When searching for a highly trusted practitioner like a “dr black dentist,” patients are fundamentally looking for a gold standard in comprehensive general, restorative, and cosmetic dentistry. True clinical excellence requires precise diagnostics, evidence-based periodontal therapies, and advanced prosthodontic workflows to ensure long-term oral health and aesthetic harmony.
Clinical Summary:
Comprehensive general dentistry integrates preventive care, periodontal maintenance, and advanced restorative procedures to rehabilitate oral function. From routine prophylaxis to complex porcelain restorations and implant-supported prosthetics, modern clinical workflows prioritize tissue preservation and biomechanical stability. Expert practitioners utilize high-resolution imaging and biocompatible materials to deliver predictable, long-lasting patient outcomes while mitigating the progression of oral pathologies.
Key Takeaways:
- General dentistry encompasses preventive, restorative, and cosmetic disciplines for holistic patient care.
- Periodontal maintenance is the foundational prerequisite for the success of any dental restoration.
- Modern restorative materials offer superior marginal adaptation, minimizing the risk of secondary caries.
- Prosthodontic rehabilitation restores occlusal harmony and prevents the migration of adjacent teeth.
- Consistent clinical monitoring ensures the longevity of both natural dentition and implant-supported prosthetics.
The Clinical Scope of Comprehensive General Dentistry
Comprehensive general dentistry provides a unified approach to oral health, seamlessly blending preventive diagnostics with advanced restorative and cosmetic interventions to maintain optimal stomatognathic function.
In the realm of modern oral healthcare, the search for a “dr black dentist” has become synonymous with patients seeking a highly reputable, comprehensive solo-practice model—a standard of care that prioritizes continuity, rigorous diagnostics, and personalized treatment plans. This archetype of dentistry moves beyond mere reactive treatments, focusing instead on a proactive, medical model of oral health management. At HCMC Dental Clinic in Ho Chi Minh City, our clinical philosophy mirrors this dedication to comprehensive care, ensuring that every patient receives a meticulous evaluation of their entire oral ecosystem.
The foundation of this approach lies in advanced diagnostics. Before any restorative or cosmetic procedure is initiated, a thorough clinical examination is mandatory. This includes full-mouth periodontal charting, oral cancer screenings, and high-resolution radiographic imaging. By assessing the structural integrity of the teeth, the health of the periodontium, and the dynamics of the temporomandibular joint (TMJ), clinicians can formulate a holistic treatment strategy. For a deeper understanding of these foundational principles, patients are encouraged to review our comprehensive general dental guide, which outlines the essential components of lifelong oral health maintenance.

The Shift Toward Minimally Invasive Dentistry
Historically, dental treatments often required aggressive removal of tooth structure to accommodate mechanical retention for restorative materials. Today, the paradigm has shifted toward minimally invasive dentistry (MID). This philosophy relies on early detection of carious lesions and the utilization of adhesive dental materials that bond directly to the enamel and dentin. By preserving the maximum amount of healthy tooth structure, clinicians can maintain the tooth’s natural biomechanical strength and significantly extend its lifespan in the oral cavity. [1]
Minimally invasive techniques also encompass remineralization protocols. Early enamel demineralization, often presenting as white spot lesions, can frequently be reversed without surgical intervention. Through the targeted application of fluoride varnishes, casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) complexes, and rigorous oral hygiene instruction, the enamel matrix can be fortified, halting the progression of dental caries before cavitation occurs.
Preventive and Periodontal Workflows
Preventive dentistry and periodontal therapy form the critical foundation of oral health, focusing on biofilm management, calculus removal, and the preservation of the supporting alveolar bone.
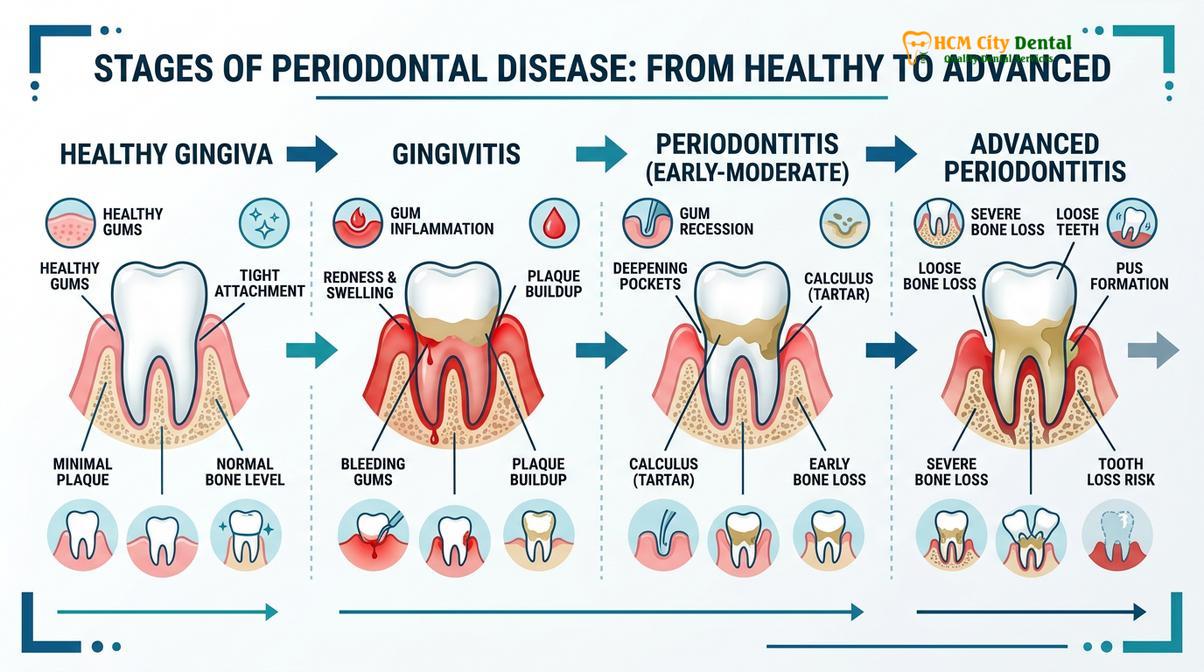
No restorative or cosmetic dental procedure can achieve long-term success without a healthy periodontal foundation. The periodontium—comprising the gingiva, periodontal ligament, cementum, and alveolar bone—acts as the crucial support system for the dentition. When bacterial biofilm is allowed to accumulate along the gingival margin, it initiates an inflammatory cascade known as gingivitis. If left untreated, this localized inflammation can progress into periodontitis, characterized by the irreversible destruction of the periodontal ligament and alveolar bone.
Clinical periodontal workflows begin with precise diagnostic probing. A periodontal probe is utilized to measure the depth of the gingival sulcus; depths exceeding 3 millimeters, especially when accompanied by bleeding on probing (BOP), indicate active periodontal disease. Dr. Nguyen Van Cuong emphasizes that comprehensive periodontal charting is the most critical step in preventing premature tooth loss. Based on these diagnostics, a tailored hygiene protocol is established, ranging from routine prophylaxis to advanced non-surgical periodontal therapy. [2]
Non-Surgical Periodontal Therapy: Scaling and Root Planing
For patients diagnosed with periodontitis, the standard of care is scaling and root planing (SRP). This meticulous procedure involves the mechanical debridement of plaque and calculus deposits from both the supragingival and subgingival tooth surfaces. Following the removal of these calcified deposits, the cementum of the tooth root is smoothed (planed) to remove necrotic tissue and bacterial endotoxins. This creates a biologically acceptable surface that encourages the reattachment of the gingival tissues and a reduction in periodontal pocket depths.
In addition to mechanical debridement, adjunctive therapies may be employed to optimize healing. These can include the localized delivery of antimicrobial agents, such as chlorhexidine chips or minocycline microspheres, directly into the periodontal pockets. Furthermore, patient education regarding dietary habits is essential, as certain acidic and sugary beverages can exacerbate both caries and gingival inflammation. Understanding the clinical facts about enamel staining and erosion is vital for maintaining the results of periodontal and preventive therapies.
Advanced Restorations: From Direct Fillings to Endodontics
Advanced restorative dentistry utilizes biocompatible materials and precise endodontic techniques to salvage compromised teeth, eradicate infection, and restore optimal biomechanical function.
When dental caries progresses beyond the enamel and penetrates the dentin, restorative intervention becomes necessary to halt the decay and rebuild the tooth’s anatomy. The evolution of dental materials has revolutionized this process. While dental amalgam was once the standard due to its high compressive strength, modern dentistry predominantly utilizes advanced composite resins. These resin-based materials offer superior aesthetic integration and, more importantly, bond micromechanically to the tooth structure, reinforcing the remaining enamel and dentin.
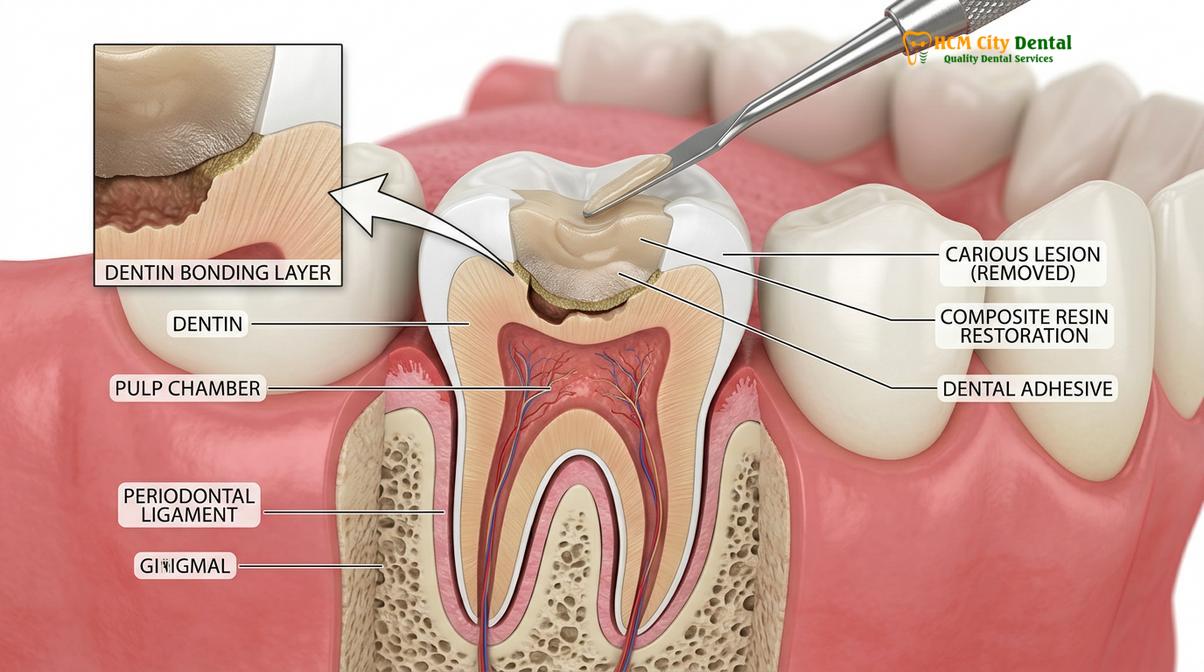
The clinical workflow for a direct composite restoration requires meticulous isolation, often utilizing a rubber dam to prevent salivary contamination. The carious tissue is excavated using precise rotary instruments, followed by the application of a mild phosphoric acid etchant. This etchant creates microscopic porosities in the tooth surface. A bonding agent is then applied and cured with a specific wavelength of blue light, creating a hybrid layer that securely anchors the composite resin to the tooth. [3]
Endodontic Therapy: Preserving the Natural Dentition
When bacterial infection breaches the pulp chamber—the innermost aspect of the tooth containing nerves and blood vessels—a direct restoration is no longer sufficient. In these cases, endodontic therapy (root canal treatment) is indicated to salvage the tooth and prevent the spread of infection into the periapical tissues and alveolar bone.
The endodontic workflow involves the chemomechanical debridement of the root canal system. Specialized endodontic files are used to meticulously clean and shape the complex anatomy of the canals, while potent irrigants, such as sodium hypochlorite, are utilized to dissolve necrotic tissue and eradicate bacterial biofilms. Once the canal system is thoroughly disinfected, it is obturated (filled) with a biocompatible material called gutta-percha and sealed with a resin cement. Because endodontically treated teeth often suffer from significant structural loss and become more brittle over time, they typically require full-coverage protection, such as a porcelain crown, to withstand the immense forces of mastication.
| Material Type | Clinical Indications | Biomechanical Advantages | Aesthetic Profile |
|---|---|---|---|
| Composite Resin | Small to moderate carious lesions, anterior aesthetics | Micromechanical bonding, reinforces tooth structure | Excellent; shade-matched to natural dentition |
| Glass Ionomer | Class V lesions, pediatric dentistry, high caries risk | Chemical bonding, continuous fluoride release | Moderate; opaque appearance |
| Dental Amalgam | Large posterior restorations (historical standard) | High compressive strength, moisture tolerant during placement | Poor; metallic appearance, potential for tooth discoloration |
Cosmetic Dentistry and Aesthetic Rehabilitation
Aesthetic rehabilitation combines artistic principles with rigorous prosthodontic protocols to enhance smile dynamics using veneers, crowns, and advanced ceramic materials.
Cosmetic dentistry transcends simple aesthetic enhancements; it is a complex discipline that requires a profound understanding of facial harmony, phonetics, and occlusal function. A successful aesthetic rehabilitation must not only look natural but also function flawlessly within the stomatognathic system. This requires meticulous planning, often utilizing digital smile design software to analyze the patient’s facial proportions, lip dynamics, and tooth morphology.
One of the most transformative procedures in cosmetic dentistry is the application of porcelain veneers. These ultra-thin ceramic shells are custom-fabricated to bond to the facial surfaces of the anterior teeth, correcting imperfections in color, shape, alignment, and spacing. The preparation for veneers is highly conservative, typically requiring the removal of only 0.3 to 0.5 millimeters of enamel. This minimal preparation ensures that the veneer bonds primarily to enamel, which provides a significantly stronger and more predictable adhesive interface than dentin. [4]
“The ultimate goal of aesthetic dentistry is to mimic nature so closely that the restorative work becomes imperceptible. This requires not only high-quality ceramics but a profound understanding of light transmission, surface texture, and gingival architecture.”
Advanced Ceramic Materials and Techniques
The choice of ceramic material is critical in aesthetic rehabilitations. Lithium disilicate (e.max) is highly favored for anterior restorations due to its exceptional translucency and ability to mimic the optical properties of natural enamel. For posterior restorations where occlusal forces are significantly higher, monolithic zirconia is often the material of choice due to its immense flexural strength.

In cases involving minor aesthetic defects, such as small chips, enamel hypoplasia, or slight contour irregularities, clinicians may utilize an innovative technique often referred to as liquid porcelain for teeth. This involves the application of highly filled, flowable ceramic-resin hybrids. These materials can be injected or brushed onto the tooth surface, offering a minimally invasive, highly polishable solution that seamlessly blends with the surrounding enamel. Understanding the nuances of line angle dental anatomy is essential when contouring these materials, as the precise placement of line angles dictates how light reflects off the tooth, ultimately determining its perceived width and length.
Oral Surgery and Prosthodontic Replacement
Surgical interventions and prosthodontic replacements are essential for managing non-restorable teeth, preserving alveolar bone, and re-establishing a stable, functional dental arch.
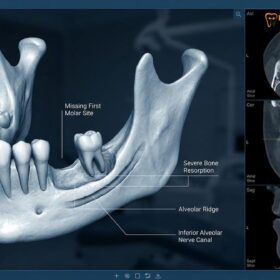
Despite the best preventive and restorative efforts, there are clinical scenarios where a tooth cannot be salvaged. Severe vertical root fractures, advanced periodontal bone loss, or massive carious lesions extending subgingivally may render a tooth non-restorable. In these instances, exodontia (tooth extraction) becomes a necessary surgical intervention to eliminate infection and prevent damage to adjacent anatomical structures.
Modern exodontia prioritizes atraumatic techniques. Rather than applying excessive force, clinicians utilize specialized instruments like periotomes and luxators to sever the periodontal ligament and gently elevate the tooth from its socket. This careful approach is vital for preserving the buccal bone plate, which is crucial for future prosthodontic rehabilitation. Patients undergoing these procedures at our clinic can expect rigorous protocols for safe outpatient oral surgery, ensuring minimal postoperative discomfort and optimal healing. [5]
Clinical Warning: Alveolar Osteitis (Dry Socket)
Following a dental extraction, the formation and retention of a blood clot within the socket is essential for normal healing. Dislodging this clot through vigorous rinsing, smoking, or using a straw can expose the underlying bone and nerves, leading to a painful condition known as alveolar osteitis, or dry socket. Strict adherence to postoperative instructions is mandatory to mitigate this risk.
Following an extraction, patients must be educated on how to prevent dry socket and manage the healing site. Once the extraction site has healed, or sometimes immediately following the extraction, the focus shifts to prosthodontic replacement. Failing to replace a missing tooth can lead to a cascade of negative consequences, including the supra-eruption of opposing teeth, the mesial drift of adjacent teeth, and progressive alveolar bone resorption.
The gold standard for replacing extracted teeth is the endosseous dental implant. Implants are biocompatible titanium or zirconia fixtures surgically placed into the jawbone, acting as artificial tooth roots. Through a physiological process called osseointegration, the bone fuses directly to the implant surface, providing unparalleled stability for a custom crown, bridge, or overdenture.
When to See a Doctor for Restorative Dental Care
Recognizing the early clinical signs of oral pathology is crucial for preventing extensive structural damage and avoiding complex surgical interventions. Patients should seek immediate evaluation from a qualified dental professional if they experience any of the following symptoms:
- Spontaneous Odontalgia: Unprovoked, throbbing tooth pain that awakens you from sleep is a strong indicator of irreversible pulpitis or an acute periapical abscess, requiring prompt endodontic evaluation.
- Prolonged Thermal Sensitivity: While mild, transient sensitivity to cold can be normal, severe pain that lingers for more than 10 to 15 seconds after the removal of a hot or cold stimulus suggests significant pulpal inflammation.
- Gingival Exudate or Swelling: The presence of purulent exudate (pus) along the gumline, accompanied by localized swelling or a persistent bad taste, indicates an active periodontal or endodontic infection.
- Tooth Mobility: Noticeable looseness in adult teeth is a severe red flag, often pointing to advanced periodontitis and significant loss of alveolar bone support.
- Fractured or Failing Restorations: A cracked tooth, a lost filling, or a loose crown compromises the biological seal, allowing bacteria to rapidly infiltrate the underlying dentin and pulp.
Timely intervention is the cornerstone of conservative dentistry. Delaying treatment for these symptoms inevitably leads to more invasive, time-consuming, and costly clinical procedures. A comprehensive evaluation utilizing digital radiography and vitality testing is necessary to determine the precise etiology of the symptoms and formulate an appropriate, evidence-based treatment plan.
Case Study: Full Mouth Rehabilitation at HCMC Dental Clinic
A structured full-mouth rehabilitation case demonstrates the seamless integration of periodontal, surgical, and prosthodontic disciplines to achieve total oral health and functional harmony.
To illustrate the profound impact of comprehensive general dentistry, we review a complex clinical case managed at HCMC Dental Clinic in Ho Chi Minh City. The patient, a 55-year-old male, presented with severe occlusal wear, multiple failing amalgam restorations, generalized moderate periodontitis, and the loss of several posterior teeth, which had led to a collapsed vertical dimension of occlusion (VDO).
Clinical Case Presentation: Complex Occlusal Rehabilitation
Chief Complaint: Difficulty masticating, chronic TMJ discomfort, and dissatisfaction with the aesthetic appearance of worn anterior teeth.
Diagnostic Phase: Dr. Nguyen Van Cuong conducted a comprehensive evaluation, including CBCT imaging, digital intraoral scanning, and a detailed occlusal analysis using articulated study models. The diagnosis confirmed a loss of VDO due to posterior bite collapse and severe attrition.
Treatment Execution:
1. Periodontal Phase: Full-mouth scaling and root planing to arrest active disease and establish healthy gingival margins.
2. Surgical Phase: Placement of three titanium dental implants in the posterior mandible to replace missing molars and restore posterior support.
3. Restorative Phase: Endodontic retreatment of two failing abutment teeth. Application of liquid porcelain for teeth to conservatively restore minor incisal edge defects on the lower anteriors.
4. Prosthodontic Phase: Fabrication of custom lithium disilicate crowns for the anterior maxilla to restore aesthetics and VDO, paired with monolithic zirconia crowns for the posterior implants to withstand heavy masticatory forces.
Clinical Outcome: The patient achieved a stable, mutually protected occlusion, complete resolution of TMJ symptomatology, and a highly aesthetic, natural-looking smile. The integration of multidisciplinary workflows ensured a predictable and long-lasting result.

This case underscores the necessity of a holistic approach. By addressing the foundational periodontal health first, establishing stable posterior support through implantology, and finally refining the aesthetics with advanced ceramics, the clinical team was able to deliver a life-changing outcome. It is this level of meticulous planning and execution that defines the highest echelon of dental care.
“Full-mouth rehabilitation is not merely about restoring teeth; it is about re-engineering the entire stomatognathic system to function in harmony. Every restoration must respect the biological width, the occlusal plane, and the neuromuscular pathways.”
For patients seeking this caliber of comprehensive care, understanding the clinical processes and maintaining open communication with your dental provider is essential. To learn more about how we maintain transparency and educate our patients, you can explore our approach to ethical dental ads and clinical marketing, which prioritizes patient education over aggressive sales tactics. If you are experiencing complex dental issues or simply require a thorough evaluation, we encourage you to schedule a consultation with our expert team at HCMC Dental Clinic.
Frequently Asked Questions
What is the difference between a general dentist and a prosthodontist?
A general dentist manages comprehensive primary oral care, including diagnostics, preventive therapies, and basic restorations. A prosthodontist is a specialist who completes additional years of training focused exclusively on complex dental prosthetics, full-mouth rehabilitation, and advanced aesthetic reconstructions. However, highly experienced general dentists often perform many prosthodontic procedures as part of a comprehensive care model.
How often should I undergo a clinical periodontal examination?
Clinical guidelines recommend a comprehensive periodontal evaluation at least once annually for healthy individuals. Patients with a history of periodontitis, systemic conditions like diabetes, or high plaque retention factors may require maintenance visits every three to four months. This frequent monitoring is critical to disrupt biofilm maturation and prevent the recurrence of active periodontal destruction.
Are composite resin fillings as durable as traditional amalgam?
Modern composite resins offer excellent durability and superior biomechanical integration due to advanced bonding protocols. While amalgam has high compressive strength, composites preserve more natural tooth structure and provide aesthetic harmony, making them the preferred choice for most clinical scenarios. The longevity of a composite restoration heavily depends on the clinician’s isolation technique and the patient’s occlusal forces.
What is the clinical protocol if a tooth cannot be saved?
If a tooth is deemed non-restorable, the clinical protocol involves atraumatic extraction to preserve the surrounding alveolar bone. This is typically followed by socket preservation grafting and the eventual placement of a dental implant or fixed bridge to restore function. Prompt replacement is vital to prevent the shifting of adjacent teeth and the continuous resorption of the jawbone.
Is teeth whitening safe for patients with enamel erosion?
Teeth whitening requires careful clinical assessment for patients with enamel erosion. Bleaching agents can penetrate compromised enamel, leading to severe hypersensitivity and potential pulpal irritation. A dentist must evaluate the enamel thickness and may recommend alternative aesthetic treatments, such as composite bonding or porcelain veneers, to safely achieve the desired cosmetic result without causing pain.
References
- Journal of the American Dental Association. Evidence-based clinical practice guideline on the nonrestorative treatments for carious lesions. (2018).
- Journal of Periodontology. Comprehensive periodontal therapy: a statement by the American Academy of Periodontology. (2011).
- Dental Materials. Polymerization shrinkage and biomechanical properties of advanced composite resins. (2020).
- International Journal of Prosthodontics. Long-term survival rates of porcelain veneers and full-coverage crowns. (2019).
- Journal of Oral and Maxillofacial Surgery. Atraumatic extraction techniques and alveolar ridge preservation protocols. (2021).