A porcelain dental bridge is a fixed prosthetic device designed to seamlessly replace one or more missing teeth by anchoring an artificial tooth (pontic) to the adjacent natural teeth (abutments). This restorative solution restores masticatory function, prevents unwanted tooth shifting, and rehabilitates the patient’s natural smile aesthetics.
Clinical Summary:
The porcelain dental bridge remains a cornerstone of modern prosthodontics, offering a highly predictable, non-surgical method for replacing missing dentition. By utilizing advanced ceramics such as monolithic zirconia and lithium disilicate, contemporary bridges achieve exceptional fracture toughness and biomimetic optical properties. The clinical success of a fixed partial denture (FPD) relies heavily on precise abutment preparation, adherence to biomechanical principles like the Law of Ante, and meticulous management of the gingival emergence profile. While implantology has advanced significantly, bridges remain the treatment of choice when adjacent teeth require structural reinforcement or when anatomical limitations preclude surgical intervention. Long-term prognosis is intrinsically linked to the patient’s commitment to specialized interdental hygiene protocols and routine professional oversight.
Key Takeaways:
- Structural Function: Bridges utilize healthy adjacent teeth (abutments) to support a suspended artificial tooth (pontic), restoring the occlusal table.
- Material Evolution: Modern restorations favor high-strength ceramics like zirconia over traditional metal-based frameworks for superior aesthetics and biocompatibility.
- Clinical Workflow: The procedure involves precise tooth reduction, digital or elastomeric impressions, provisionalization, and final adhesive cementation.
- Maintenance Requirements: Specialized cleaning aids, such as floss threaders and water irrigators, are mandatory to prevent secondary caries and periodontal inflammation.
- Strategic Alternative: Bridges offer a rapid, non-surgical alternative to implants, particularly beneficial when adjacent teeth already exhibit significant structural compromise.
Understanding the Porcelain Dental Bridge: Clinical Definition and Mechanics
A porcelain bridge functions by utilizing healthy adjacent teeth as structural pillars to support a suspended prosthetic tooth, effectively bridging the edentulous gap and restoring occlusal harmony.
In the realm of restorative dentistry, the loss of even a single tooth initiates a cascade of detrimental biomechanical events. The adjacent teeth may drift or tilt into the edentulous space, while the opposing tooth may super-erupt due to the lack of occlusal contact. A porcelain dental bridge, clinically referred to as a Fixed Partial Denture (FPD), is engineered to halt this structural collapse. By creating a rigid, splinted unit, the bridge redistributes masticatory forces across the remaining dentition, preserving the integrity of the dental arch.
The Anatomy of a Fixed Partial Denture
To fully comprehend the mechanics of this restoration, one must understand its distinct anatomical components. The abutments are the natural teeth situated on either side of the missing tooth gap. These teeth serve as the foundational anchors for the prosthesis. During the clinical workflow, these teeth are circumferentially reduced to accommodate the thickness of the restorative material. The pontic is the artificial tooth that spans the empty space. It is meticulously contoured to mimic the natural emergence profile of a real tooth, resting gently against the gingival tissue to create the illusion of natural growth. Finally, the connectors are the rigid joints that fuse the pontic to the abutment crowns, ensuring the entire structure functions as a single, cohesive unit[1].

Biomechanical Considerations and the Law of Ante
The design and execution of a porcelain bridge are governed by strict biomechanical principles. One of the most critical foundational rules in prosthodontics is Ante’s Law. Formulated by Dr. Irwin H. Ante, this principle dictates that the combined pericemental area (root surface area) of the abutment teeth must be equal to or greater than the root surface area of the tooth or teeth being replaced. If this biomechanical threshold is not met, the abutment teeth will be subjected to excessive occlusal overload, leading to periodontal ligament trauma, mobility, and eventual failure of the restoration.
Furthermore, the span length of the bridge exponentially affects the stress placed on the connectors and abutments. According to the principles of physics applied to dental engineering, if the span of a bridge is doubled (e.g., replacing two missing teeth instead of one), the deflection (bending) of the bridge under chewing forces increases by a factor of eight. This necessitates the use of exceptionally rigid materials, such as high-density zirconia, and meticulous occlusal adjustment to ensure that lateral excursive forces do not compromise the cement seal or the ceramic framework.
Types of Porcelain Bridges in Modern Dentistry
Dental bridges are categorized into traditional, cantilever, Maryland, and implant-supported designs, each selected based on the specific anatomical, functional, and aesthetic requirements of the edentulous space.
The selection of a specific bridge design is not arbitrary; it is a highly individualized clinical decision based on a comprehensive diagnostic evaluation. Factors such as the location of the missing tooth, the periodontal health of the adjacent teeth, the patient’s occlusal scheme, and aesthetic demands all dictate the optimal prosthetic approach. For patients exploring comprehensive dental restoration guides, understanding these variations is crucial for informed consent.
Traditional Fixed Bridges
The traditional fixed bridge remains the most prevalent and biomechanically stable configuration. It involves creating full-coverage crowns for the teeth on both sides of the edentulous span, with a pontic suspended between them. This design provides maximum retention and resistance form, making it the gold standard for replacing posterior teeth where masticatory forces are highest. However, the primary drawback is the necessity for aggressive, irreversible reduction of healthy enamel and dentin on the abutment teeth.
Cantilever Bridges
A cantilever bridge is utilized when there is an adjacent tooth on only one side of the missing tooth gap. The pontic is supported by one or more abutments on a single side, acting as a lever arm. Due to the significant torque and rotational forces generated during chewing, cantilever bridges are generally contraindicated for posterior regions. They are most successfully employed in the anterior segment, such as replacing a missing lateral incisor by anchoring it solely to the robust canine tooth, thereby preserving the delicate central incisor from preparation.
Maryland (Resin-Bonded) Bridges
The Maryland bridge, or resin-bonded fixed partial denture, was developed as a conservative alternative to traditional bridges. Instead of full-coverage crowns, this design utilizes a pontic supported by thin metal or ceramic wings that are adhesively bonded to the lingual (tongue-facing) surfaces of the adjacent teeth. The preparation is minimal, often restricted to the enamel layer, preserving the structural integrity of the abutments. While highly conservative, Maryland bridges have a lower retention rate and are highly technique-sensitive regarding moisture control during cementation. They are primarily indicated for anterior single-tooth replacement in patients with favorable occlusion[2].
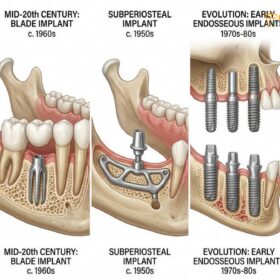
Implant-Supported Bridges
When multiple consecutive teeth are missing, or when the posterior abutment is absent (a free-end saddle situation), an implant-supported bridge is the treatment of choice. Instead of relying on natural teeth, titanium fixtures are surgically placed into the jawbone to serve as artificial roots. Once osseointegration is complete, the porcelain bridge is screwed or cemented onto the implant abutments. This approach preserves the remaining natural dentition and provides unparalleled stability for extensive spans.
| Bridge Type | Primary Indication | Tooth Preparation Required | Relative Durability & Stability |
|---|---|---|---|
| Traditional Fixed | Single or multiple missing teeth with healthy adjacent abutments. | High (Full circumferential reduction). | Excellent (Gold standard for posterior forces). |
| Cantilever | Missing anterior teeth (e.g., lateral incisors) with one strong adjacent abutment. | High (Full reduction on one side only). | Moderate (Susceptible to rotational torque). |
| Maryland (Resin-Bonded) | Missing anterior teeth requiring conservative treatment. | Minimal (Lingual enamel etching and slight reduction). | Fair (Higher risk of debonding). |
| Implant-Supported | Multiple missing teeth or absence of posterior abutments. | None (Relies on surgical implant placement). | Exceptional (Preserves adjacent natural teeth). |
Material Science: Why Porcelain is the Gold Standard
Modern dental bridges utilize advanced ceramics like monolithic zirconia and lithium disilicate, offering superior fracture toughness, biocompatibility, and optical properties compared to traditional metal-based restorations.
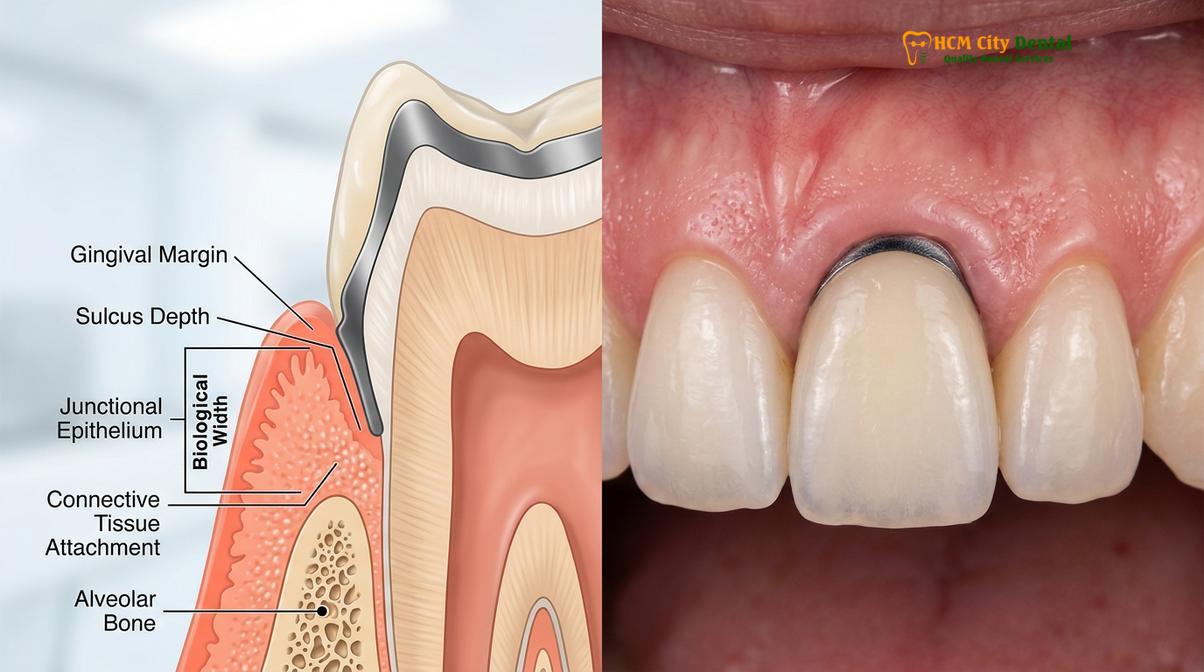
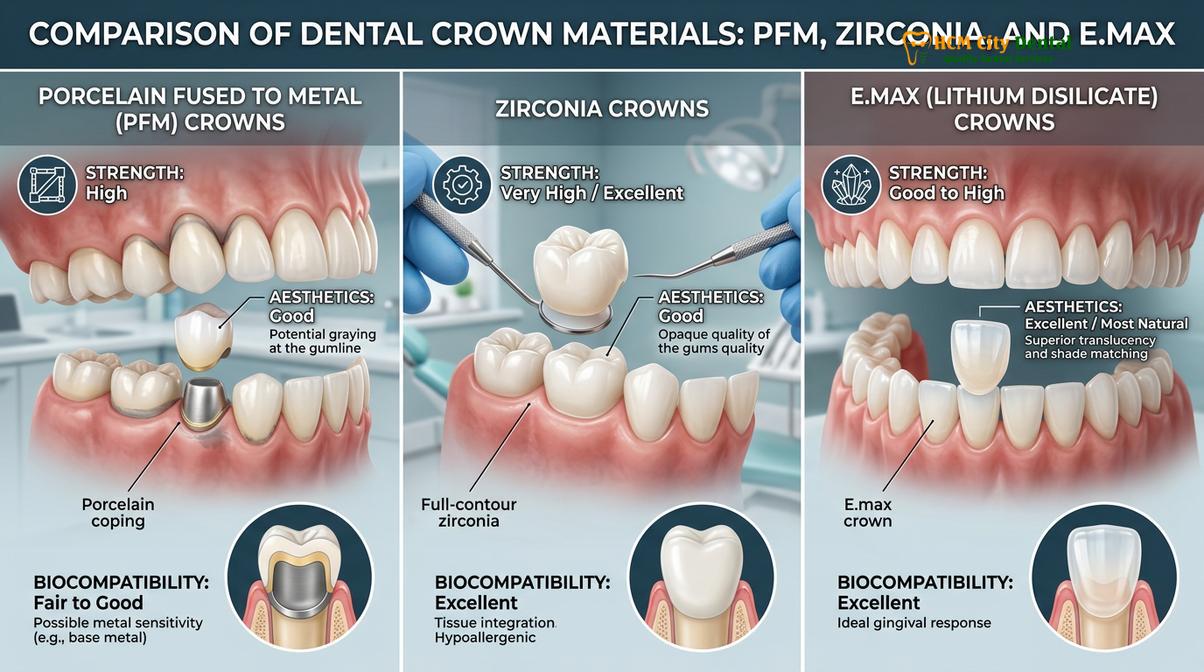
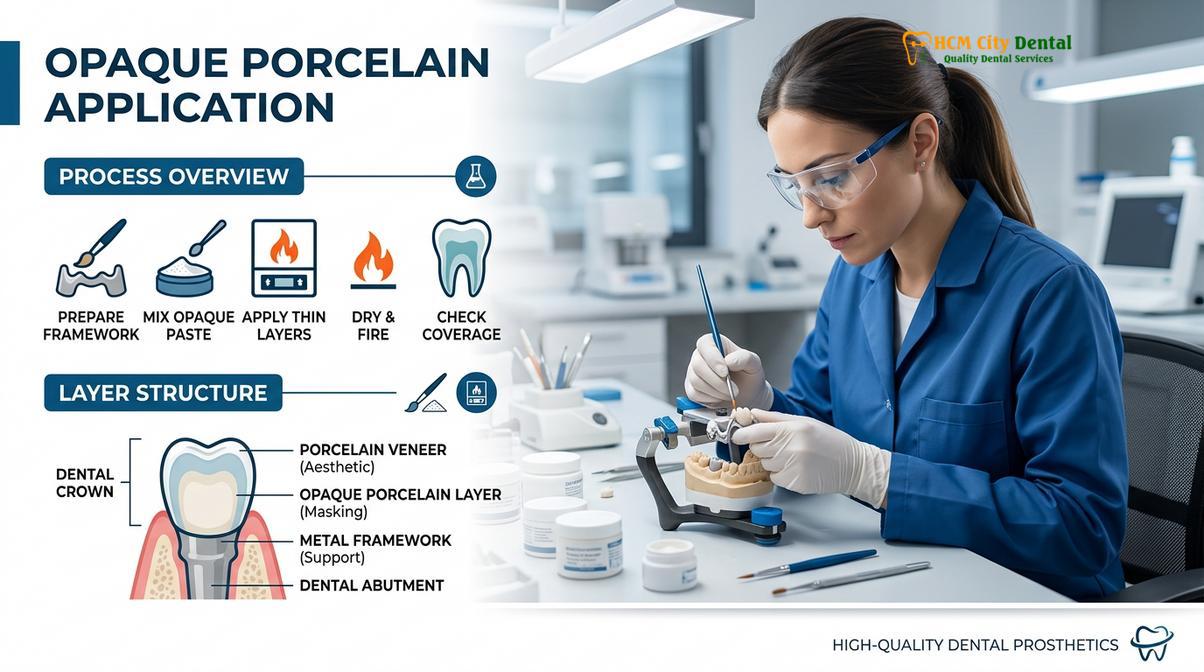
The evolution of dental biomaterials has fundamentally transformed the fabrication of fixed prosthetics. Historically, the structural demands of a bridge necessitated the use of a cast metal framework, which was then veneered with feldspathic porcelain for aesthetics. While functional, these Porcelain-Fused-to-Metal (PFM) restorations presented significant aesthetic challenges, most notably the opaque masking required to hide the metal and the eventual exposure of a dark “gray line” at the gingival margin if tissue recession occurred.
The Rise of Monolithic Zirconia
Today, Yttria-stabilized tetragonal zirconia polycrystal (Y-TZP) has become the material of choice for posterior bridges. Zirconia is a polymorphic material that undergoes a phenomenon known as “phase transformation toughening.” When a micro-crack begins to propagate through the material, the crystalline structure locally transforms, expanding in volume and effectively clamping the crack shut. This gives zirconia an exceptionally high flexural strength (often exceeding 1000 MPa), allowing it to withstand the immense compressive forces of the molar region without the need for a metal substructure.
Early generations of zirconia were highly opaque and visually unappealing. However, advancements in material science have led to the development of highly translucent, multi-layered zirconia blanks. These modern materials exhibit a natural gradient of color and translucency from the cervical margin to the incisal edge, rivaling the aesthetics of natural enamel while maintaining robust structural integrity.
Lithium Disilicate (E.max) for Anterior Aesthetics
For anterior bridges where aesthetic demands are paramount and occlusal forces are lower, lithium disilicate (commonly known by the brand name IPS e.max) is frequently utilized. Lithium disilicate offers unparalleled optical properties, mimicking the light transmission, opalescence, and fluorescence of natural teeth. While its flexural strength (around 400-500 MPa) is lower than zirconia, it is more than sufficient for short-span anterior bridges, particularly when adhesively bonded to the underlying tooth structure.
“The transition from metal-ceramic to all-ceramic restorations represents a paradigm shift in prosthodontics. Materials like monolithic zirconia not only eliminate the aesthetic compromise of metal margins but also exhibit superior soft tissue biocompatibility, significantly reducing plaque accumulation and gingival inflammation around the pontic site.”
The Clinical Workflow: Step-by-Step Procedure
The fabrication of a porcelain bridge involves a meticulous multi-step protocol, encompassing diagnostic imaging, precise abutment preparation, provisionalization, and final adhesive cementation.
The successful execution of a porcelain bridge requires absolute precision at every stage of the clinical workflow. Any deviation in preparation geometry, impression accuracy, or cementation protocol can compromise the longevity of the restoration. Patients traveling for dental tourism options in Southeast Asia often seek clinics that utilize advanced CAD/CAM technology to streamline this process without sacrificing clinical excellence.
Initial Diagnostic Evaluation and 3D Imaging
The process begins with a comprehensive clinical and radiographic examination. Cone Beam Computed Tomography (CBCT) and periapical radiographs are utilized to assess the bone levels, root morphology, and endodontic status of the proposed abutment teeth. The clinician evaluates the occlusal plane, the curve of Spee, and the curve of Wilson to ensure the new prosthesis will function harmoniously within the patient’s dynamic bite.
Tooth Preparation and Impression Taking
Once the treatment plan is finalized, profound local anesthesia is administered. The abutment teeth are meticulously prepared using high-speed diamond burs. The goal is to create a specific geometric form—typically a chamfer or modified shoulder margin—that provides adequate space (usually 1.5 to 2.0 mm of occlusal clearance) for the ceramic material while ensuring a precise marginal seal. The preparation must possess adequate axial wall height and a slight convergence angle (taper) to provide retention and resistance against dislodging forces.
Following preparation, the gingival tissue is carefully retracted using specialized cords or hemostatic pastes to expose the preparation margins fully. A highly accurate impression is then captured. While traditional elastomeric materials (like polyvinyl siloxane) are still used, modern clinics increasingly rely on intraoral digital scanners. These optical impressions create a highly accurate 3D virtual model, eliminating the discomfort of traditional putty and allowing for immediate digital transmission to the dental laboratory.
Clinical Case Review: Posterior Rehabilitation
A 45-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City with a missing mandibular first molar and heavily restored adjacent teeth. Dr. Nguyen Van Cuong conducted a comprehensive occlusal analysis and determined that a traditional fixed bridge was the optimal solution. The adjacent premolar and second molar were prepared with precise chamfer margins. Utilizing intraoral digital scanning and CAD/CAM technology, a monolithic high-translucency zirconia bridge was milled and sintered. The final restoration provided exceptional marginal adaptation, restored the patient’s masticatory efficiency, and seamlessly blended with the natural dentition, demonstrating the efficacy of modern digital prosthodontics.
Provisionalization (The Temporary Bridge)
Because the fabrication of the final ceramic bridge takes time (unless utilizing rapid dental crown restorations via in-house milling), a temporary bridge made of bis-acryl composite resin is fabricated and cemented with temporary cement. This provisional restoration is critical; it protects the exposed dentin from thermal sensitivity, prevents the abutment teeth from shifting, and helps shape the gingival tissue (emergence profile) around the pontic site to ensure a natural appearance for the final restoration.
Final Cementation and Occlusal Adjustment
Upon completion of the final porcelain bridge, the patient returns for the delivery appointment. The temporary bridge is carefully removed, and the abutment teeth are thoroughly cleaned and decontaminated. The final bridge is tried in to verify marginal fit, interproximal contacts, and aesthetic integration.
Once verified, the intaglio (internal) surface of the bridge is treated based on the material—zirconia requires sandblasting and a primer containing MDP monomer, while lithium disilicate requires hydrofluoric acid etching and silanization. The teeth are isolated, and the bridge is permanently bonded using a dual-cure resin cement or a resin-modified glass ionomer. Finally, the occlusion is meticulously checked using articulating paper to ensure there are no premature contacts or working/non-working interferences that could fracture the ceramic[3].
Advantages and Disadvantages: A Balanced Clinical Perspective
While porcelain bridges provide rapid aesthetic and functional rehabilitation without surgery, they inherently require the irreversible alteration of adjacent natural teeth and present unique hygiene challenges.
In clinical practice, informed consent requires a transparent discussion of both the benefits and the inherent limitations of any proposed treatment. A porcelain dental bridge is a highly successful modality, but it is not without its compromises.
Functional and Aesthetic Benefits
The primary advantage of a fixed bridge is its ability to rapidly restore function and aesthetics without the need for invasive surgical procedures or extended healing times. Unlike removable partial dentures, a fixed bridge is securely cemented in place, providing a stable and confident chewing experience. Furthermore, if the adjacent abutment teeth already possess large, failing restorations or require full-coverage protection due to endodontic treatment, a bridge elegantly solves multiple clinical problems simultaneously. The aesthetic outcomes achievable with modern ceramics, particularly when combined with treatments like Porcelain Veneers on adjacent teeth, are virtually indistinguishable from natural dentition.
Potential Drawbacks and Structural Limitations
The most significant disadvantage of a traditional bridge is the biological cost to the abutment teeth. The aggressive reduction of healthy enamel and dentin increases the risk of pulpal trauma; studies indicate that a percentage of abutment teeth may eventually require root canal therapy due to the stress of preparation and subsequent microleakage.
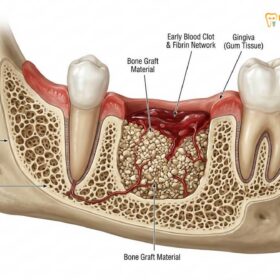
Additionally, because a bridge pontic rests above the gums and does not penetrate the bone, it does not provide the internal mechanical stimulation necessary to maintain alveolar bone volume. Over time, the bone beneath the pontic will undergo physiological resorption (atrophy), which can lead to an unesthetic gap between the artificial tooth and the gum line. Finally, the splinted nature of the bridge complicates oral hygiene, requiring specialized techniques to prevent plaque accumulation.
Clinical Warning: The Risk of Secondary Caries
The margins where the porcelain bridge meets the natural tooth structure are highly susceptible to plaque accumulation. If meticulous interdental hygiene is not maintained, cariogenic bacteria will colonize these margins, leading to secondary tooth decay beneath the crowns. Because the bridge masks the underlying tooth, this decay can progress silently and extensively before it is detected, often resulting in the catastrophic failure of the entire restoration and the potential loss of the abutment teeth.
Porcelain Bridge vs. Dental Implants: Making the Right Choice
Choosing between a bridge and an implant depends on the structural integrity of adjacent teeth, patient bone volume, and individual preferences regarding surgical intervention and treatment timelines.
The debate between fixed partial dentures and single-tooth implants is one of the most common discussions in restorative dentistry. Both modalities boast high success rates, but their biomechanical approaches are fundamentally different.
Bone Preservation and Adjacent Tooth Integrity
Dental implants are widely considered the premier standard of care for single-tooth replacement because they are independent restorations. An implant replaces both the root and the crown of the missing tooth, transmitting chewing forces directly into the alveolar bone. This internal stimulation preserves bone volume according to Wolff’s Law of bone remodeling. Most importantly, an implant leaves the adjacent natural teeth completely untouched, preserving their structural integrity and vitality.
Conversely, a bridge relies entirely on the adjacent teeth for support. If the adjacent teeth are pristine and virgin (unrestored), preparing them for a bridge is considered biologically aggressive. However, if the adjacent teeth are heavily decayed, fractured, or already have large fillings, a bridge becomes a highly logical choice, as those teeth require crown coverage regardless.
“The paradigm of tooth replacement has shifted towards implantology to preserve adjacent dentition. However, the fixed dental bridge remains an indispensable tool in the prosthodontic armamentarium, particularly in cases of severe alveolar ridge deficiency where bone grafting is contraindicated, or when rapid, non-surgical rehabilitation is mandated by the patient’s systemic health or timeline.”
Timeline and Treatment Complexity
Treatment timelines differ drastically. An implant requires surgical placement, followed by a healing period of 3 to 6 months for osseointegration before the final crown can be attached. A porcelain bridge, however, can typically be completed in just two appointments spanning a few weeks. For international patients planning a dental stay in Vietnam, the rapid turnaround of a fixed bridge is often a decisive factor.
Long-Term Maintenance and Lifespan of a Dental Bridge
The longevity of a porcelain bridge relies heavily on meticulous home care, including the use of specialized interdental cleaning aids to prevent plaque accumulation beneath the pontic and around the margins.
While dental ceramics are impervious to decay, the natural tooth structure supporting the bridge is not. The long-term prognosis of a fixed partial denture is directly proportional to the patient’s oral hygiene compliance and the stability of their occlusal forces.
Specialized Oral Hygiene Protocols
Because the crowns and the pontic are fused together, traditional dental floss cannot be passed vertically between the teeth. Patients must utilize specialized tools to clean the critical area beneath the pontic and around the abutment margins.
- Floss Threaders and Superfloss: These tools allow the patient to thread the floss horizontally under the bridge, sweeping away plaque and food debris from the gingival surface of the pontic and the interproximal walls of the abutments.
- Interdental Brushes: Sized appropriately for the embrasure spaces, these brushes are highly effective at disrupting biofilm at the cervical margins.
- Oral Irrigators (Water Flossers): Pulsating water streams are excellent adjuncts for flushing out loose debris and reducing gingival inflammation, though they do not replace the mechanical friction of flossing[4].
Preventing Secondary Caries and Periodontal Issues
Routine professional maintenance is non-negotiable. Patients with fixed bridges should undergo professional prophylaxis and clinical examinations every six months. The clinician will evaluate the integrity of the cement seal, probe the periodontal pockets around the abutments, and assess the occlusion for any signs of traumatic interference. Patients who exhibit signs of bruxism (teeth grinding) should be fitted with a custom occlusal guard to protect the ceramic from fracture and prevent excessive stress on the abutment roots[5].
When to See a Doctor
While porcelain bridges are highly durable, they are subject to the harsh environment of the oral cavity. Early detection of complications is critical to salvaging the restoration and the underlying teeth. You should schedule an immediate evaluation with a qualified professional, such as an consulting an English-speaking dental professional, if you experience any of the following symptoms:
- Mobility or Looseness: If the bridge feels loose or shifts during chewing, the cement seal may have washed out on one or both abutments. This requires immediate recementation to prevent rapid decay underneath the loose crown.
- Localized Pain or Sensitivity: Sharp pain upon biting or lingering sensitivity to hot and cold can indicate pulpal inflammation, a fractured abutment root, or recurrent decay approaching the nerve.
- Gingival Inflammation or Bleeding: Persistent redness, swelling, or bleeding around the margins of the bridge suggests periodontal disease or a biological width violation that requires professional intervention.
- Foul Odor or Taste: A persistent bad taste or odor emanating from the bridge area is a strong indicator of microleakage, where bacteria and food particles are trapped beneath a compromised margin.
- Ceramic Fracture: Any visible chipping or cracking of the porcelain should be evaluated to ensure the structural integrity of the framework is not compromised and to polish any sharp edges that could irritate the tongue or mucosa.
For patients seeking expert evaluation of existing restorations or considering new prosthodontic work, Dr. Nguyen Van Cuong and the team at HCMC Dental Clinic in Ho Chi Minh City provide comprehensive diagnostic assessments. Utilizing advanced 3D imaging and a meticulous clinical approach, they ensure that every restorative treatment plan is tailored to the patient’s unique anatomical and functional needs, delivering premium dental care for expats and local residents alike.

Frequently Asked Questions
How long does a porcelain dental bridge typically last?
A porcelain dental bridge typically lasts between 10 to 15 years, depending on the material used and the patient’s oral hygiene. With meticulous home care, regular professional prophylaxis, and a stable occlusal bite, high-strength zirconia bridges can often exceed this lifespan. However, the underlying abutment teeth remain susceptible to secondary caries and periodontal disease, which are the primary causes of premature bridge failure.
Is the procedure for getting a dental bridge painful?
The procedure for getting a dental bridge is highly controlled and virtually painless, as it is performed under profound local anesthesia. Patients may experience mild thermal sensitivity or gingival tenderness for a few days following the preparation phase and the placement of the temporary bridge. Over-the-counter analgesics are usually sufficient to manage any transient post-operative discomfort.
Can a porcelain bridge be whitened if it stains?
No, dental porcelain and ceramic materials do not respond to traditional peroxide-based teeth whitening treatments. While high-quality dental ceramics are highly resistant to intrinsic staining, surface accumulation of plaque or extrinsic stains from coffee and tobacco can occur. These surface stains must be removed through professional dental polishing rather than chemical bleaching.
What is the difference between a traditional bridge and a Maryland bridge?
A traditional bridge requires the aggressive reduction of adjacent teeth to accommodate full-coverage crowns, whereas a Maryland bridge is a conservative alternative that uses metal or porcelain wings bonded to the lingual (back) surfaces of the adjacent teeth. Traditional bridges offer superior structural stability for posterior chewing forces, while Maryland bridges are typically reserved for replacing low-stress anterior teeth.
How do I clean underneath my porcelain dental bridge?
Cleaning underneath a porcelain bridge requires specialized interdental aids, as traditional flossing cannot pass through the connected crowns. Patients must use floss threaders, Superfloss, or interdental brushes to navigate beneath the artificial tooth (pontic) and sweep away plaque. Additionally, oral irrigators (water flossers) are highly recommended to flush out debris and maintain the health of the underlying gingival tissues.
References
- Journal of Prosthetic Dentistry. Biomechanical principles of fixed partial dentures and abutment preparation. (2021).
- International Journal of Prosthodontics. Long-term survival rates of monolithic zirconia vs. porcelain-fused-to-metal bridges. (2020).
- Journal of Clinical Periodontology. Periodontal response to pontic design and gingival embrasure contours. (2019).
- Journal of the American Dental Association. Clinical evaluation of resin-bonded fixed dental prostheses. (2022).
- Dental Materials. Phase transformation toughening and optical properties of modern dental ceramics. (2018).