

Lip protrusion after braces is a common, often temporary condition caused by the physical bulk of orthodontic brackets and the initial forward movement of teeth during the leveling and aligning phase. As treatment progresses and spaces close, the lips typically relax into a natural, balanced profile.
Clinical Summary:
The phenomenon of lip protrusion during orthodontic treatment is a well-documented clinical occurrence primarily driven by two factors: the physical thickness of the appliance (brackets and wires) and the biomechanical flaring of incisors during the initial resolution of dental crowding. When teeth are aligned within a restricted arch perimeter without immediate space creation, the anterior segment naturally tips forward, pushing the overlying soft tissue outward. This effect is generally transient. Advanced orthodontic workflows, including the use of Temporary Anchorage Devices (TADs), strategic extractions, and Interproximal Reduction (IPR), are employed to retract the anterior teeth during the space closure phase, ultimately flattening the profile. Furthermore, the choice of appliance—such as clear aligners versus traditional labial braces—significantly influences the degree of temporary soft tissue displacement. A comprehensive cephalometric analysis is essential to differentiate between transient appliance-induced protrusion and underlying skeletal discrepancies, ensuring that the final treatment outcome achieves optimal facial harmony and functional occlusion.
Key Takeaways:
- Initial lip fullness is frequently caused by the physical thickness of brackets resting against the inner mucosa.
- Resolving severe crowding often results in temporary incisor flaring, which pushes the lips forward until retraction begins.
- Orthodontists utilize space-gaining techniques like extractions or IPR to pull teeth back and flatten the facial profile.
- Clear aligner therapy eliminates the labial bulk of traditional brackets, minimizing temporary soft tissue protrusion.
- Final facial aesthetics depend heavily on individual soft tissue thickness, jaw relationship, and precise biomechanical control.
The Biomechanics of Lip Protrusion During Orthodontic Treatment
Initial orthodontic alignment utilizes flexible archwires to unravel crowded teeth, which can temporarily push the incisors and overlying lips forward if space is limited.
To understand why the lips may appear more prominent after the placement of orthodontic appliances, it is essential to examine the biomechanics of the initial treatment phase. Orthodontic treatment is broadly divided into several stages, the first of which is “leveling and aligning.” During this phase, the primary objective is to correct vertical discrepancies and unravel crowded or rotated teeth to create a continuous, smooth dental arch. [1]
When a patient presents with dental crowding, it means the total width of their teeth exceeds the available perimeter of their jawbone. To align these teeth, the orthodontist engages highly flexible, shape-memory archwires (often made of Nickel-Titanium) into the brackets. As these wires attempt to return to their original U-shape, they exert continuous, light forces on the teeth. If no space has been created through extractions or enamel reduction, the only way for the crowded teeth to align is by expanding the arch outward. This outward expansion predominantly affects the anterior teeth (incisors), causing them to tip or “flare” forward. [2]
This forward tipping of the incisors directly impacts the overlying soft tissue. The lips rest directly against the labial surfaces of the anterior teeth; therefore, any forward movement of the dentition translates to a forward projection of the lips. This is a well-documented biomechanical consequence often referred to clinically as “round-tripping,” where teeth are temporarily moved into a more protrusive position before being retracted later in treatment.

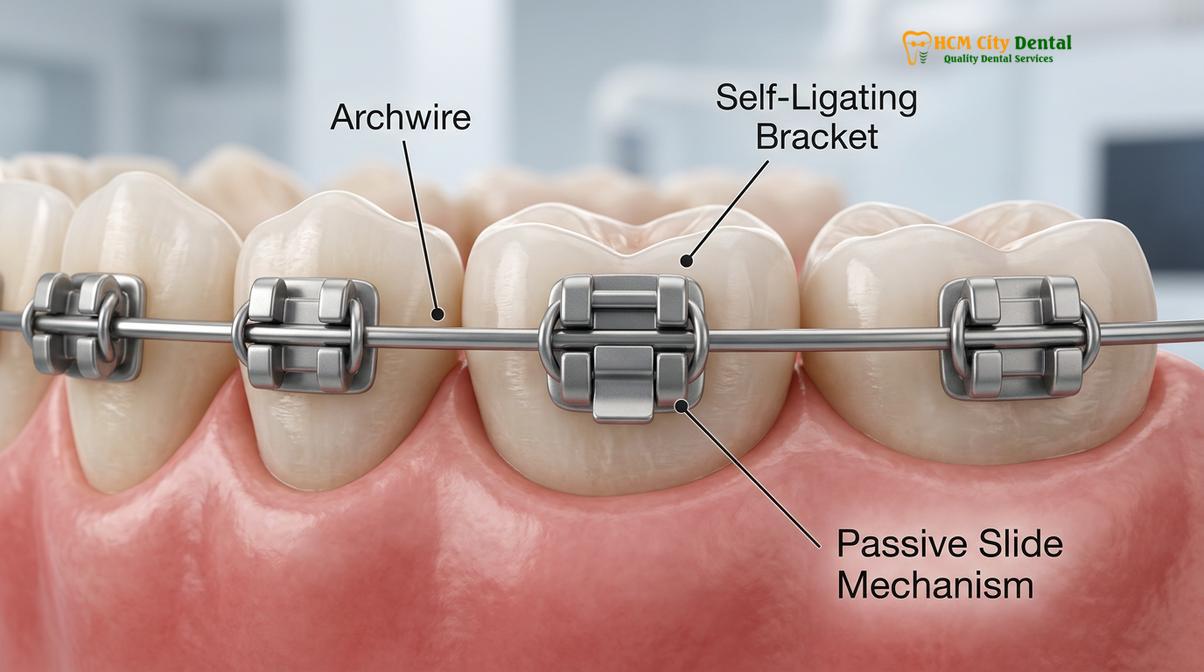
Furthermore, the physical presence of the orthodontic hardware itself contributes significantly to perceived lip protrusion. Traditional metal or ceramic brackets have a specific thickness—usually ranging from 1.5 to 2.5 millimeters. When these brackets are bonded to the labial (front) surfaces of the teeth, they instantly add bulk between the teeth and the inner mucosa of the lips. [3] This sudden addition of volume forces the lips to stretch and drape over the hardware, creating an immediate, albeit artificial, fullness. Patients often notice this the very day their braces are placed, long before any actual tooth movement has occurred.
“The soft tissue drape is highly sensitive to underlying hard tissue changes. During the initial stages of orthodontics, the combination of bracket thickness and necessary incisor flaring creates a temporary fullness that is a normal part of the biomechanical journey toward a balanced occlusion.”
Dr. Nguyen Van Cuong frequently educates patients on this phenomenon during their initial consultations. By setting realistic expectations regarding the temporary changes in facial profile, patients are better prepared for the transitional phases of their comprehensive orthodontic care. Understanding that this initial protrusion is a mechanical necessity for unraveling severe crowding helps alleviate anxiety during the first few months of treatment.
Temporary vs. Permanent Profile Changes
Most lip fullness experienced early in treatment is a transient effect of bracket bulk and initial alignment, resolving completely once the retraction and space closure phases commence.
A critical distinction must be made between transient lip protrusion caused by the active mechanics of early treatment and permanent profile changes resulting from the final positioning of the teeth and jaws. For the vast majority of patients, the lip protrusion experienced after getting braces is strictly temporary. [4]
As discussed, the initial bulk of the brackets and the flaring of the incisors create a temporary outward displacement of the soft tissue. However, orthodontic treatment is a dynamic process. Once the teeth are leveled and aligned, the orthodontist transitions to stiffer, rectangular archwires (such as stainless steel or TMA). These wires allow for precise control over the torque (the root-to-crown inclination) of the teeth. It is during this subsequent phase—often involving space closure and retraction—that the temporary protrusion is addressed.
If the treatment plan involves pulling the front teeth backward (retraction), the lips will naturally follow the new, more posterior position of the incisors. As the teeth move back, the tension on the lips decreases, allowing them to relax and flatten. [5] Additionally, once the active treatment is complete and the braces are physically removed from the teeth, the 1.5 to 2.5 millimeters of artificial bulk is instantly eliminated. Patients frequently report that their lips feel significantly thinner and more relaxed immediately following the debonding appointment.
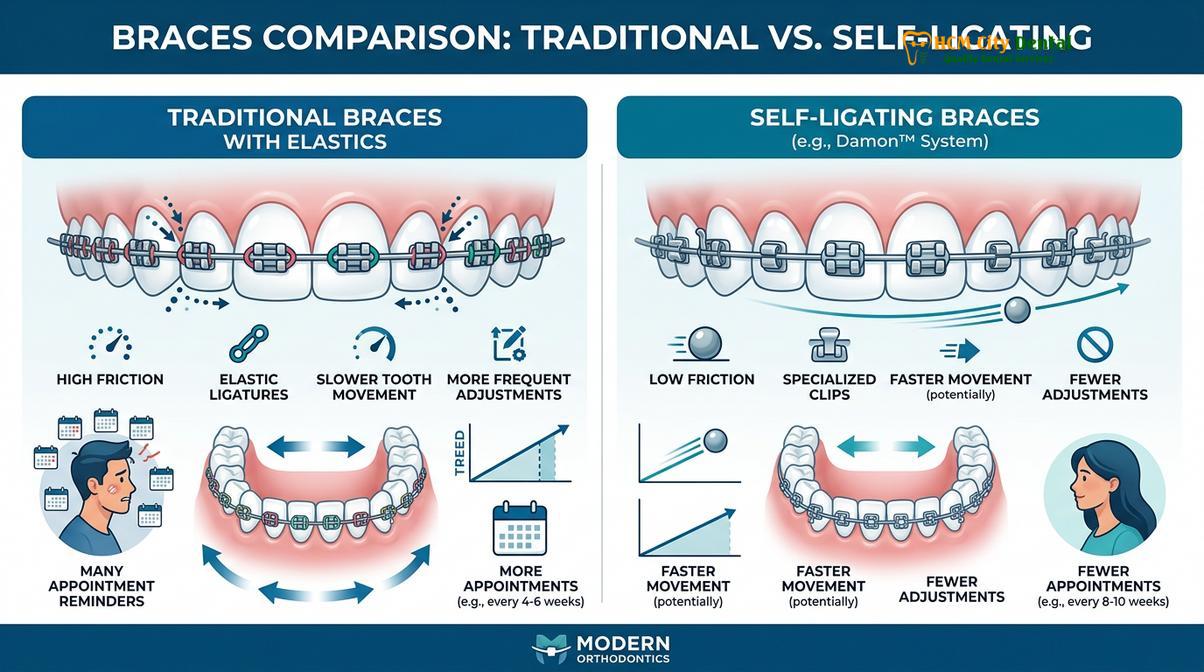
Modern orthodontic technologies also play a role in managing this temporary phase. The use of heat activated braces and advanced archwire alloys allows for more gentle, controlled expansion, potentially minimizing the severity of the initial flaring. Similarly, self ligating braces, which do not require elastic ties to hold the wire in place, often have a slightly lower profile and generate less friction, which can influence how the arch expands and how the soft tissue responds during the early months of treatment.
However, it is important to note that in some specific clinical scenarios, a slight increase in lip fullness may be a planned, permanent outcome. For patients who present with a “dished-in” profile, severely retruded incisors, or very thin lips, the orthodontist may intentionally design the treatment to advance the anterior teeth. In these cases, the resulting lip support is a desired aesthetic enhancement, contributing to a more youthful and balanced facial appearance. The key is precise cephalometric diagnosis and individualized treatment planning.
Clinical Workflows to Manage and Correct Protrusion
Orthodontists employ specific space-gaining strategies, such as extractions, interproximal reduction, and skeletal anchorage, to effectively retract protruding teeth and flatten the facial profile.
When a patient presents with genuine bimaxillary protrusion (where both the upper and lower front teeth are angled excessively forward) or when severe crowding necessitates significant space creation, the orthodontist must employ specific clinical workflows to manage the profile. The goal is to create enough space within the dental arch to retract the anterior teeth, thereby reducing the strain on the lips and improving the nasolabial angle.
One of the most common and effective methods for resolving severe protrusion is the extraction of premolars. By removing one premolar in each quadrant (usually the first premolars), the orthodontist gains approximately 7 to 8 millimeters of space on each side of the arch. [1] Once the initial leveling and aligning are complete, the anterior teeth are systematically pulled backward into these extraction spaces. As the incisors move posteriorly, the overlying lips lose their excessive support and naturally fall back into a more relaxed, harmonious position.
In cases where the protrusion or crowding is mild to moderate, a non-extraction approach may be preferred. In these scenarios, Interproximal Reduction (IPR) is a highly effective technique. IPR involves carefully polishing away a microscopic amount of enamel (usually 0.2 to 0.5 millimeters) from the sides of adjacent teeth. When performed across several teeth, this can generate several millimeters of space, allowing the orthodontist to retract the flared incisors without the need for extractions. [2]
Clinical Case Study: Managing Bimaxillary Protrusion
A 24-year-old patient visited HCMC Dental Clinic in Ho Chi Minh City expressing concern about lip incompetence (inability to close lips naturally) and a protrusive facial profile. Clinical and cephalometric evaluation by Dr. Nguyen Van Cuong revealed severe bimaxillary dental protrusion with minimal crowding. The treatment plan involved the extraction of four first premolars. Utilizing maximum anchorage protocols with Temporary Anchorage Devices (TADs), the anterior segments were retracted by 6mm over 18 months. Post-treatment records demonstrated a significantly relaxed lip posture, a normalized nasolabial angle, and complete resolution of lip strain, highlighting the profound impact of controlled anterior retraction on soft tissue aesthetics.
To achieve maximum retraction of the front teeth without allowing the back teeth (molars) to drift forward into the extraction spaces, orthodontists increasingly rely on Temporary Anchorage Devices (TADs). TADs are miniature titanium screws temporarily placed into the jawbone. They serve as an immovable anchor point from which forces can be applied to pull the front teeth back. [3] By utilizing TADs, the clinician ensures that 100% of the extraction space is used for reducing the lip protrusion, resulting in a more dramatic and predictable improvement in the facial profile.
Additionally, specific mechanics such as the use of damon braces elastics or specialized retraction loops in the archwire are employed to control the tipping and torque of the teeth as they move backward. Proper torque control is vital; if the crowns of the teeth are tipped back without moving the roots, the aesthetic outcome will be compromised. The roots must be moved through the alveolar bone to ensure long-term stability and optimal soft tissue support.
How Different Orthodontic Appliances Affect Lip Posture
The physical design and placement of orthodontic appliances—ranging from bulky traditional brackets to smooth clear aligners—directly dictate the degree of temporary soft tissue displacement.
The type of orthodontic appliance selected for treatment plays a substantial role in how the lips adapt and whether temporary protrusion becomes a noticeable concern for the patient. Not all appliances interact with the soft tissue in the same manner, and understanding these differences is crucial for patients prioritizing facial aesthetics during their treatment journey.
Traditional metal braces are the most common and robust appliances used in orthodontics. However, they also possess the highest profile, meaning they protrude the furthest from the tooth surface. This inherent bulk inevitably pushes the lips outward. Ceramic braces, while offering a more discreet appearance due to their tooth-colored material, are often slightly thicker than their metal counterparts to ensure structural integrity, potentially causing a similar or slightly greater degree of temporary lip fullness. [4]
For patients highly concerned about lip protrusion during treatment, clear aligner therapy represents a paradigm shift in soft tissue management. Clear aligners are fabricated from thin, medical-grade thermoplastic (typically around 0.76 millimeters thick). Because they encapsulate the teeth smoothly without any protruding labial brackets or sharp tie-wings, they cause minimal disruption to the resting posture of the lips. The soft tissue can drape naturally over the aligners, virtually eliminating the artificial “bumpy” protrusion associated with fixed braces.

Another alternative is lingual orthodontics, where the brackets are custom-fitted to the lingual (tongue-facing) surfaces of the teeth. Because the labial surfaces remain completely bare, lingual braces cause zero outward displacement of the lips. However, they do encroach upon the tongue space, which can temporarily affect speech and swallowing. [5]
When correcting specific bite discrepancies, the mechanics of the appliance also influence lip posture. For instance, when utilizing class 3 braces mechanics to correct an underbite, elastics are often worn from the lower front teeth to the upper back teeth. This force vector can temporarily alter the posture of the lower lip as the lower jaw is guided backward and the upper jaw is encouraged forward.
| Appliance Type | Labial Bulk (Thickness) | Impact on Lip Protrusion | Soft Tissue Comfort |
|---|---|---|---|
| Traditional Metal Braces | High (1.5mm – 2.0mm) | Noticeable temporary outward displacement of lips. | Moderate; requires adaptation period for inner mucosa. |
| Ceramic Braces | High (1.8mm – 2.5mm) | Noticeable temporary outward displacement; slightly bulkier than metal. | Moderate; smooth contours but higher profile. |
| Lingual Braces | None (Labially) | Zero impact on lip protrusion; brackets are behind teeth. | Low initially; requires significant tongue adaptation. |
| Clear Aligners | Very Low (~0.76mm) | Minimal to no noticeable lip protrusion; smooth drape. | High; smooth plastic prevents mucosal irritation. |
Choosing the right appliance involves balancing biomechanical needs with aesthetic desires. Patients undergoing orthodontic treatment in Vietnam often consult with specialists to determine which system aligns best with their lifestyle and aesthetic tolerances. Regardless of the appliance chosen, maintaining excellent oral hygiene is paramount, as inflamed, swollen gums can further exacerbate the appearance of a protrusive mouth. Patients must be diligent in maintaining hygiene around brackets to prevent gingival hypertrophy.
The Role of Soft Tissue and Facial Anatomy
Individual anatomical factors, such as lip thickness, jaw relationship, and the nasolabial angle, heavily influence how noticeably the lips respond to underlying dental movements.
Orthodontics is no longer solely about straightening teeth; it is deeply rooted in the “soft tissue paradigm.” This modern approach dictates that the final position of the teeth must be determined by the desired aesthetic outcome of the overlying soft tissues—the lips, cheeks, and chin. [1] How a patient’s lips respond to braces is highly dependent on their unique facial anatomy.
One of the primary cephalometric measurements used by orthodontists is the Ricketts E-line (Esthetic line), which is drawn from the tip of the nose to the soft tissue prominence of the chin. In a harmoniously balanced profile, the upper and lower lips should rest slightly behind or just touching this line. If a patient naturally has a retruded chin (micrognathia) or a very prominent nose, their lips may appear protrusive relative to the E-line, even if their teeth are perfectly positioned. [2]
Lip thickness also plays a crucial role. Patients with naturally thick, fleshy lips will exhibit less noticeable changes in their profile when the teeth are moved backward or forward. The thick tissue acts as a buffer, absorbing the underlying hard tissue changes. Conversely, patients with very thin, taut lips will show a 1:1 ratio of tooth movement to lip movement; even a millimeter of incisor retraction will result in a visible flattening of the lip profile. [3]
“The ultimate goal of modern orthodontics is not merely a Class I occlusion, but the achievement of facial harmony. We must meticulously evaluate the nasolabial angle, the mentolabial sulcus, and the resting lip posture before initiating any biomechanical movements that could alter the patient’s profile.”
Furthermore, the nasolabial angle—the angle formed between the base of the nose and the upper lip—is a critical aesthetic marker. A sharp, acute angle often indicates flared upper incisors and a protrusive upper lip. Retracting the upper teeth opens this angle, creating a softer, more aesthetically pleasing transition from the nose to the mouth. Providing elegant dental care requires the clinician to view the face as a whole, ensuring that dental corrections enhance, rather than detract from, the patient’s natural beauty.
For patients concerned about the financial investment required for comprehensive profile correction, exploring financing options for orthodontic care can make advanced treatments, such as clear aligners or TAD-assisted retraction, more accessible. Once the structural alignment is complete and the braces are removed, many patients further enhance their new, balanced smiles with post-orthodontic aesthetic enhancements like professional whitening.
When to See an Orthodontist
While temporary lip fullness is a standard part of the orthodontic process, certain soft tissue responses warrant professional evaluation. It is crucial to differentiate between normal appliance bulk and functional issues that could compromise treatment outcomes or patient comfort.
Important Clinical Considerations
You should schedule an evaluation with your orthodontist if you experience any of the following symptoms during your treatment:
- Severe Lip Incompetence: An inability to close your lips together at rest without excessive muscle strain or chin dimpling (mentalis strain).
- Chronic Mouth Breathing: If the protrusion forces you to breathe primarily through your mouth, which can lead to dry mouth, gingival inflammation, and altered facial growth in adolescents.
- Traumatic Ulcerations: Deep, non-healing sores on the inner lips caused by excessive pressure from the brackets.
- Unexpected Profile Worsening: If you are in the later stages of treatment (space closure phase) and your profile continues to become more protrusive rather than flattening out.
If you are experiencing significant discomfort or are concerned about the trajectory of your facial profile, a comprehensive reassessment is necessary. At HCMC Dental Clinic in Ho Chi Minh City, the clinical team utilizes advanced 3D cephalometric imaging to monitor tooth movement and soft tissue changes continuously. This ensures that the biomechanical forces applied are yielding the desired aesthetic and functional results. Always consult directly with a certified orthodontic specialist for personalized diagnostic advice rather than relying solely on general educational references.

Frequently Asked Questions
Is lip protrusion normal during the first few months of braces?
Yes, temporary lip protrusion is a normal clinical occurrence during the initial leveling and aligning phase of orthodontic treatment. As flexible archwires resolve dental crowding, the front teeth may temporarily flare forward before space closure and retraction protocols pull them back into their final, balanced positions. Additionally, the physical thickness of the brackets themselves adds immediate bulk under the lips.
How long does it take for my lips to look normal again?
Most patients notice their lip profile returning to normal within six to nine months, typically after the extraction spaces are closed or the retraction phase begins. The exact timeline depends on your specific malocclusion, the biomechanics utilized, and whether space-gaining procedures like extractions or interproximal reduction were performed to allow for anterior retraction.
Do clear aligners cause the same lip protrusion as metal braces?
Clear aligners generally cause significantly less lip protrusion than traditional metal brackets because they lack the physical bulk of labial hardware. The smooth, thin plastic encapsulates the teeth, allowing the lips to rest more naturally against the dental arch without the added thickness of brackets and wires, making them a preferred choice for aesthetically conscious patients.
Can orthodontics fix lips that naturally stick out?
Yes, orthodontic treatment can effectively reduce natural lip protrusion if the underlying cause is dental, such as flared incisors or bimaxillary protrusion. By utilizing extractions or temporary anchorage devices (TADs) to retract the anterior teeth, the overlying soft tissues of the lips will naturally follow, flattening the facial profile and improving the nasolabial angle.
Will my lips look thinner after my braces are removed?
Your lips may appear slightly less full after braces removal simply because the physical bulk of the brackets is no longer pushing them outward. However, the actual anatomical thickness of your lip tissue remains unchanged; the perceived difference is solely due to the altered resting posture over the newly aligned, smooth dental arch.
References
- American Journal of Orthodontics and Dentofacial Orthopedics. Soft tissue profile changes following orthodontic extraction treatment. (2021).
- Journal of Clinical Orthodontics. Biomechanics of anterior retraction and anchorage control using TADs. (2020).
- European Journal of Orthodontics. The effect of bracket thickness on perceived lip protrusion during initial alignment. (2019).
- Angle Orthodontist. Cephalometric evaluation of incisor flaring during non-extraction leveling and aligning. (2022).
- International Journal of Dentistry. Patient perceptions of facial aesthetics and lip posture during clear aligner therapy. (2018).



