

Most patients wear braces for 18 to 24 months, though minor corrections may take only six months, and complex bite issues can require up to three years. The exact duration depends on your specific malocclusion, age, chosen orthodontic appliance, and biological response to tooth movement.
Clinical Summary:
The duration of orthodontic treatment is a highly individualized timeline dictated by the biological principles of bone remodeling. When patients ask how long do you have to wear braces, the clinical answer relies on the severity of the malocclusion, the patient’s skeletal maturity, and the specific biomechanical forces applied. Treatment is generally divided into four distinct phases: leveling and aligning, working phase (space closure and bite correction), finishing and detailing, and finally, retention. While mild aesthetic corrections can be achieved in under a year, comprehensive functional bite corrections typically span one to three years. Factors such as appliance choice—ranging from traditional brackets to clear aligners—and strict patient compliance with oral hygiene and adjunctive wear (like elastics) significantly influence the overall speed and success of the treatment.
Key Takeaways:
- Average comprehensive orthodontic treatment lasts between 18 and 24 months.
- Minor cosmetic alignments can be completed in 6 to 12 months.
- Complex skeletal discrepancies or impacted teeth may extend treatment to 36 months or longer.
- Patient compliance with elastics and aligner wear is the most critical factor in preventing delays.
- The biological rate of bone remodeling limits how fast teeth can safely be moved.
- Lifelong retainer wear is mandatory to maintain the final results after braces are removed.
The Biological Timeline: How Long Do You Have to Wear Braces?
Orthodontic tooth movement relies on a biological process called bone remodeling, which dictates that safe, permanent alignment typically requires one to three years.
To truly understand the timeline of orthodontic treatment, one must look beyond the metal wires and brackets and examine the cellular biology of the human jaw. Teeth are not rigidly fixed into the jawbone; rather, they are suspended in their sockets by a hammock-like structure called the periodontal ligament (PDL). When orthodontic forces are applied, this ligament is compressed on one side of the tooth and stretched on the other. This mechanical stress triggers a complex biological cascade [1].
On the compressed side of the PDL, specialized cells called osteoclasts begin to break down the alveolar bone, creating space for the tooth to move into. Simultaneously, on the stretched side, cells known as osteoblasts generate new bone tissue to fill the void left behind. This continuous process of bone resorption and bone deposition is known as bone remodeling. Because this biological mechanism operates at a specific, natural pace, there is a physiological limit to how fast teeth can be moved safely. Applying excessive force does not speed up the process; in fact, it can cause a condition called hyalinization, where the blood supply to the PDL is cut off, temporarily halting tooth movement and potentially causing permanent damage to the tooth roots [6].

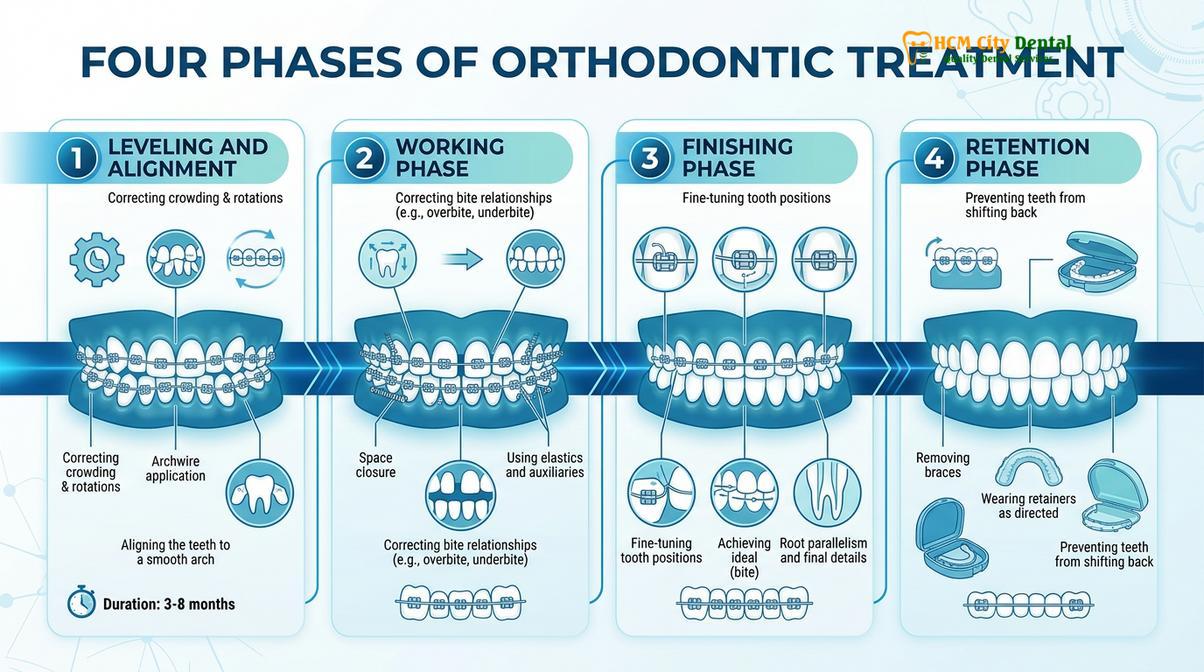
Because of these biological constraints, the timeline for wearing braces is generally divided into four distinct clinical phases:
- Phase 1: Leveling and Aligning (Months 1-6): When first getting braces, the primary goal is to bring the crowns of the teeth into a level arch. Orthodontists use highly flexible, shape-memory wires (typically Nickel-Titanium) that exert light, continuous forces to untwist rotated teeth and correct vertical discrepancies.
- Phase 2: The Working Phase (Months 6-15): This is often the longest phase of treatment. Thicker, more rigid stainless steel wires are utilized to close extraction spaces, correct the anterior-posterior relationship of the bite (overbite or underbite), and adjust the angulation of the tooth roots.
- Phase 3: Finishing and Detailing (Months 15-24): In this meticulous phase, the orthodontist makes micro-adjustments to ensure the teeth interlock perfectly. Custom bends are placed in the wire to perfect the torque, tip, and rotation of individual teeth, ensuring optimal functional occlusion and aesthetics.
- Phase 4: Retention (Post-Treatment): Once the active movement is complete and the braces are removed, the bone surrounding the teeth is still relatively soft. The retention phase is critical to hold the teeth in their new positions while the bone fully mineralizes and the periodontal fibers reorganize.
While the best age for orthodontic braces is generally considered to be during early adolescence (ages 11-14) when the jawbones are still actively growing and highly responsive to modification, adults can also achieve excellent results. However, adult bone is denser and lacks growth potential, which can slightly extend the biological timeline of tooth movement [2].
Key Factors Influencing Your Orthodontic Treatment Duration
Your treatment timeline is primarily determined by the severity of your malocclusion, your skeletal maturity, and your individual biological response to orthodontic forces.
No two orthodontic cases are exactly alike. When a patient asks a clinician how long they will need to wear braces, the estimate is based on a comprehensive diagnostic workup, which includes panoramic and cephalometric X-rays, digital intraoral scans, and clinical photographs. Several key variables dictate the length of the treatment plan.
The most significant factor is the severity and classification of the malocclusion (bite misalignment). Orthodontic issues are broadly categorized into three classes:
- Class I Malocclusion: The upper and lower jaws are properly aligned, but there are issues with individual teeth, such as crowding, spacing, or mild rotations. These cases are typically the fastest to resolve, often taking 12 to 18 months.
- Class II Malocclusion (Overbite/Overjet): The upper jaw and teeth protrude significantly over the lower jaw. Correcting this discrepancy often requires moving the entire upper dentition backward or encouraging lower jaw growth in adolescents. These cases generally require 18 to 24 months.
- Class III Malocclusion (Underbite): The lower jaw protrudes past the upper jaw. This is often a complex skeletal issue that is more challenging to correct, frequently requiring 24 to 36 months of treatment, and sometimes necessitating surgical intervention in adults.
Another critical factor is the presence of impacted teeth, most commonly the maxillary canines. If a tooth is trapped within the jawbone, the orthodontist must surgically expose it and slowly drag it into the dental arch using specialized attachments and elastic chains. This process alone can add six to twelve months to the overall treatment time.
| Clinical Factor | Mild Complexity (6-12 Months) | Moderate Complexity (12-24 Months) | Severe Complexity (24-36+ Months) |
|---|---|---|---|
| Crowding / Spacing | Minor gaps or slight overlapping of anterior teeth. | Moderate crowding requiring arch expansion or slenderizing (IPR). | Severe crowding requiring the extraction of premolars. |
| Bite Relationship | Class I (Normal skeletal relationship). | Class II or Class III requiring elastic wear. | Severe skeletal discrepancies requiring orthognathic surgery. |
| Tooth Eruption | All permanent teeth fully erupted and positioned normally. | Delayed eruption of certain permanent teeth. | Impacted teeth (e.g., canines) requiring surgical exposure and traction. |
| Patient Age | Growing adolescents (high bone plasticity). | Young adults (moderate bone density). | Older adults with dense cortical bone or periodontal compromise. |
The process of getting braces involves a period of adaptation. During the first few weeks, the teeth may feel mobile, and the supporting structures are highly active. The initial rate of movement can seem rapid as the crowns align, but patients must understand that moving the roots of the teeth through dense alveolar bone during the later stages of treatment is a much slower, more deliberate process.
How Different Types of braces Affect Treatment Speed
The specific orthodontic appliance you choose—whether traditional brackets, self-ligating systems, or clear aligners—can influence both the mechanics of tooth movement and the overall treatment duration.
Advancements in orthodontic technology have provided patients with multiple appliance options, each with its own biomechanical advantages and limitations. The choice of appliance can subtly impact how efficiently certain types of tooth movements are achieved.
Traditional stainless steel brackets, sometimes referred to colloquially as original braces, remain the gold standard for treating highly complex malocclusions. Historically, metal bands for braces were placed around every single tooth. Today, modern systems rely primarily on brackets bonded directly to the enamel, with bands usually reserved only for the heavy-duty molar teeth. Traditional braces use small elastic ties (ligatures) to hold the archwire into the bracket slot. While highly effective, these elastics create friction, which can slightly slow down the sliding mechanics needed during space closure.
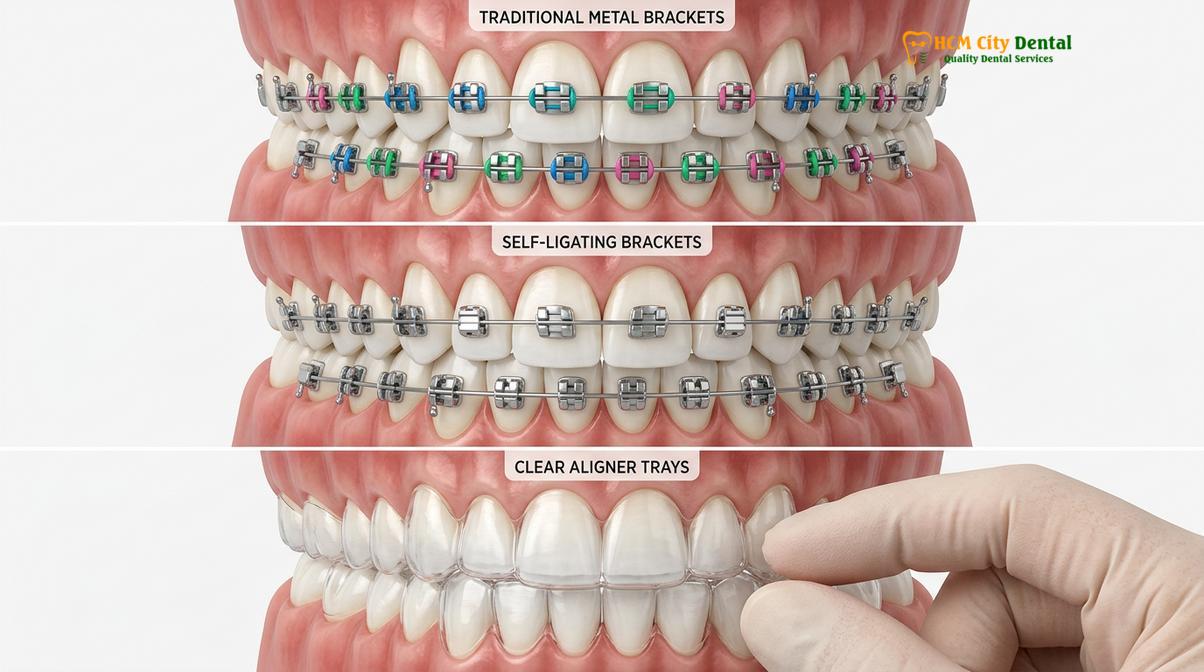
To address the issue of friction, self-ligating systems were developed. These are essentially metal braces without rubber bands. Instead of elastic ties, self-ligating brackets feature a built-in sliding door or clip that secures the wire. Because there are braces no bands or elastic ligatures creating drag, the wire can slide more freely through the brackets. Some clinical studies suggest that self-ligating systems can reduce the time spent in the initial leveling and aligning phase and may require fewer adjustment appointments, though the overall treatment duration is often similar to traditional braces [3].
For patients concerned about aesthetics, ceramic braces are a popular alternative. Patients frequently ask, are clear braces good for complex cases? Yes, ceramic brackets function almost identically to metal brackets and are capable of treating severe malocclusions. However, ceramic material is more brittle than stainless steel and can create slightly more friction against the metal archwire, which might marginally extend treatment time in cases requiring significant space closure. Additionally, patients must be diligent about oral hygiene to learn about preventing yellow stains around brackets, as the clear elastic ties used with ceramic braces can discolor.
Finally, clear aligner therapy has revolutionized the field. Aligners apply force differently than fixed braces, pushing the teeth rather than pulling them. For mild to moderate crowding, spacing, and certain types of bite correction, clear aligners can sometimes achieve results faster than traditional braces because the digital treatment plan optimizes the exact movement of every tooth simultaneously. However, for severe vertical discrepancies, complex root torquing, or significant rotations of cylindrical teeth (like premolars), fixed braces are generally more efficient and predictable.
Complex Cases: When Additional Appliances or Surgery Are Needed
Severe skeletal discrepancies often require adjunctive appliances or surgical intervention, which can significantly extend the active phase of your orthodontic treatment.
In many instances, brackets and wires alone are insufficient to correct the underlying structural issues of the jaw. When the upper and lower jaws grow at different rates or in different directions, the orthodontist must employ adjunctive appliances to modify skeletal growth or compensate for the discrepancy.
For growing children and adolescents, appliances like Palatal Expanders are frequently used. An expander is attached to the upper molars and features a central screw that is turned daily. This gently separates the midpalatal suture, widening the upper jaw to correct crossbites and create space for crowded teeth. This orthopedic phase of treatment usually takes several months and is often completed before or in conjunction with the placement of full braces. Other appliances, such as Headgear or functional appliances like the Herbst or Forsus devices, are used to correct severe overbites by holding the upper jaw back or posturing the lower jaw forward.
Clinical Warning: Failure to wear prescribed adjunctive appliances, such as intermaxillary elastics (rubber bands) or headgear, is the leading cause of prolonged orthodontic treatment. Without the continuous directional forces provided by these appliances, bite correction will stall entirely, adding months or even years to your timeline.
In adult patients, the jawbones have fused, and growth modification is no longer possible. For those with severe skeletal malocclusions—such as a pronounced underbite, a severe open bite where the front teeth do not touch, or significant facial asymmetry—orthodontics alone cannot achieve a functional bite. In these scenarios, orthognathic (jaw) surgery is required [5].
The timeline for surgical orthodontic cases is extensive. It begins with 12 to 18 months of pre-surgical orthodontics, where surgical braces are used to align the teeth independently within their respective jaws. Counterintuitively, the bite often looks and feels worse during this phase as dental compensations are removed. Once the teeth are perfectly positioned, the oral and maxillofacial surgeon performs the orthognathic surgery to physically reposition the jawbones. Attempting jaw surgery without braces is generally contraindicated, as the teeth must interlock perfectly immediately after the jaws are moved to ensure stability. Following a recovery period of several weeks, the patient undergoes a post-surgical orthodontic phase lasting 6 to 12 months to finalize the bite detailing.
For patients with very minor aesthetic concerns who are wondering how to get straight teeth without braces, restorative dentistry options such as porcelain veneers or dental bonding can sometimes provide the illusion of straight teeth in a matter of weeks. However, these are camouflage techniques that do not correct underlying bite issues or root positions.
The Patient’s Role: Accelerating vs. Delaying Your Progress
Patient compliance, including strict adherence to dietary guidelines and excellent oral hygiene, is the most critical variable you can control to prevent treatment delays.
While the orthodontist designs the biomechanical blueprint, the patient is ultimately responsible for the daily execution of the treatment plan. The duration of your time in braces is heavily dependent on your level of compliance [4].
The most common cause of delayed treatment is broken appliances. Every time a bracket is sheared off a tooth by biting into hard, crunchy, or sticky foods (such as ice, hard candies, nuts, or chewing gum), the active tooth movement for that specific tooth stops. Furthermore, repairing broken brackets requires the orthodontist to step backward in the treatment progression, often requiring a return to a lighter, more flexible archwire to re-engage the errant tooth. Multiple breakages can easily add several months to your overall timeline.

Oral hygiene is equally critical. Plaque accumulation around brackets leads to gingivitis (gum inflammation). Swollen, bleeding gums are not only uncomfortable but also alter the biological environment of the periodontal ligament, making tooth movement slower and less predictable. In severe cases of poor hygiene, the orthodontist may be forced to remove the braces prematurely to prevent permanent damage to the enamel and supporting bone.
“Orthodontic treatment is a partnership. I can design the most precise digital ClinCheck or bend the most intricate archwires, but if a patient does not wear their prescribed elastics 22 hours a day, the bite simply will not correct. Compliance is the true engine of orthodontic speed.”
— Dr. Nguyen Van Cuong, Orthodontic Specialist
For patients utilizing clear aligners, compliance is measured in wear time. Aligners must be worn for 20 to 22 hours every single day, removed only for eating, drinking anything other than plain water, and oral hygiene. Failing to meet this wear time means the teeth will not track properly with the digital plan, necessitating mid-course corrections or additional refinement scans, which prolong the treatment.
Financial planning is also a part of the patient journey, and maintaining consistent appointments is vital. Patients seeking affordable financing options or exploring a monthly payment plan should ensure their arrangements allow for uninterrupted care, as missing adjustment appointments directly stalls progress.
The Removal Process and Retention Phase
The active phase concludes with the debonding appointment, followed immediately by the retention phase to stabilize the teeth in their new anatomical positions.
As the treatment nears its conclusion, patients frequently ask how long does it take to get braces off. The actual debonding appointment is relatively quick, usually taking about an hour. The orthodontist uses specialized pliers to gently squeeze the base of each bracket, breaking the adhesive bond and lifting the bracket away from the tooth. The remaining composite resin is then carefully polished off the enamel using a high-speed handpiece and specialized finishing burs, leaving the teeth smooth and clean.
Many patients look forward to aesthetic enhancements immediately following removal. Understanding the teeth whitening after braces timeline is important, as clinicians generally recommend waiting at least one to two months before undergoing professional bleaching to allow the enamel to remineralize and tooth sensitivity to subside.
Clinical Case Study: The Importance of Retention
A 24-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City seeking retreatment. She had successfully completed 24 months of traditional braces as a teenager but failed to wear her removable retainers during her university years. Due to natural mesial drift and the elastic memory of the periodontal fibers, her lower anterior teeth had severely crowded once again. She required an additional 14 months of clear aligner therapy to recapture her straight smile, highlighting that orthodontic retention is a lifelong commitment.
The removal of the braces marks the end of active treatment but the beginning of the retention phase. Teeth have a strong tendency to relapse—or shift back toward their original positions—especially in the first 12 months after braces are removed. This occurs because the periodontal ligaments are still stretched and the surrounding alveolar bone has not fully calcified around the new root positions [7].
To prevent relapse, orthodontists prescribe retainers. There are several types:
- Essix Retainers: Clear, vacuum-formed plastic trays that fit snugly over the teeth, similar to clear aligners.
- Hawley Retainers: Traditional removable retainers made of an acrylic palate and a metal wire that wraps around the front teeth.
- Fixed Lingual Retainers: A custom-fitted wire bonded permanently to the tongue-side (lingual) surfaces of the front teeth, providing continuous, passive retention without relying on patient compliance.
When to See a Doctor (Orthodontist)
While general dentists are highly skilled in maintaining overall oral health, the specialized dentist for braces is called an orthodontist. Orthodontists complete dental school and then undergo an additional two to three years of rigorous, full-time residency training focused exclusively on the biomechanics of tooth movement and dentofacial orthopedics.
If you are currently undergoing treatment, you should contact your orthodontist immediately if you experience any of the following:
- A broken bracket that is sliding on the wire or causing soft tissue trauma.
- A poking wire that cannot be managed with orthodontic wax.
- Severe, unmanageable pain that persists beyond the normal 3-5 day adjustment period.
- A lost or broken retainer (this is a dental emergency, as teeth can shift noticeably within just a few days).
- Unusual mobility of a tooth that seems excessive.
“We strongly advise patients seeking comprehensive orthodontic care to consult with a certified specialist. Proper diagnosis and treatment planning are the foundations of a stable, functional bite that will last a lifetime, rather than just a temporary cosmetic fix.”
— Dr. Nguyen Van Cuong, HCMC Dental Clinic

For those considering starting their journey, reviewing a comprehensive orthodontic care guide and understanding how to go about choosing the right orthodontist are crucial first steps toward achieving a healthy, beautiful smile.
Frequently Asked Questions
What is the absolute minimum time you can wear braces?
The minimum time for wearing braces is typically six months for very minor cosmetic corrections. However, comprehensive orthodontic treatment involving bite correction and root movement generally requires at least 12 to 18 months to ensure long-term stability.
Can I speed up my orthodontic treatment time?
Yes, you can optimize treatment time by strictly following your orthodontist’s instructions regarding elastic wear, maintaining impeccable oral hygiene, and never missing adjustment appointments. Adjunctive technologies like high-frequency vibration devices may also offer marginal speed improvements in specific cases.
Do clear aligners work faster than traditional metal braces?
Clear aligners can work faster than traditional braces for mild to moderate crowding or spacing issues. However, for complex bite corrections, severe rotations, or significant vertical movements, traditional fixed appliances are often more efficient and predictable.
Why do some people wear braces for more than three years?
Treatments extending beyond three years usually involve severe skeletal discrepancies, impacted teeth, orthognathic surgery preparation, or significant patient non-compliance. Missing appointments or failing to wear prescribed elastics are the most common reasons for delayed treatment completion.
Will my teeth shift back immediately after my braces are removed?
Teeth are highly susceptible to shifting immediately after braces removal because the surrounding bone and periodontal ligaments have not fully solidified. Wearing your prescribed retainers exactly as directed is mandatory to prevent orthodontic relapse.
References
- American Journal of Orthodontics and Dentofacial Orthopedics. Biological mechanisms of tooth movement and bone remodeling. (2021).
- Journal of Clinical Orthodontics. Average duration of comprehensive orthodontic treatment in adult and adolescent patients. (2020).
- European Journal of Orthodontics. Comparative efficacy of self-ligating vs conventional brackets in alignment speed. (2019).
- Angle Orthodontist. The impact of patient compliance on orthodontic treatment duration and outcomes. (2022).
- International Journal of Oral and Maxillofacial Surgery. Orthognathic surgery timelines and presurgical orthodontic preparation. (2018).
- Journal of Dental Research. Periodontal ligament response to continuous vs intermittent orthodontic forces. (2021).
- British Dental Journal. Retention protocols and long-term stability following fixed appliance therapy. (2020).



