoms, and never attempt to adjust your own appliances. Early intervention is the only way to prevent permanent structural damage.”
— Dr. Nguyen Van Cuong, HCMC Dental Clinic

For individuals who have recently completed treatment but are unhappy with the results, or those who suspect they have suffered orthodontic damage from DIY aligners, scheduling a comprehensive diagnostic consultation is imperative. At HCMC Dental Clinic, our specialists utilize advanced 3D imaging to assess the hidden health of your roots and bone, providing a clear, evidence-based pathway to restore both function and aesthetics. If you are an expatriate or frequent traveler dealing with appliance issues, we also provide comprehensive guidance on managing dental appliances while traveling to ensure your treatment remains stable.
Frequently Asked Questions
What are the first signs that my braces treatment is failing?
The earliest signs of failing orthodontic treatment include excessive tooth mobility, severe localized pain that does not subside, and unexpected shifting of your bite. If you notice your gums receding rapidly or teeth feeling unusually loose beyond normal orthodontic adjustment periods, immediate clinical evaluation is necessary. Prolonged ignoring of these symptoms can lead to irreversible periodontal damage or root resorption.
Can root resorption caused by bad braces be reversed?
No, orthodontically induced inflammatory root resorption (OIIRR) is a permanent loss of root structure and cannot be biologically reversed. However, once the excessive orthodontic forces are removed, the active resorption process typically halts. A specialist can then stabilize the affected teeth, monitor them radiographically, and design a safe, low-force retreatment plan to prevent further structural degradation.
Why are DIY clear aligners considered dangerous by orthodontists?
DIY aligners are considered highly dangerous because they completely bypass essential clinical diagnostics, such as CBCT scans and periodontal probing, which are required to assess bone health. Moving teeth without understanding the underlying bone architecture can push roots outside the alveolar housing, leading to severe mobility, bite misalignment, and ultimately, catastrophic tooth loss.
How long should I wait to fix orthodontic damage from a previous provider?
You should seek a diagnostic consultation immediately upon suspecting orthodontic damage, though active retreatment may require a resting period of several months. This resting phase allows the periodontal ligament to heal and localized inflammation to subside. Your new orthodontist will determine the exact timeline based on 3D imaging and the severity of the iatrogenic trauma.
Will I need surgery to correct complications from poor braces treatment?
Surgery is not always required, but severe cases of poor braces treatment may necessitate adjunctive surgical procedures. If teeth have been pushed out of the bone, periodontal grafting may be needed to restore lost tissue. In cases of severe skeletal discrepancy exacerbated by bad orthodontics, orthognathic surgery might be recommended to properly align the jaws and stabilize the bite.
References
- American Journal of Orthodontics and Dentofacial Orthopedics. Orthodontically induced inflammatory root resorption: Clinical and histological perspectives. (2021).
- Journal of Clinical Periodontology. Periodontal complications of orthodontic treatment: A comprehensive review. (2020).
- European Journal of Orthodontics. The biomechanical impact of direct-to-consumer clear aligners on the periodontium. (2022).
- Angle Orthodontist. Iatrogenic effects of excessive orthodontic forces on alveolar bone remodeling. (2019).
- International Journal of Dentistry. Interdisciplinary management of failed orthodontic cases: Restorative and periodontal considerations. (2023).