Does it hurt to get braces? The application process itself is completely painless, as no needles or drilling are involved. However, patients typically experience mild to moderate soreness and pressure starting a few hours after placement, lasting for three to five days as teeth begin to shift.
Clinical Summary:
Orthodontic treatment involves applying controlled biomechanical forces to reposition teeth, which naturally induces a temporary inflammatory response in the periodontal tissues. While the physical bonding of brackets and wires is entirely painless, the subsequent cellular activity—specifically bone remodeling—results in a dull ache or pressure that peaks within 24 to 72 hours. This discomfort is a normal indicator that the treatment is working. Modern orthodontics utilizes heat-activated nickel-titanium wires and advanced self-ligating brackets to deliver lighter, more continuous forces, significantly reducing overall pain compared to historical methods. Effective pain management relies on a combination of soft diets, orthodontic wax for mucosal protection, and appropriate analgesics that do not inhibit necessary bone metabolism.
Key Takeaways:
- The actual procedure of attaching braces to your teeth involves no pain, injections, or drilling.
- Soreness typically begins 4 to 6 hours after the appointment and peaks between days two and three.
- Discomfort is caused by the stretching of the periodontal ligament and localized changes in blood flow.
- Soft tissue irritation (cheeks and lips) is common initially but resolves as the mouth adapts.
- Over-the-counter pain relievers and orthodontic wax are highly effective for managing early treatment symptoms.
The Clinical Reality: Does Getting Braces Hurt?
Getting braces applied does not hurt, but the subsequent biological response to orthodontic forces causes temporary soreness as the periodontal ligaments stretch and bone remodeling begins.
One of the most common anxieties for patients considering Orthodontics is the anticipation of pain. To accurately answer the question of whether does getting braces hurt, it is essential to separate the physical appointment from the biological response that follows. The clinical procedure of placing fixed orthodontic appliances is non-invasive. It requires no local anesthesia, no drilling of the tooth structure, and no surgical intervention.
The Bonding Appointment: A Step-by-Step Look
Understanding the workflow of the bonding appointment can significantly alleviate pre-treatment anxiety. When you sit in the dental chair to have your braces placed, the primary sensation you will experience is simply having your mouth held open for an extended period. The orthodontist uses a cheek retractor to keep the teeth dry, which is crucial for the dental adhesive to bond properly.
First, the teeth are polished with a specialized pumice paste to remove any plaque or pellicle layer. Next, a mild conditioning gel (typically 37% phosphoric acid) is applied to the enamel for a few seconds. This etchant creates microscopic pores on the tooth surface, allowing the bonding agent to adhere securely. The gel is rinsed off, and the teeth are thoroughly dried. You may feel a slight cold sensation from the air syringe, but this is not painful.
The orthodontist then applies a primer and a small amount of composite resin adhesive to the back of each bracket. The brackets are meticulously positioned on the exact center of each tooth based on the customized treatment plan. A specialized curing light is used to harden the adhesive instantly. Finally, the initial archwire—usually a highly flexible nickel-titanium alloy—is threaded through the bracket slots and secured with tiny elastic bands (ligatures) or the bracket’s own closing mechanism in the case of self-ligating systems. Throughout this entire process, patients report zero pain.

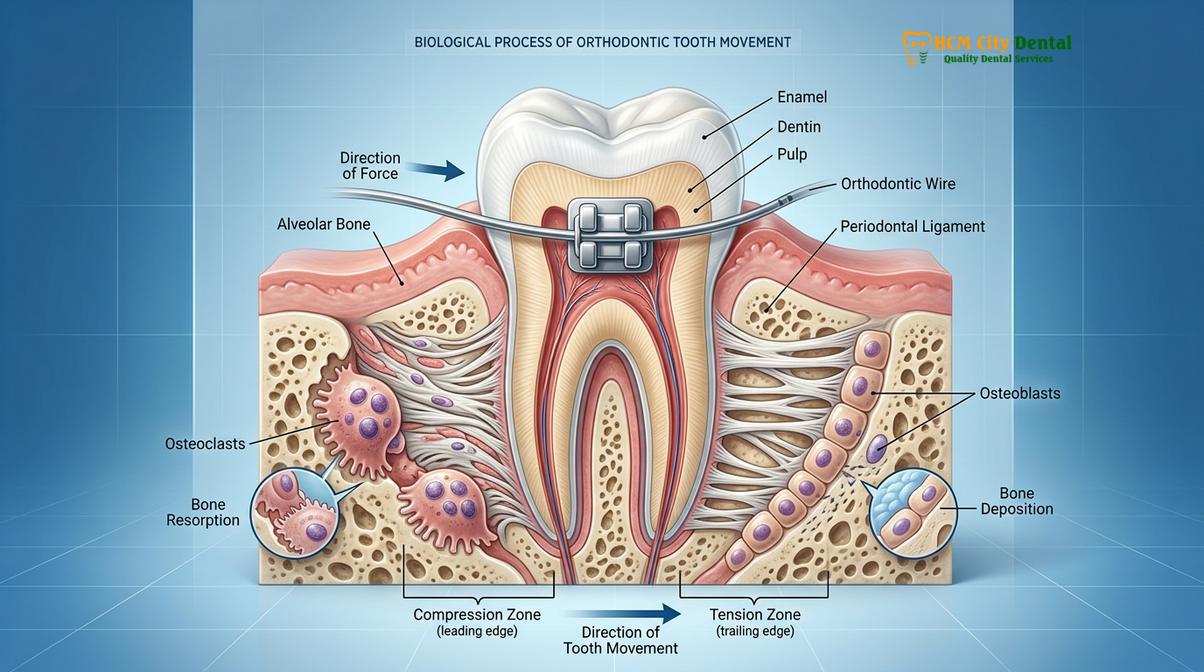
The Biological Mechanism: Why Teeth Become Sore
If the application is painless, why do patients ask does it hurt when you get braces? The discomfort begins several hours after the patient leaves the clinic. Once the archwire is engaged, it immediately begins attempting to return to its original U-shape, applying a continuous, gentle force to the teeth. This force is transferred from the bracket to the tooth root, and subsequently to the periodontal ligament (PDL)—the fibrous connective tissue that anchors the tooth to the alveolar bone.
When the PDL is compressed on one side of the root and stretched on the other, it alters the local blood flow. This mild ischemia (reduction in blood supply) triggers an aseptic inflammatory cascade. The body releases biochemical mediators, including prostaglandins, substance P, and histamine. These molecules stimulate the nerve endings within the PDL, transmitting pain signals to the brain. This is why the teeth feel tender, especially when biting down[1].
Simultaneously, this inflammatory response is exactly what allows the teeth to move. The chemical signals recruit specialized cells called osteoclasts to break down bone on the pressure side, while osteoblasts build new bone on the tension side. Therefore, the dull ache experienced is a direct clinical indicator of active, healthy bone remodeling.
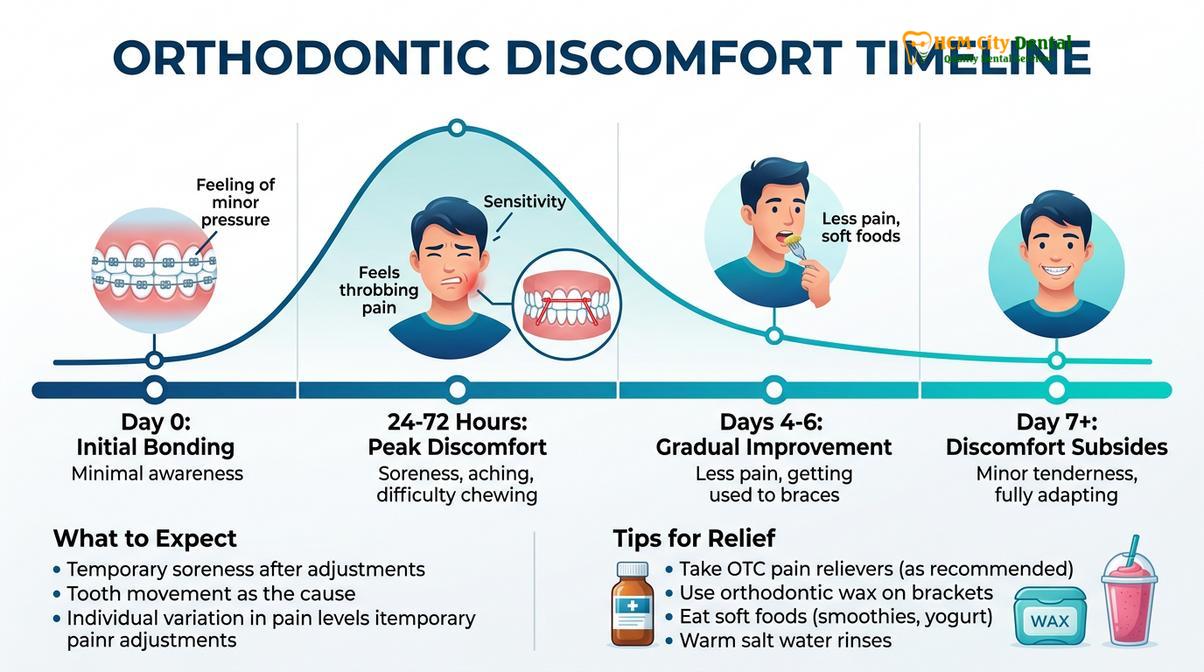
A Clinical Timeline of Orthodontic Discomfort
Orthodontic discomfort peaks between 24 and 72 hours after initial placement or adjustments, gradually subsiding within a week as the periodontal tissues adapt to the new forces.
Patients frequently ask their clinicians how long do braces hurt. Setting accurate expectations is a cornerstone of successful orthodontic therapy. The pain profile of braces is not constant; it follows a highly predictable bell curve that correlates with the biological stages of tooth movement.
The First 24 to 72 Hours: The Peak Inflammatory Phase
Immediately after leaving the clinic, your teeth will likely feel completely normal. However, as the biochemical cascade initiates, a sensation of tightness will develop within 4 to 6 hours. By the time you wake up the next morning, the teeth will feel noticeably sore. This soreness is typically described as a dull, generalized ache rather than a sharp, localized pain.
During days two and three, the discomfort reaches its peak. The periodontal ligaments are highly sensitized, making the teeth tender to vertical pressure. Chewing solid foods can be challenging during this window. Additionally, the soft tissues of the mouth—specifically the inner cheeks, lips, and tongue—are encountering the physical profile of the brackets and wires for the first time. Friction from speaking and eating can cause localized mucosal irritation or small aphthous ulcers (canker sores) to form.
Days 4 to 7: The Adaptation Phase
As the first week progresses, the acute inflammatory response begins to subside. The initial resistance of the bone gives way, and the tooth begins its microscopic migration. Consequently, the pressure within the PDL decreases. By days four through seven, patients notice a rapid improvement in their comfort levels. The teeth may still feel slightly loose—a normal clinical finding—but the constant ache diminishes.
Concurrently, the oral mucosa undergoes a process of keratinization. The tissues lining the cheeks and lips become slightly tougher in the areas where they contact the braces, forming a natural callus that prevents further irritation. By the end of the first week, most patients have fully adapted to the presence of the appliances and can resume a relatively normal diet, albeit with modifications to protect the hardware.
Monthly Adjustment Appointments: Reactivating the Cycle
Orthodontic treatment requires periodic adjustments, typically scheduled every 4 to 8 weeks depending on the specific mechanics being utilized. During these visits, the orthodontist may replace the archwire with a thicker, stiffer alloy, or apply new directional forces using power chains, elastics, or springs.
Each adjustment reactivates the inflammatory cascade, initiating a new cycle of bone remodeling. However, the discomfort experienced after an adjustment is almost universally reported as being much milder and shorter in duration than the initial placement. The periodontal tissues are already primed for movement, and the psychological shock of the new sensation is absent. Post-adjustment soreness usually resolves within 24 to 48 hours.
| Timeline | Clinical Milestone | Expected Sensation & Discomfort Level |
|---|---|---|
| Day 1 (Hours 1-6) | Appliance Bonding & Wire Insertion | No pain. Sensation of tightness and bulkiness begins. |
| Days 2-3 | Peak PDL Inflammation | Moderate dull ache. High sensitivity to biting pressure. Soft tissue friction. |
| Days 4-7 | Cellular Adaptation & Mucosal Keratinization | Mild, decreasing soreness. Cheeks adapt to brackets. |
| Weeks 2-4 | Active Tooth Movement | Generally pain-free. Teeth may feel slightly mobile. |
| Adjustment Days | Wire Progression / Force Reactivation | Mild soreness returning for 1-2 days, resolving quickly. |
Comparing Modalities: Does invisalign Hurt More Than Braces?
Invisalign generally causes less soft tissue irritation than traditional metal brackets, though both methods produce similar mild pressure during active tooth movement due to identical biological mechanisms.
With the rise of clear aligner therapy, a frequent point of comparison is the pain profile of different orthodontic systems. Patients evaluating their options often wonder does invisalign hurt more than braces. To answer this clinically, we must examine the differences in force application and hardware design.
Force Application: Continuous vs. Intermittent
Traditional fixed braces utilize highly advanced archwires that deliver continuous, light forces over a period of weeks. The wire is constantly working to express its shape. In contrast, clear aligner systems like Invisalign rely on a series of thermoplastic trays. Each tray is manufactured to be slightly straighter than the patient’s current dental alignment.
When a new aligner is seated, it applies a sudden, intermittent force to push the teeth into the new position. Because the force is applied all at once when switching to a new tray (usually every 7 to 14 days), patients often experience a distinct feeling of tightness and pressure for the first 24 hours of each new aligner cycle. However, because the total movement per tray is strictly limited (usually 0.25mm per stage), the biological trauma is minimized. Studies indicate that while the initial pressure of a new aligner can be noticeable, the overall pain scores reported by clear aligner patients are generally lower than those with fixed appliances[2].
Soft Tissue Irritation: The Aesthetic Advantage
The most significant difference in comfort between the two modalities lies in soft tissue interaction. Traditional braces, even modern low-profile ceramic brackets, present a textured surface to the inner lips and cheeks. This inevitably causes some degree of friction during the initial adaptation phase.
Clear aligners are fabricated from smooth, medical-grade polyurethane resins. They fit snugly over the clinical crown of the teeth and have scalloped edges that follow the gingival margin. Because there are no protruding metal tie-wings or sharp wire ends, mucosal abrasions and canker sores are exceedingly rare with Invisalign. For patients who play wind instruments or engage in contact sports, this smooth profile offers a distinct comfort advantage.
“The biological mechanism of bone remodeling is identical whether we use a titanium wire or a thermoplastic aligner. The teeth do not know what is pushing them. However, the delivery system matters. Aligners eliminate the mucosal trauma associated with brackets, which accounts for a significant portion of early orthodontic discomfort.”
— Dr. Nguyen Van Cuong, Lead Clinician

It is important to note that clear aligner therapy often requires the placement of “attachments”—small, tooth-colored composite bumps bonded to the enamel to give the plastic trays leverage. When the aligners are removed for eating, these attachments can feel slightly rough against the cheeks, though they are far less abrasive than traditional brackets.
Evidence-Based Strategies: How to Make Braces Not Hurt
Managing orthodontic discomfort involves a combination of over-the-counter analgesics, soft dietary modifications, cold therapy, and the strategic application of orthodontic wax to protect soft tissues.
While some degree of soreness is an unavoidable byproduct of moving teeth through bone, patients do not need to suffer needlessly. Orthodontic science has established clear, evidence-based protocols for mitigating pain. Understanding how to make braces not hurt empowers patients to navigate the initial stages of treatment with confidence.
Pharmacological Interventions: Choosing the Right Analgesic
When the dull ache of tooth movement becomes distracting, over-the-counter pain relievers are the first line of defense. However, the choice of medication is clinically significant. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), such as Ibuprofen (Advil) and Naproxen (Aleve), are highly effective at reducing pain. They work by inhibiting the cyclooxygenase (COX) enzymes, thereby reducing the production of prostaglandins.
While this provides excellent pain relief, prostaglandins are the exact biochemical messengers required to stimulate osteoclast activity and facilitate bone remodeling. Therefore, frequent, heavy use of NSAIDs can theoretically slow down the rate of orthodontic tooth movement[3].
For this reason, many orthodontists recommend Acetaminophen (Tylenol) as the preferred analgesic. Acetaminophen acts centrally in the brain to elevate the pain threshold but has minimal anti-inflammatory effects in the peripheral tissues. It effectively manages the discomfort without interfering with the biological mechanisms of tooth movement. Medication should be taken proactively, ideally an hour before an adjustment appointment, to stay ahead of the pain curve.
Dietary Modifications: The Soft Food Protocol
Mechanical stress exacerbates periodontal pain. Chewing hard, crunchy, or chewy foods applies heavy vertical forces to teeth that are already sensitized by orthodontic pressure. Adopting a soft food diet during the first few days of treatment is crucial for comfort.
Recommended foods include smoothies, yogurt, mashed potatoes, scrambled eggs, oatmeal, and pureed soups. Cold foods and beverages offer an additional therapeutic benefit. The cold temperature causes local vasoconstriction, reducing blood flow and inflammation in the PDL. Furthermore, modern orthodontic archwires are often made of heat-activated nickel-titanium. Drinking ice water can temporarily cool the wire, making it slightly more flexible and reducing the active force on the teeth for a brief period of relief.
Clinical Case Review: Managing Early Treatment Discomfort
A 14-year-old patient visited HCMC Dental Clinic in Ho Chi Minh City for the initiation of comprehensive orthodontic treatment using traditional metal braces. Anticipating discomfort, the clinical team provided a detailed pain management protocol. The patient was instructed to consume a chilled, soft diet for 48 hours and utilize orthodontic wax on the canine brackets, which frequently cause lip irritation. By adhering to the protocol and taking a single dose of Acetaminophen on the second night, the patient reported only mild, highly manageable pressure, successfully transitioning to a normal diet by day five without any mucosal ulcerations.
Orthodontic Wax and Barrier Methods
For soft tissue irritation, orthodontic wax is an indispensable tool. This medical-grade silicone or beeswax can be pinched off, rolled into a small ball, and pressed directly over any bracket or wire that is rubbing against the cheek or lip. The wax creates a smooth, protective barrier, allowing the ulcerated mucosa to heal.
Patients should dry the bracket with a tissue before applying the wax to ensure it adheres properly. It is perfectly safe if accidentally swallowed. In addition to wax, warm saltwater rinses (one teaspoon of salt in a glass of warm water) can be used two to three times a day. The hypertonic saline solution draws fluid out of inflamed tissues, reducing swelling and promoting the rapid healing of any small cuts or canker sores[4].
“Patient compliance with dietary guidelines and the proactive use of barrier wax during the first week are the most significant factors in ensuring a comfortable transition into orthodontic treatment. We prioritize patient education to prevent pain before it starts.”
— Dr. Nguyen Van Cuong
For patients who experience severe bruxism (teeth grinding) at night, the pressure on sore teeth can disrupt sleep. In some cases, discussing a specialized orthodontic nightguard with your clinician can provide a cushioning effect, though this must be carefully designed so as not to interfere with the active tooth movement.
When to See a Doctor: Identifying Abnormal Pain
While mild to moderate soreness is a standard part of the orthodontic journey, it is vital to distinguish between normal inflammatory discomfort and abnormal pain that requires clinical intervention. Orthodontic emergencies are rare, but recognizing the red flags ensures that complications are addressed promptly.
Normal pain is characterized by a dull, generalized ache that peaks within a few days of an appointment and gradually subsides. It is symmetrical (affecting all teeth that are being moved) and responds well to over-the-counter analgesics. Abnormal pain, however, is typically sharp, highly localized, and persistent.
Clinical Red Flags: When to Contact Your Orthodontist
- Severe, Unrelenting Pain: Pain that wakes you up at night, does not respond to maximum doses of analgesics, or worsens after the first week.
- Poking Wires: As teeth move, the archwire may extend out the back of the molar tube, causing a sharp, lacerating pain in the back of the cheek. This requires the wire to be clipped by the clinician.
- Traumatic Injury: If you sustain a blow to the face and the braces are driven into the soft tissue, or if a tooth feels excessively loose following trauma.
- Signs of Infection: Localized swelling of the gums, purulent discharge (pus), or a pimple-like bump on the gums near a tooth root.
If a bracket becomes debonded (unglued) from the tooth, it will typically slide freely along the archwire. While not usually painful, it renders that specific tooth inactive and can cause irritation. Patients should not attempt to remove or glue the bracket themselves. Instead, apply wax to stabilize it and contact the clinic for a repair appointment.
Dr. Cuong emphasizes that open communication between the patient and the clinical team is essential. If you are ever unsure whether the sensation you are experiencing is normal, it is always safer to schedule a brief clinical evaluation. A quick adjustment can often resolve an issue that would otherwise cause days of unnecessary discomfort[5].

Orthodontic treatment is a profound investment in your long-term oral health and facial aesthetics. Whether you are exploring braces for expat children or adult aligner therapy, understanding the biological realities of the process allows you to approach treatment with confidence. The temporary discomfort experienced in the early stages is a small price to pay for a lifetime of functional harmony and a beautiful smile. If you are ready to begin your journey, a comprehensive dental plan tailored to your specific anatomical needs is the first step.
For personalized diagnostic advice and to explore the most comfortable orthodontic modalities available today, we encourage you to schedule a consultation at HCMC Dental Clinic in Ho Chi Minh City. Our clinical team is dedicated to utilizing the latest low-friction technologies to ensure your path to a perfect smile is as seamless and pain-free as possible.
Frequently Asked Questions
Does it hurt to get your braces off?
No, removing braces is generally painless and much faster than the application process. You may feel slight pressure as the orthodontist uses a specialized tool to gently squeeze and pop the brackets off your teeth, followed by a polishing step to remove residual adhesive. The entire debonding process is non-invasive and leaves the enamel smooth and intact.
Can braces cause headaches?
Yes, tension headaches can occasionally occur during the first few days after getting braces or following an adjustment. The pressure applied to your teeth and jaws can radiate through the trigeminal nerve, causing mild, temporary head discomfort that responds well to standard analgesics. Staying hydrated and practicing jaw relaxation techniques can help mitigate this symptom.
Why do my teeth feel loose with braces?
Teeth feeling slightly loose is a normal and necessary part of orthodontic treatment. In order for teeth to move into their new positions, the periodontal ligaments must stretch and the surrounding bone must temporarily soften, creating a sensation of mobility. Once the teeth reach their final positions and the braces are removed, the bone will harden and the teeth will stabilize.
Is it normal for braces to cut my cheeks?
Mild irritation or small abrasions on the inner cheeks and lips are very common during the first two weeks of treatment. Your oral mucosa needs time to toughen and adapt to the metal or ceramic brackets, which can be managed effectively using orthodontic wax. Over time, the tissues develop a natural resistance, and the irritation resolves completely.
Can I use numbing gel for braces pain?
Yes, over-the-counter topical oral anesthetics containing benzocaine can provide temporary relief for localized soft tissue irritation. Applying a small amount directly to the sore spots on your gums or cheeks can numb the area, making eating and speaking more comfortable. However, these gels only treat mucosal pain and will not relieve the deep, dull ache of bone remodeling.
References
- American Journal of Orthodontics and Dentofacial Orthopedics. Pain perception and management in orthodontic treatment: A comprehensive review. (2021).
- European Journal of Orthodontics. Cellular and molecular mechanisms of orthodontic tooth movement and associated pain. (2020).
- Journal of Clinical Orthodontics. Comparative analysis of discomfort between clear aligners and fixed appliances. (2022).
- Angle Orthodontist. The effect of non-steroidal anti-inflammatory drugs on orthodontic tooth movement. (2019).
- International Journal of Dentistry. Soft tissue adaptation and mucosal lesions in early orthodontic treatment. (2018).