

Functional braces are specialized orthodontic appliances designed to correct jaw discrepancies, such as severe overbites or underbites, by modifying skeletal growth. Typically used in growing children and adolescents, these devices harness natural muscle forces to guide the upper and lower jaws into optimal alignment while simultaneously shifting teeth.
Clinical Summary:
Functional brace teeth therapy, often referred to as dentofacial orthopedics, is a cornerstone of interceptive orthodontics aimed at correcting skeletal imbalances before a patient reaches physical maturity. By posturing the mandible into a more favorable position, these appliances stimulate adaptive changes in the temporomandibular joint (TMJ) and surrounding musculature. Treatment is highly time-sensitive, yielding the best results during the pubertal growth spurt. While removable appliances like the Twin Block require strict patient compliance, fixed options like the Herbst appliance offer continuous force application. Successful functional therapy frequently eliminates the need for future orthognathic surgery, laying a stable foundation for Phase II detailing with fixed brackets or clear aligners.
Key Takeaways:
- Functional braces primarily target skeletal jaw discrepancies rather than just crooked teeth.
- Treatment is most effective during the adolescent growth spurt (typically ages 11-14).
- Appliances can be removable (e.g., Twin Block) or fixed (e.g., Herbst appliance).
- Strict compliance of 22-24 hours of daily wear is mandatory for removable types.
- Functional therapy is usually Phase I, followed by Phase II fixed braces or aligners.
What Are Functional Braces and How Do They Work?
Functional braces correct skeletal malocclusions by posturing the lower jaw into a new position, stimulating adaptive growth in the temporomandibular joint and surrounding musculature. This orthopedic effect resolves bite discrepancies before skeletal maturity is reached.
In the realm of orthodontics, treatments are generally divided into two categories: those that move teeth (orthodontics) and those that modify facial growth (dentofacial orthopedics). Functional brace teeth therapy falls heavily into the latter category. These appliances are engineered to address significant skeletal disharmonies, most notably Class II malocclusions, where the upper jaw is positioned too far forward, or the lower jaw is positioned too far back (retrognathic mandible) [1].
The core mechanism of a functional appliance relies on altering the neuromuscular environment of the oral cavity. When a patient wears the appliance, it forces the lower jaw to posture forward (or backward, in the case of Class III correctors) to close the mouth or chew. This continuous, altered posture stretches the muscles of mastication, particularly the lateral pterygoid muscle. The tension generated by these stretched muscles is transmitted to the skeletal structures, specifically the condyle of the temporomandibular joint (TMJ) and the glenoid fossa [2].
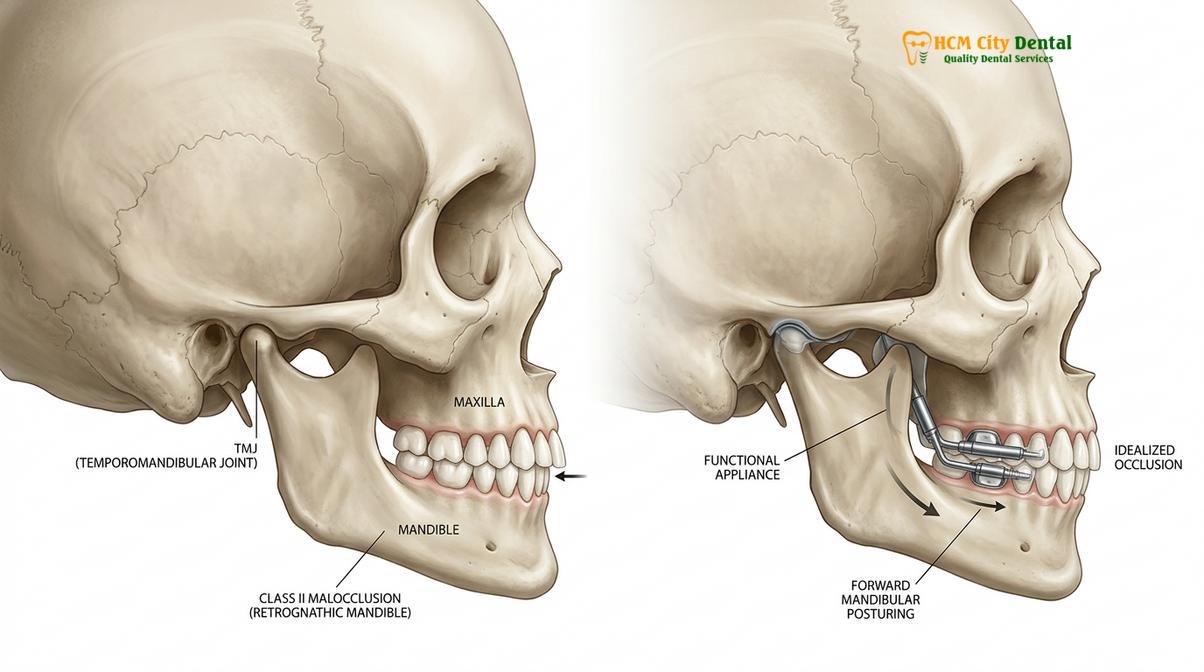
Over time, this sustained mechanical strain stimulates endochondral ossification—the biological process of bone formation—at the head of the condyle. Simultaneously, remodeling occurs within the glenoid fossa, allowing the mandible to permanently adapt to its new, forward position. Furthermore, functional appliances exert reciprocal forces on the dentition; as the lower jaw is guided forward, a distalizing (backward) force is applied to the upper teeth, helping to reduce severe overjets (protruding upper front teeth).
“Functional appliances do not merely tip teeth; they fundamentally alter the neuromuscular environment, allowing the mandible to achieve its full genetic growth potential while restricting excessive maxillary protrusion.”
It is crucial to understand that the success of this biological mechanism is entirely dependent on the patient’s growth status. Once the skeletal sutures have fused and the pubertal growth spurt has concluded, the ability to achieve significant orthopedic changes diminishes drastically. Therefore, timing is the most critical variable in functional appliance therapy.
The Biological Mechanism of Growth Modification
Growth modification relies on the viscoelastic properties of the periodontal ligament and the adaptive capacity of condylar cartilage. By altering muscular forces, functional appliances trigger cellular remodeling that permanently changes jaw relationships.
To fully appreciate how functional brace teeth operate, one must delve into the cellular and biomechanical responses triggered by these devices. The human face grows in three dimensions: transverse (width), sagittal (front-to-back), and vertical (height). Functional appliances primarily target the sagittal dimension, though some designs incorporate expansion screws to address transverse deficiencies simultaneously.
When the mandible is postured forward by an appliance like a Twin Block, the condyle is pulled out of its resting position in the articular fossa. This displacement creates a localized environment of tension and altered blood flow. According to the widely accepted “functional matrix theory,” bone grows in response to the functional demands placed upon it by surrounding soft tissues [3]. The altered muscular activity upregulates the expression of specific growth factors, such as Insulin-like Growth Factor (IGF) and Vascular Endothelial Growth Factor (VEGF), within the condylar cartilage.
These biochemical signals accelerate the proliferation of chondrocytes (cartilage cells), which eventually ossify into mature bone, effectively lengthening the mandible. Concurrently, the appliance utilizes the teeth as anchorage. The viscoelastic nature of the periodontal ligament (PDL) allows for the transmission of these orthopedic forces to the alveolar bone, resulting in the desired dental tipping that complements the skeletal correction. This dual action—skeletal growth modification combined with dentoalveolar compensation—is what makes functional therapy so effective in correcting severe overjet and establishing a harmonious facial profile.
Types of Functional Orthodontic Appliances
Orthodontists utilize various functional appliances, categorized into removable devices like the Twin Block and fixed systems such as the Herbst appliance, each selected based on the patient’s specific skeletal diagnosis and compliance levels.
The orthodontic armamentarium includes a wide array of functional appliances, each with unique design features suited for specific clinical scenarios. The choice of appliance depends on the severity of the malocclusion, the patient’s facial growth pattern (vertical vs. horizontal growers), and the anticipated level of patient compliance.
Removable Functional Appliances
Removable appliances are highly popular due to their ease of fabrication and the ability for patients to maintain optimal oral hygiene. However, their efficacy is entirely dependent on the patient wearing them for the prescribed 22-24 hours a day.
- The Twin Block: Developed by Dr. William Clark, this is arguably the most widely used functional appliance globally. It consists of separate upper and lower acrylic plates featuring bite blocks that interlock at a 70-degree angle. When the patient closes their mouth, the angled blocks force the lower jaw to slide forward. Its split design allows for relatively normal speech and eating, making it highly tolerated by patients.
- The Bionator: A single-piece acrylic appliance that fits over both the upper and lower teeth. It is less bulky than older designs like the Activator and is designed to guide the eruption of teeth while posturing the jaw forward. It is particularly useful for patients with deep bites.
- The Frankel Appliance: Unlike tooth-borne appliances, the Frankel is primarily tissue-borne. It features large acrylic shields that sit in the vestibule (between the teeth and cheeks). These shields hold the facial muscles away from the developing jaws, allowing for natural expansion and forward growth, utilizing the periosteal pull to stimulate bone formation.

Fixed Functional Appliances
For patients who struggle with compliance, or for those nearing the end of their growth spurt where continuous force is critical, fixed functional appliances are the treatment of choice. These are cemented or bonded to the teeth and cannot be removed by the patient.
- The Herbst Appliance: A robust system of metal sleeves and plungers attached to the upper and lower molars. It acts like an artificial joint, physically preventing the lower jaw from moving backward while allowing opening and lateral movements. It is highly effective and guarantees 24/7 force application [4].
- The MARA (Mandibular Anterior Repositioning Appliance): Similar in concept to the Herbst but less bulky. It uses metal “elbows” attached to the upper molars that guide the lower jaw forward upon closure. It is often preferred for its durability and reduced risk of breakage.
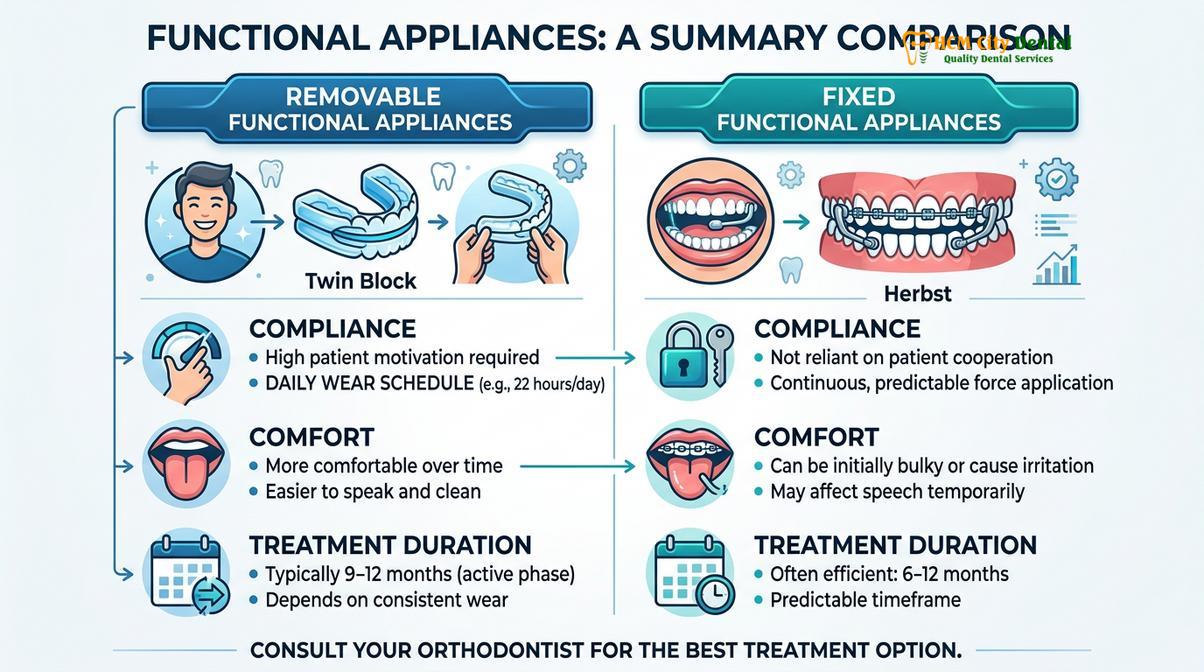
| Feature | Removable (e.g., Twin Block) | Fixed (e.g., Herbst) |
|---|---|---|
| Compliance Dependency | Extremely High (Patient must wear 22+ hours/day) | Low (Cemented in place, works 24/7) |
| Oral Hygiene | Easier (Appliance can be removed for brushing) | More Challenging (Requires specialized flossing) |
| Speech Impact | Moderate initially, adapts within a week | Minimal impact on speech |
| Risk of Breakage | Moderate (If dropped or mishandled) | Higher (If hard/sticky foods are consumed) |
| Clinical Indication | Highly motivated growing patients | Non-compliant patients or late adolescents |
Clinical Workflow: From Diagnosis to Appliance Fitting
The treatment protocol begins with comprehensive cephalometric radiography and 3D intraoral scanning to analyze skeletal discrepancies, followed by precise bite registration to fabricate a custom appliance that postures the jaw correctly.
The successful implementation of functional brace teeth requires meticulous planning and precise clinical execution. The workflow begins with a comprehensive orthodontic consultation, which is a critical component of comprehensive general dentistry and specialized orthodontic care.
At HCMC Dental Clinic in Ho Chi Minh City, Dr. Nguyen Van Cuong emphasizes the importance of accurate diagnostics before initiating any growth modification therapy. The diagnostic phase involves capturing high-resolution intraoral and extraoral photographs, panoramic X-rays, and, most importantly, a lateral cephalometric radiograph. The cephalometric X-ray allows the orthodontist to trace specific anatomical landmarks and measure angles (such as SNA, SNB, and ANB) to determine exactly how much of the malocclusion is skeletal versus dental.
Once a Class II skeletal discrepancy is confirmed and the patient is deemed to be in an active growth phase (often verified by examining the cervical vertebrae maturation on the X-ray), the physical records are taken. Modern clinics utilize 3D intraoral scanners to create highly accurate digital models of the patient’s dentition, eliminating the need for uncomfortable traditional putty impressions.

The most critical step in the fabrication process is the “construction bite.” The orthodontist guides the patient’s lower jaw forward into the desired therapeutic position—usually an edge-to-edge incisor relationship—and records this position using a rigid bite registration material. This record dictates exactly how the laboratory will construct the appliance to ensure the correct amount of forward posturing.
Upon delivery of the appliance, the orthodontist carefully checks the fit, retention, and the patient’s ability to close into the new postured position. Adjustments are made to the acrylic or metal clasps to ensure comfort. Patients are then scheduled for regular review appointments, typically every 6 to 8 weeks, to monitor growth, adjust expansion screws if present, and selectively trim the acrylic to guide the eruption of permanent teeth.
Patient Experience: Adaptation, Diet, and Oral Hygiene
Patients typically experience a brief adaptation period involving altered speech and increased salivation, requiring strict adherence to dietary guidelines and rigorous oral hygiene protocols to prevent appliance damage and dental caries.
Embarking on functional appliance therapy requires a significant commitment from both the patient and their parents. The initial adaptation period, usually lasting 3 to 7 days, can be challenging. Because the appliance introduces a large volume of acrylic or metal into the oral cavity and forces the jaw into an unfamiliar position, patients will immediately notice changes in their speech. Words containing “s” or “th” sounds may be difficult to pronounce initially. Reading aloud for 15-20 minutes a day rapidly accelerates speech adaptation.
Additionally, the brain initially interprets the appliance as food, leading to a temporary overproduction of saliva. This hypersalivation subsides within a few days as the sensory receptors adapt. Mild muscular aching in the cheeks and jaw joints is also common and perfectly normal; it is a sign that the muscles are stretching and the orthopedic forces are working. Over-the-counter analgesics can be used if necessary, though the discomfort is rarely severe.
Clinical Warning: Poor compliance or frequent removal of removable functional appliances significantly prolongs treatment time and compromises skeletal correction. If the appliance breaks or causes severe soft tissue ulceration, patients must contact their orthodontist immediately rather than waiting for the next scheduled appointment to prevent relapse.
Dietary modifications are essential, particularly for fixed functional appliances. Patients must strictly avoid hard, sticky, or chewy foods—such as caramels, hard candies, ice, and crusty bread—which can dislodge cemented bands or bend the metal mechanisms. For removable appliances like the Twin Block, patients are often encouraged to eat with the appliance in place to maximize the functional forces during mastication, though this requires practice and softer foods initially.
Oral hygiene cannot be overstated. Removable appliances must be taken out and brushed meticulously twice a day with a soft brush and mild soap. Toothpaste should be avoided on the appliance as its abrasives can scratch the acrylic, creating microscopic havens for bacteria. For fixed appliances, patients must use interdental brushes, floss threaders, and water flossers to navigate around the complex hardware and prevent decalcification (white spot lesions) and gingivitis.
Phase II Orthodontics: Transitioning to Fixed Braces or Clear Aligners
Functional appliance therapy is typically the first phase of a comprehensive treatment plan, followed by a second phase utilizing fixed brackets or clear aligners to achieve precise dental detailing and final occlusal interdigitation.
It is a common misconception that functional braces are the entirety of the orthodontic journey. In reality, functional therapy is almost always “Phase I” of a two-phase treatment protocol. The primary goal of Phase I is to correct the underlying skeletal foundation and reduce the severity of the overjet. However, functional appliances are relatively blunt instruments when it comes to individual tooth positioning [5].
Once the functional appliance has successfully guided the jaws into a Class I relationship (where the upper and lower jaws are harmoniously aligned), the patient transitions to Phase II. This phase focuses on the micro-aesthetics and precise interdigitation of the teeth. Depending on the clinical requirements and patient preference, Phase II can be executed using traditional metal braces, self-ligating bracket systems, or modern clear aligner therapy.
During the transition period, the orthodontist must carefully manage the “dual bite” phenomenon. As the functional appliance is phased out, the patient may instinctively try to bite back into their old, retrognathic position. To prevent this skeletal relapse, the functional appliance is often worn at night as a retainer while the fixed braces or aligners begin to settle the teeth into their new, permanent interlocking positions. This interlocking of the upper and lower teeth acts as a natural biological retainer for the newly grown jaw position.
Clinical Case Study: A 12-year-old patient presented at HCMC Dental Clinic in Ho Chi Minh City with a severe 10mm overjet, a retrognathic mandible, and difficulty closing his lips. Dr. Nguyen Van Cuong initiated Phase I treatment using a removable Twin Block appliance for 10 months, successfully reducing the overjet to 3mm and significantly improving the facial profile. Phase II involved 14 months of fixed orthodontics to detail the bite and align the arches, resulting in a perfectly functional smile without the need for future orthognathic surgery or permanent tooth extractions. This highlights the profound impact of timely clinical orthodontic transformations.
“The success of two-phase orthodontic treatment relies heavily on capturing the pubertal growth spurt, transforming a potentially surgical skeletal discrepancy into a manageable, non-invasive orthodontic case.”
For older adolescents or adults who missed the window for growth modification, functional appliances are generally contraindicated. In these cases, orthodontists must explore cost-effective adult orthodontic options that focus on dental camouflage (moving teeth to mask the skeletal discrepancy) or collaborate with oral surgeons for orthognathic jaw surgery.
When to See an Orthodontist for Jaw Discrepancies
Early detection is the linchpin of successful functional orthodontic treatment. The American Association of Orthodontists recommends that every child receive their first orthodontic evaluation by the age of 7. While functional appliances are typically not deployed until ages 10 to 13 (coinciding with the pubertal growth spurt), early screening allows the orthodontist to monitor facial growth and intervene at the precise biological moment.
Parents should be vigilant for signs that may indicate a developing skeletal discrepancy. These include:
- Severe Overjet: The upper front teeth protrude significantly beyond the lower teeth, increasing the risk of dental trauma during falls or sports.
- Receding Chin: A noticeably weak or retrognathic lower jaw profile.
- Deep Bite: The upper front teeth completely cover the lower front teeth when biting down, sometimes causing the lower teeth to bite into the roof of the mouth.
- Mouth Breathing: Chronic open-mouth posture, which can alter the resting position of the tongue and negatively influence jaw growth.
- Difficulty Chewing or Biting: Inability to incise food properly due to the gap between the upper and lower front teeth.

If any of these signs are present, a comprehensive evaluation is highly recommended. Delaying assessment until all permanent teeth have erupted often means missing the critical window for growth modification, potentially limiting treatment options to extractions or jaw surgery later in life. A timely consultation ensures that all conservative, growth-harnessing avenues are explored based on thorough clinical diagnostics.
Frequently Asked Questions
Are functional braces painful to wear?
Functional braces are not typically painful, though patients may experience mild muscular ache and dental tenderness during the first few days of adaptation. Over-the-counter analgesics and a soft diet can effectively manage this initial, temporary discomfort. As the facial muscles stretch and adapt to the new jaw posture, the aching rapidly subsides, usually within a week.
How many hours a day must a removable functional appliance be worn?
For optimal skeletal modification, removable functional appliances like the Twin Block must be worn for 22 to 24 hours a day. They should only be removed for contact sports, swimming, and rigorous oral hygiene routines. Wearing the appliance part-time or only at night is insufficient to trigger the necessary biological bone remodeling and will result in treatment failure.
Can adults successfully use functional orthodontic appliances?
Functional appliances are generally ineffective for skeletal correction in adults because their facial growth sutures have fully fused. Adult jaw discrepancies typically require orthognathic surgery or camouflage orthodontics to achieve functional and aesthetic improvements. Attempting to use functional appliances in non-growing adults can lead to unwanted tipping of the teeth and potential damage to the temporomandibular joint.
How should I clean my removable functional appliance?
Clean the appliance twice daily using a soft-bristled toothbrush and non-abrasive liquid soap or specialized retainer cleaner. Avoid using hot water or harsh toothpaste, as these can warp the acrylic base and degrade the metal components. When not in the mouth, the appliance should always be stored in its protective hard case to prevent accidental breakage or loss.
Will functional braces permanently change my facial profile?
Yes, functional braces can significantly improve a patient’s facial profile by encouraging the lower jaw to grow forward, reducing the appearance of a receding chin. This orthopedic change enhances facial harmony when treatment occurs during the pubertal growth spurt. The skeletal changes achieved during this active growth phase are generally stable and permanent, provided proper retention protocols are followed.
References
- American Journal of Orthodontics and Dentofacial Orthopedics. The clinical effectiveness of functional appliances in Class II malocclusion. (2020).
- European Journal of Orthodontics. Skeletal and dental effects of the Twin Block appliance: A systematic review. (2019).
- Journal of Clinical Orthodontics. Neuromuscular adaptations during functional appliance therapy. (2021).
- Angle Orthodontist. Long-term stability of Herbst appliance treatment in growing patients. (2018).
- British Orthodontic Society. Guidelines for the use of functional appliances in interceptive orthodontics. (2022).



