

Patients seeking dental crowns in Thailand or neighboring medical hubs receive world-class restorative care utilizing advanced CAD/CAM technology. These custom-milled prosthetics restore structural integrity to severely damaged teeth, offering exceptional functional durability and natural aesthetics at a fraction of Western clinical costs.
Clinical Summary:
Dental crown procedures in Southeast Asian medical hubs combine precision digital dentistry with high-strength biomaterials like monolithic zirconia and lithium disilicate. The clinical workflow involves comprehensive diagnostics, conservative tooth preparation, 3D intraoral scanning, and computerized milling. This approach ensures optimal marginal adaptation, biocompatibility, and long-term occlusal stability for patients requiring extensive restorative rehabilitation. Advanced adhesive protocols further enhance the retention and fracture resistance of these modern ceramic prostheses.
Key Takeaways:
- Modern restorative protocols utilize digital impressions for superior marginal fit and patient comfort.
- High-strength ceramics offer excellent biocompatibility, tissue integration, and fracture resistance.
- Treatment timelines are significantly reduced through in-house CAD/CAM milling technology.
- Proper occlusal adjustment prevents post-operative sensitivity and temporomandibular joint strain.
- Comprehensive clinical evaluation is mandatory to determine structural candidacy and pulpal health.
The Clinical Rationale for Restorative Dentistry in Southeast Asia
Southeast Asian dental hubs provide advanced prosthodontic rehabilitation using state-of-the-art digital workflows, ensuring clinical outcomes that meet or exceed rigorous international standards.
The landscape of global healthcare has shifted significantly, with Southeast Asia emerging as a premier destination for complex restorative dentistry. Patients requiring extensive prosthodontic work often face prohibitive costs in their home countries. By comparing local estimates—such as typical dentist perth prices—against the comprehensive, high-tech care available in regional medical hubs, patients discover that they can access superior biomaterials and specialized expertise without compromising on clinical safety or quality.
Modern clinics in this region operate under strict international sterilization protocols and utilize the exact same digital ecosystems found in top-tier Western practices. The integration of Cone Beam Computed Tomography (CBCT) and intraoral confocal microscopy allows for sub-millimeter precision in treatment planning. This technological parity ensures that advanced dental crown restorations are fabricated with ideal emergence profiles, promoting optimal gingival health and long-term structural stability.[1]

Furthermore, the concentration of highly trained prosthodontists in these hubs facilitates a multidisciplinary approach to patient care. Complex cases involving altered vertical dimension of occlusion (VDO) or severe parafunctional wear are managed collaboratively by endodontists, periodontists, and restorative specialists. This comprehensive diagnostic environment is crucial for ensuring that the underlying foundation of the tooth is sound before any definitive prosthesis is permanently cemented.
Diagnostic Criteria: When is a Crown Medically Necessary?
A dental crown is clinically indicated when a tooth suffers extensive structural compromise that cannot be reliably restored with direct composite or amalgam fillings.
The decision to place a full-coverage restoration is based on rigorous biomechanical principles. A tooth that has lost more than 50% of its coronal structure due to extensive caries, trauma, or previous large restorations is at a high risk of catastrophic fracture under normal masticatory forces. In these scenarios, a crown acts as a protective ferrule, encircling the remaining healthy dentin and distributing occlusal loads evenly across the root structure.
Endodontically treated teeth (teeth that have undergone root canal therapy) are particularly vulnerable. The removal of the pulpal tissue alters the moisture content and proprioceptive feedback of the tooth, making it more brittle and susceptible to vertical root fractures. Current endodontic guidelines strongly recommend full-coverage protection for posterior teeth following root canal treatment to ensure long-term survivability.[2]
“Preserving the natural ferrule—a minimum of 1.5 to 2 millimeters of healthy, parallel dentin above the gingival margin—is the most critical factor in the biomechanical success of a dental crown. Without this solid foundation, even the strongest ceramic materials are prone to debonding or root fracture under functional loading.”
— Dr. Nguyen Van Cuong, Lead Prosthodontist
Additionally, teeth exhibiting signs of Cracked Tooth Syndrome—characterized by sharp pain upon release of biting pressure—often require a crown to bind the fractured segments together and prevent the propagation of the crack into the pulp chamber. Patients experiencing post-operative chewing sensitivity with older, failing restorations are also prime candidates for evaluation and potential replacement with modern, well-sealed ceramic crowns.
Material Science: Choosing the Right Crown for Functional Longevity
Selecting the appropriate biomaterial depends on the tooth’s location, occlusal load, and the patient’s aesthetic requirements, ranging from layered ceramics to monolithic zirconia.
The evolution of dental biomaterials has largely phased out traditional metal-based restorations in favor of high-strength, biocompatible ceramics. The selection process is highly individualized, balancing the need for mechanical strength in the posterior segments with the demand for lifelike optical properties in the anterior aesthetic zone.
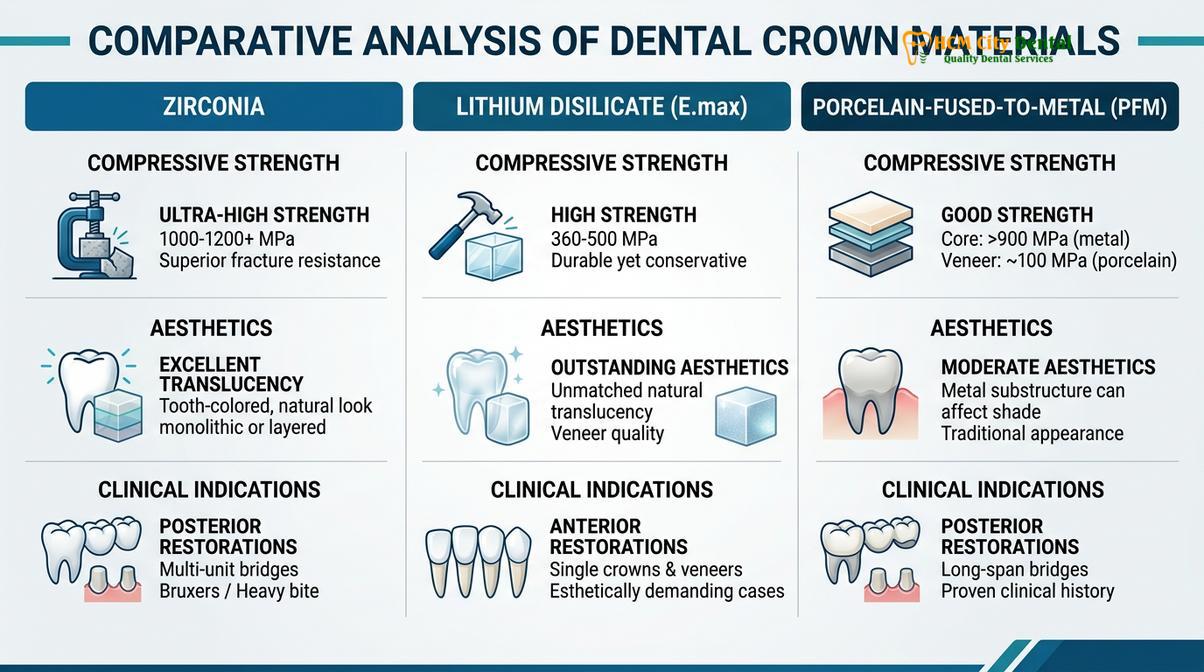
Lithium disilicate (often recognized under the brand name IPS e.max) is a glass-ceramic renowned for its exceptional translucency and ability to mimic the light-scattering properties of natural enamel. With a flexural strength of approximately 400-500 MPa, it is highly suitable for anterior crowns, premolars, and Porcelain Veneers. Its primary advantage lies in its ability to be adhesively bonded to the tooth structure, creating a monoblock effect that reinforces the underlying dentin.
For patients exhibiting heavy bruxism (teeth grinding) or requiring multi-unit restorations, Yttria-stabilized tetragonal zirconia polycrystal (Y-TZP) is the material of choice. Monolithic zirconia boasts a flexural strength exceeding 1000 MPa, making it virtually indestructible under normal physiological forces. Premium branded materials, including lava porcelain crowns, offer exceptional masking capabilities for severely discolored underlying tooth stumps while maintaining high fracture toughness. This robust nature also makes systems like the lava bridge dental framework highly reliable for replacing missing teeth across longer edentulous spans.[3]

While all-ceramic options dominate modern treatment plans, it is important to understand the safety of porcelain fused to metal restorations (PFM). PFM crowns utilize a cast or milled metal substructure layered with feldspathic porcelain. While they have a long history of clinical success, they often present aesthetic challenges, such as an opaque appearance or a dark line at the gingival margin if tissue recession occurs.
| Material Type | Flexural Strength | Aesthetic Quality | Primary Clinical Indication |
|---|---|---|---|
| Lithium Disilicate (E.max) | ~400 – 500 MPa | Exceptional (High Translucency) | Anterior teeth, premolars, high aesthetic demands. |
| Monolithic Zirconia | ~1000 – 1200 MPa | Good (Improving with newer generations) | Posterior molars, heavy bruxers, multi-unit bridges. |
| Layered Zirconia | ~800 – 1000 MPa (Core) | Excellent | Anterior crowns requiring both strength and masking. |
| Porcelain Fused to Metal (PFM) | Variable (Depends on alloy) | Moderate (Opaque core) | Cost-effective posterior restorations, deep subgingival margins. |
The Digital Workflow: From Preparation to Final Cementation
Contemporary prosthodontic treatment relies on CAD/CAM technology to transition from conservative tooth preparation to the precise milling and bonding of the final restoration.
The integration of Computer-Aided Design and Computer-Aided Manufacturing (CAD/CAM) has revolutionized the predictability and efficiency of crown fabrication. The clinical workflow begins with meticulous tooth preparation. The dentist utilizes specialized diamond burs to reduce the coronal structure, creating specific geometric forms—such as a heavy chamfer or modified shoulder margin—that provide adequate space for the ceramic material while ensuring a distinct finish line for the digital scanner to capture.
Tissue management is a critical step prior to scanning. Retraction cords impregnated with hemostatic agents are gently packed into the gingival sulcus to displace the soft tissue laterally, exposing the preparation margin clearly. This ensures that the final crown will have a precise marginal seal, preventing microleakage and secondary caries.[4]

Instead of traditional, uncomfortable silicone impression materials, an intraoral scanner captures thousands of images per second, stitching them together to create a highly accurate 3D virtual model of the patient’s dentition. This digital file is instantly transferred to the CAD software, where the restoration is designed. The software analyzes the opposing dentition, adjacent contact points, and dynamic occlusal pathways to generate a crown that integrates seamlessly into the patient’s bite.
Once the design is finalized, the data is sent to a CAM milling machine. A solid block of the chosen ceramic is carved into the exact shape of the crown within minutes. For materials like zirconia, the milled restoration must undergo a sintering process in a high-temperature furnace to achieve its final density and strength. The crown is then custom-stained and glazed to match the adjacent natural teeth, a crucial step in comprehensive smile makeovers.
The final phase is cementation. Depending on the material, the internal surface of the crown is treated—either etched with hydrofluoric acid and silanated for glass ceramics, or sandblasted and primed with 10-MDP for zirconia. The tooth is isolated, cleaned, and the crown is bonded using advanced dual-cure resin cements, creating a virtually impenetrable seal.
Clinical Case Study: Full Mouth Rehabilitation
Complex restorative cases require meticulous treatment planning, combining multiple prosthetic modalities to re-establish proper vertical dimension and occlusal harmony.
Patients presenting with severe generalized attrition, acid erosion, or multiple failing restorations often require a comprehensive approach rather than single-tooth dentistry. Rebuilding an entire arch or full mouth necessitates a deep understanding of gnathology and temporomandibular joint function.
Clinical Case Review: Severe Attrition Management
Patient Profile: A 55-year-old male presented to HCMC Dental Clinic in Ho Chi Minh City with severe occlusal wear secondary to nocturnal bruxism, resulting in a collapsed vertical dimension and hypersensitivity.
Diagnostic Phase: Comprehensive CBCT imaging, digital intraoral scanning, and a diagnostic wax-up were utilized to determine the ideal functional and aesthetic parameters. The treatment plan required opening the bite by 3mm to restore proper facial proportions and joint space.
Execution: The patient underwent phased treatment. The posterior segments were restored with high-strength monolithic zirconia crowns to withstand heavy masticatory forces. The anterior aesthetic zone was rehabilitated using layered lithium disilicate restorations. Understanding the differences between crowns and veneers allowed the clinical team to utilize conservative veneers on the lower anteriors where structural integrity permitted, while utilizing full crowns on the upper arch for maximum retention.
Outcome: The patient achieved a stable, mutually protected occlusion, complete resolution of hypersensitivity, and a highly aesthetic, natural-looking smile. A custom hard acrylic night guard was fabricated to protect the new restorations from future parafunctional habits.
Important Clinical Considerations and When to See a Doctor
While dental crowns boast a high success rate, they are complex medical devices placed in a harsh, bacteria-rich environment. Patients must be aware of potential complications and understand when immediate clinical intervention is necessary.
Important Clinical Considerations
Patients should seek prompt evaluation from a qualified dental professional if they experience any of the following symptoms post-cementation:
- Spontaneous, throbbing pain: This may indicate irreversible pulpitis, requiring endodontic therapy beneath the crown.
- Pain upon biting that does not subside: Often a sign of a “high” occlusal contact that requires minor adjustment to prevent trauma to the periodontal ligament.
- Foul odor or taste around the crown: This can indicate cement wash-out, marginal leakage, or recurrent decay beneath the restoration.
- Mobility of the crown: A loose crown compromises the seal and risks aspiration or swallowing; it must be recemented immediately.
During the interim phase of treatment, patients are often fitted with provisional (temporary) crowns made of bis-acrylic resin. These temporaries protect the prepared tooth and maintain space, but they are cemented with weak temporary cement. Patients must exercise caution, avoiding sticky or hard foods. For those undergoing treatment abroad, understanding how to handle emergencies, such as managing temporary restorations while traveling, is essential to prevent damage to the underlying tooth structure before the final prosthesis is delivered.
Post-Cementation Care and Lifespan Expectations
The long-term success of a fixed dental prosthesis relies heavily on meticulous daily oral hygiene and routine professional periodontal maintenance.
A common misconception is that a crowned tooth is immune to further dental disease. While the ceramic material itself cannot decay, the junction where the crown meets the natural tooth structure (the margin) is highly susceptible to plaque accumulation. If bacterial biofilm is allowed to mature at this interface, secondary caries can develop rapidly, often progressing undetected beneath the crown until catastrophic failure occurs.[5]
“The longevity of a restorative prosthesis is a shared responsibility. We utilize the most advanced biomaterials to create a precise, biocompatible seal, but the patient must maintain impeccable marginal hygiene. Without daily interdental cleaning, even the most perfectly executed crown is at risk of periodontal breakdown.”
— Dr. Nguyen Van Cuong, Lead Prosthodontist
Patients must adopt a rigorous home care routine, utilizing soft-bristled toothbrushes and non-abrasive fluoride toothpaste. Interdental cleaning is non-negotiable; the use of dental floss, interdental brushes, or water flossers is critical for disrupting biofilm at the gingival margin. Furthermore, routine professional prophylaxis and radiographic examinations every six months are necessary to monitor the integrity of the cement seal and the health of the surrounding bone.
When properly maintained, the clinical lifespan of dental crowns can easily exceed 10 to 15 years, with many restorations functioning flawlessly for decades. However, patients with a history of bruxism must wear a protective occlusal splint during sleep to prevent excessive wear or catastrophic fracture of the ceramic material.
Frequently Asked Questions
How long does the dental crown procedure take using digital workflows?
With modern CAD/CAM technology, a digital crown procedure can often be completed in one to two visits over a few days. The digital workflow eliminates the need for physical impressions, allowing the in-house laboratory to design, mill, and crystallize the ceramic restoration rapidly while maintaining precise marginal adaptation.
Is it painful to have a tooth prepared for a dental crown?
The preparation phase is performed under profound local anesthesia, ensuring the patient remains comfortable throughout the procedure. Post-operative mild tissue tenderness or transient thermal sensitivity may occur, but this is generally self-limiting and manageable with standard over-the-counter analgesics.
What is the difference between monolithic zirconia and lithium disilicate crowns?
Monolithic zirconia offers superior flexural strength, making it ideal for posterior teeth subjected to heavy occlusal forces. Lithium disilicate provides exceptional translucency and optical properties that closely mimic natural enamel, making it the preferred biomaterial for highly aesthetic anterior restorations.
Can a dental crown be placed on a tooth with severe decay?
A crown can be placed on a severely decayed tooth provided there is sufficient sound tooth structure remaining to establish a ferrule. If the decay extends subgingivally or compromises the pulp, preliminary treatments such as endodontic therapy and core build-ups are clinically mandatory before crown fabrication.

How should I care for my new ceramic dental crown?
Ceramic crowns require the same meticulous daily hygiene as natural teeth, including twice-daily brushing and daily interdental cleaning. Patients should avoid chewing on excessively hard objects like ice or hard candies, and those with bruxism are strongly advised to wear a custom occlusal guard during sleep.
For a personalized assessment of your restorative needs and to determine your candidacy for advanced ceramic prosthetics, schedule a comprehensive clinical consultation with the specialists at HCMC Dental Clinic in Ho Chi Minh City.
References
- Journal of Prosthetic Dentistry. Marginal adaptation and fracture resistance of CAD/CAM monolithic ceramic crowns. (2021).
- International Journal of Prosthodontics. Long-term clinical survival rates of lithium disilicate and zirconia restorations. (2020).
- Journal of Clinical Periodontology. Periodontal tissue response to subgingival restorative margins. (2019).
- Dental Materials. Adhesive cementation protocols for high-strength silica and non-silica based ceramics. (2022).
- Journal of Endodontics. The impact of the ferrule effect on the biomechanical behavior of endodontically treated teeth. (2018).



