

To numb your mouth, dentists primarily use local anesthetics like Lidocaine or Articaine, administered via injection. Before the shot, a topical numbing gel containing Benzocaine is often applied to the gums to minimize needle discomfort, ensuring a virtually painless experience during fillings, extractions, or root canals.
Clinical Summary:
Dental anesthesia is a cornerstone of modern dentistry, allowing for complex procedures to be performed with minimal patient discomfort. The process typically involves a two-step protocol: the application of a topical anesthetic to desensitize the mucosal surface, followed by the injection of a local anesthetic agent. While Novocaine was historically the standard, contemporary practices rely on advanced amide anesthetics such as Lidocaine, Articaine, Mepivacaine, and Bupivacaine. These agents work by temporarily blocking voltage-gated sodium channels in nerve membranes, preventing the transmission of pain signals to the brain. To enhance efficacy and duration, vasoconstrictors like epinephrine are frequently added to the anesthetic solution. Understanding the pharmacology, administration techniques, and potential side effects of these medications empowers patients to approach their dental treatments with confidence and reduced anxiety.
Key Takeaways:
- Modern dentists use amide anesthetics like Lidocaine and Articaine, having completely phased out the older, allergy-prone Novocaine.
- A topical numbing gel is routinely applied before the injection to significantly reduce the sensation of the needle pinch.
- Epinephrine is commonly mixed with anesthetics to constrict blood vessels, prolonging the numbing effect and minimizing bleeding.
- Dental numbing typically lasts 1 to 3 hours for the tooth itself, while soft tissues like the lips and tongue may remain numb for up to 5 hours.
- Alternative sedation methods, such as nitrous oxide or IV sedation, are available for patients experiencing severe dental anxiety.
The Science of Dental Anesthesia: What Do Dentists Use to Numb You?
Dentists rely on a specific class of medications called local anesthetics, primarily Lidocaine and Articaine, which temporarily block nerve signals to prevent pain during dental procedures.
The foundation of painless dentistry lies in the precise application of local anesthetics. When patients ask what dentists use to numb them, they are often surprised to learn that the infamous “Novocaine” has not been used in mainstream dentistry for decades. Novocaine, an ester-based anesthetic, was prone to causing allergic reactions and took a considerable amount of time to take effect. Today, the dental profession utilizes a superior class of drugs known as amide anesthetics[1].
Local anesthetics function through a highly specific pharmacological mechanism. When injected near a nerve bundle, the anesthetic molecules diffuse through the nerve membrane and bind to voltage-gated sodium channels. By blocking these channels, the medication prevents sodium ions from entering the nerve cell. Without the influx of sodium, the nerve cannot depolarize, meaning it cannot generate or transmit the electrical impulses that the brain interprets as pain. This blockade is entirely reversible, allowing normal sensation to return once the body metabolizes the drug.
The modern dental anesthetic arsenal includes several distinct formulations, each selected based on the patient’s medical history and the specific requirements of the procedure:
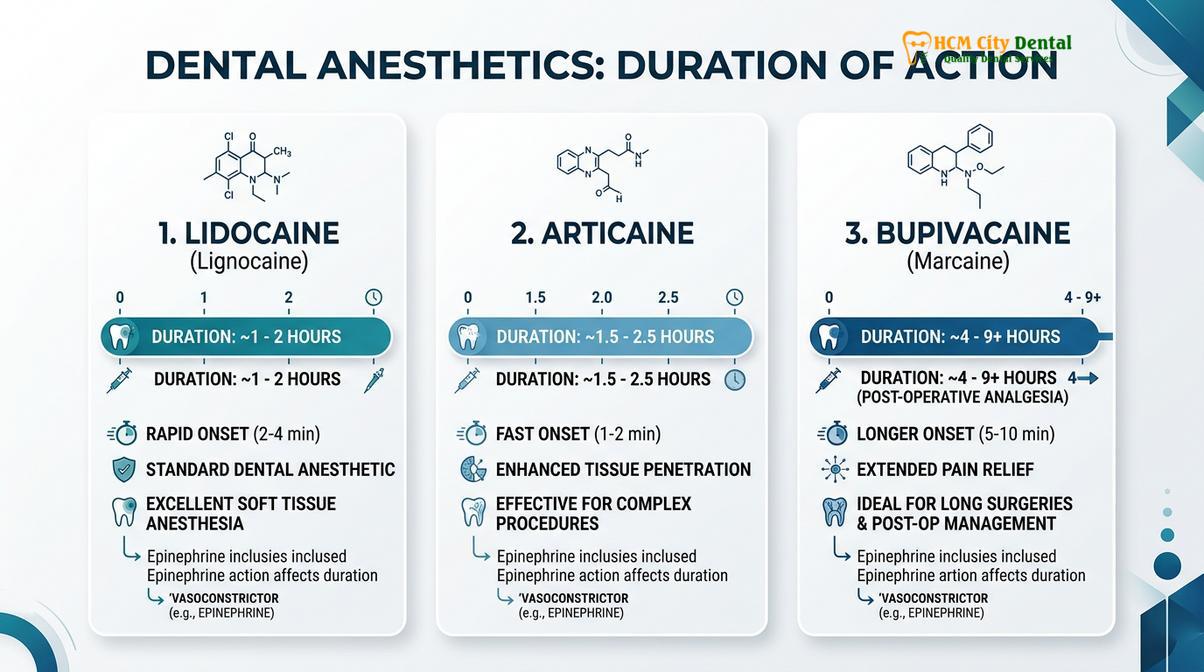
- Lidocaine (Xylocaine): Introduced in the mid-20th century, Lidocaine remains the gold standard in dental anesthesia. It is highly effective, acts quickly, and has a well-documented safety profile. It is typically formulated as a 2% solution with epinephrine.
- Articaine (Septocaine): Articaine has gained immense popularity, particularly for General Dentistry procedures. It contains a thiophene ring, which makes it highly lipid-soluble. This unique chemical structure allows Articaine to diffuse through dense cortical bone more effectively than Lidocaine, making it exceptionally useful for numbing lower teeth without always requiring a full nerve block[2].
- Mepivacaine (Carbocaine): Mepivacaine is often used as a 3% plain solution, meaning it does not contain epinephrine. It is the anesthetic of choice for patients who have cardiovascular contraindications to vasoconstrictors or for short procedures where prolonged numbness is unnecessary.
- Bupivacaine (Marcaine): Bupivacaine is a long-acting anesthetic. While Lidocaine may provide pulpal (tooth) anesthesia for about an hour, Bupivacaine can keep a tooth numb for up to three hours and soft tissues numb for eight hours or more. It is primarily reserved for extensive oral surgeries or for managing post-operative pain.
- Prilocaine (Citanest): Prilocaine is another alternative that causes less vasodilation than Lidocaine. It is metabolized differently (in the lungs and liver) and is often used when epinephrine needs to be limited.

Topical vs. Injectable Anesthetics: The Two-Step Numbing Process
The numbing process typically involves two steps: applying a topical benzocaine gel to desensitize the gum surface, followed by an injectable anesthetic to achieve deep, profound numbness.
One of the most common fears associated with dental visits is the anticipation of the injection. To mitigate this, dental professionals employ a two-step protocol designed to make the administration of local anesthesia as comfortable as possible. This approach addresses both the superficial mucosal tissue and the deep nerve structures.
Step 1: Topical Anesthesia
Before any needle approaches the mouth, the dentist will dry the target area with gauze and apply a topical anesthetic. The most common agent used is 20% Benzocaine, which comes in various flavors like cherry, mint, or bubblegum. Topical anesthetics are formulated as gels, ointments, or sprays. Because they are applied directly to the non-keratinized oral mucosa, they absorb quickly and numb the outermost 2 to 3 millimeters of tissue. This surface numbing significantly reduces, and often entirely eliminates, the sharp “pinch” associated with the initial needle penetration.
Step 2: Injectable Anesthesia
Once the surface is numb, the dentist proceeds with the injectable anesthetic. The delivery system consists of a sterile syringe, a disposable ultra-fine needle, and a glass carpule (cartridge) containing the anesthetic solution. The dentist injects the fluid slowly. Interestingly, the mild discomfort some patients feel during an injection is rarely from the needle itself; rather, it is the sensation of volume expansion as the anesthetic fluid enters the confined space of the gum tissue. Administering the fluid slowly minimizes this pressure sensation.
To help patients understand the differences between the injectable options, the following table outlines the most common anesthetics used in clinical practice:
| Anesthetic Agent | Brand Name Example | Contains Epinephrine? | Pulpal Duration (Tooth) | Primary Clinical Use |
|---|---|---|---|---|
| Lidocaine 2% | Xylocaine | Yes (Usually 1:100,000) | 60 minutes | Standard fillings, crowns, routine extractions. |
| Articaine 4% | Septocaine | Yes (1:100,000 or 1:200,000) | 60 – 75 minutes | Infiltrations in dense bone, endodontics. |
| Mepivacaine 3% | Carbocaine | No | 20 – 40 minutes | Patients with cardiac issues, short procedures. |
| Bupivacaine 0.5% | Marcaine | Yes (1:200,000) | 90 – 180 minutes | Complex oral surgery, prolonged post-op pain relief. |
Types of Dental Injections: Infiltration vs. Block Anesthesia
Depending on the tooth’s location, dentists use infiltration injections to numb individual upper teeth or nerve block injections to numb an entire quadrant of the lower jaw.
The anatomical differences between the upper jaw (maxilla) and the lower jaw (mandible) dictate the technique the dentist must use to achieve profound anesthesia. The bone of the upper jaw is relatively porous and thin, whereas the bone of the lower jaw is dense and thick. This anatomical variance requires two primary injection techniques: infiltrations and nerve blocks.
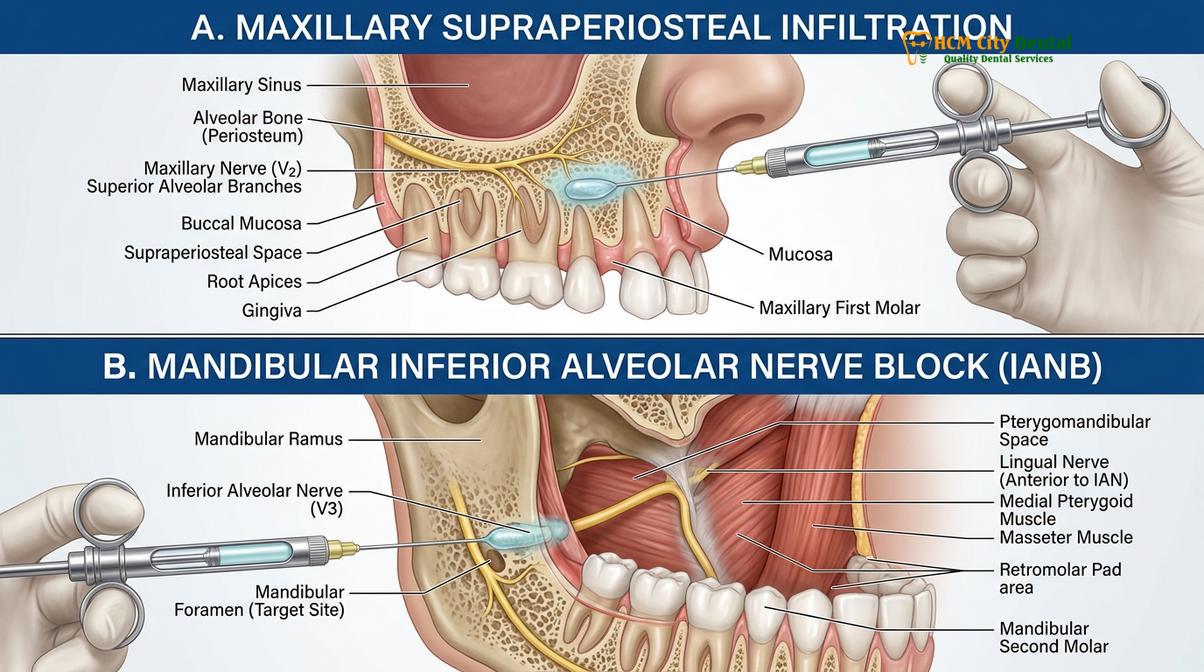
Supraperiosteal Infiltration
Infiltration anesthesia is primarily used for the upper teeth. The dentist injects the anesthetic solution into the soft tissue near the apex (root tip) of the target tooth. Because the maxillary bone is porous, the anesthetic fluid easily diffuses through the bone to reach the nerve endings of that specific tooth. Infiltrations are highly localized, meaning only the tooth being treated and the immediately adjacent gum tissue will feel numb. This technique is also frequently used in pediatric dentistry, as children’s bones are less dense, allowing for easier diffusion.
Inferior Alveolar Nerve Block (IANB)
Numbing the lower teeth presents a greater clinical challenge due to the dense cortical bone of the mandible, which prevents anesthetic from simply soaking through. To overcome this, dentists utilize the Inferior Alveolar Nerve Block. Instead of injecting near the tooth, the dentist targets the main nerve trunk before it enters the jawbone. The injection is placed in the back of the mouth, near the hinge of the jaw. When successful, an IANB numbs an entire quadrant of the lower jaw, including the teeth, the bone, the lower lip, and half of the tongue on that side.
Supplemental Injection Techniques
In cases where standard infiltrations or blocks do not provide sufficient numbness—often due to severe inflammation or anatomical anomalies—dentists employ supplemental techniques. The Periodontal Ligament (PDL) injection involves depositing anesthetic directly into the space between the tooth root and the surrounding bone. Intraosseous injections deliver the anesthetic directly into the spongy bone surrounding the tooth. These advanced techniques ensure that even the most difficult-to-numb teeth can be treated comfortably.
The Role of Epinephrine (Vasoconstrictors) in Dental Numbing
Epinephrine is a vasoconstrictor mixed into dental anesthetics to narrow blood vessels, which keeps the numbing medication localized, prolongs its effect, and minimizes bleeding during treatment.
When examining the contents of a dental anesthetic cartridge, one will almost always find a vasoconstrictor, most commonly epinephrine (adrenaline). The addition of epinephrine is a critical component of modern dental pharmacology, serving three vital purposes[5].
First, epinephrine constricts the blood vessels in the immediate area of the injection. Local anesthetics are inherently vasodilators, meaning they naturally cause blood vessels to widen. If injected without epinephrine, the body’s bloodstream would rapidly carry the anesthetic away from the tooth, resulting in a very short duration of numbness and a higher risk of systemic toxicity. By constricting the vessels, epinephrine traps the anesthetic at the site, significantly prolonging the duration of profound anesthesia.
Second, by keeping the anesthetic localized, epinephrine reduces the peak concentration of the drug in the systemic bloodstream, thereby enhancing the overall safety profile of the injection.
Third, the vasoconstrictive properties of epinephrine are invaluable for achieving hemostasis (controlling bleeding). During procedures that involve the gums or bone, such as extractions or deep cleanings, the localized reduction in blood flow provides the dentist with a clear, dry field of vision, which is essential for precise clinical work.
“The inclusion of epinephrine in local anesthetics revolutionized our ability to perform complex, time-consuming procedures. However, we must always evaluate a patient’s cardiovascular history. For patients with uncontrolled hypertension or severe arrhythmias, we adjust our protocols and utilize epinephrine-free alternatives like Mepivacaine to ensure absolute safety.”
— Dr. Nguyen Van Cuong, Clinical Director
It is not uncommon for patients to experience a sudden, temporary racing heart or a feeling of jitteriness immediately after receiving a dental injection. This is a direct physiological response to the small amount of epinephrine entering the bloodstream. While it can feel alarming, it is a harmless “fight or flight” response that typically subsides within three to five minutes as the body naturally metabolizes the adrenaline.
Overcoming Anesthetic Failure: The “Hot Tooth” Phenomenon
Achieving profound anesthesia in an infected tooth requires advanced techniques, as inflammation alters tissue pH and makes standard numbing injections less effective.
One of the most challenging scenarios in clinical dentistry is achieving profound numbness in a tooth suffering from irreversible pulpitis—commonly referred to as a “hot tooth.” Patients often report that despite receiving multiple injections, they still feel sharp pain when the dentist attempts to begin the procedure. This failure is not due to a lack of skill, but rather a complex biochemical interaction caused by infection[4].
Healthy human tissue has a physiological pH of approximately 7.4. Local anesthetics are formulated as weak bases. When injected into healthy tissue, a portion of the anesthetic molecules remains un-ionized (lipid-soluble), allowing them to easily penetrate the nerve membrane and block the pain signals. However, when a tooth is severely infected or inflamed, the surrounding tissue becomes highly acidic, often dropping to a pH of 5.5 or lower.
In this acidic environment, the vast majority of the anesthetic molecules become ionized (water-soluble). Ionized molecules cannot penetrate the lipid barrier of the nerve membrane. This phenomenon, known as “ion trapping,” means the anesthetic is physically present around the nerve but is biochemically incapable of entering it to provide numbness.
To overcome a “hot tooth,” dentists utilize several advanced strategies. They may use Articaine, which has superior bone penetration capabilities. They may employ supplemental PDL or intraosseous injections to bypass the acidic tissue and deliver the anesthetic directly to the nerve apex. In some modern practices, dentists use anesthetic buffering—adding sodium bicarbonate to the anesthetic cartridge immediately before injection to raise its pH, allowing it to work effectively even in inflamed tissues.
How Long Does Dental Numbing Last and What to Expect After
A standard dental numbing shot typically lasts one to two hours for the tooth itself, while the surrounding lips and soft tissues may remain numb for three to five hours.
Understanding the timeline of dental anesthesia helps patients plan their day post-treatment. The duration of numbness is categorized into two distinct phases: pulpal anesthesia (the numbness of the tooth nerve) and soft tissue anesthesia (the numbness of the gums, lips, and tongue).
For a standard Lidocaine or Articaine injection with epinephrine, pulpal anesthesia typically lasts between 60 to 90 minutes. This provides ample time for the dentist to complete most routine procedures, such as placing fillings or preparing crowns. However, the soft tissue anesthesia lasts significantly longer, often persisting for 3 to 5 hours. If a long-acting agent like Bupivacaine is used, soft tissue numbness can last up to 8 hours or more.

During the period of soft tissue numbness, patients must exercise extreme caution. The lack of sensation makes it incredibly easy to accidentally bite the lip, cheek, or tongue while chewing or speaking. These self-inflicted bite injuries can cause severe swelling and ulceration that takes days to heal. For this reason, dentists strongly advise against eating any solid foods requiring chewing until the numbness has completely dissipated. Consuming hot beverages should also be avoided, as the inability to gauge temperature can lead to severe burns.
For patients who find prolonged numbness intolerable—perhaps because they have a speaking engagement or a business meeting immediately after their appointment—dentists can sometimes administer a reversal agent. Phentolamine mesylate (marketed as OraVerse) is an injection given at the end of the procedure that dilates the blood vessels, rapidly flushing the anesthetic away from the site and cutting the duration of soft tissue numbness in half.
Managing Dental Anxiety: Sedation Options Beyond Local Numbing
For patients with severe dental phobia, local anesthetics are often combined with sedation methods like nitrous oxide, oral sedatives, or intravenous sedation to ensure complete relaxation.
While local anesthetics are highly effective at eliminating pain, they do nothing to alleviate the psychological anxiety, fear, or claustrophobia that many patients experience in the dental chair. When considering comprehensive care, **dentists recommend** discussing anxiety levels openly before any procedure begins. Depending on **where do dentists work**—whether in a hospital setting, a specialized surgical center, or a modern private practice like HCMC Dental Clinic—a variety of sedation options are available to complement local numbing.
The **most successful dentists** understand that treating the patient’s mind is just as important as treating the tooth. Sedation dentistry bridges this gap:
- Nitrous Oxide (Laughing Gas): This is a mild inhaled sedative that induces a state of deep relaxation and euphoria. It takes effect quickly and wears off within minutes after the gas is turned off, allowing the patient to drive themselves home. It is excellent for mild to moderate anxiety.
- Oral Conscious Sedation: Patients are prescribed a sedative medication (usually a benzodiazepine like Halcion or Valium) to take an hour before their appointment. This produces a moderate level of sedation. The patient remains awake and responsive but is highly relaxed and often has little memory of the procedure.
- Intravenous (IV) Sedation: Administered directly into the bloodstream, IV sedation provides deep conscious sedation. It is highly controllable and is typically reserved for severe dental phobia, complex oral surgeries, or patients with strong gag reflexes.
It is important to note that sedation does not replace local anesthesia. Even under IV sedation, the dentist must still administer numbing shots to block the pain receptors locally. The sedation simply ensures the patient is entirely relaxed and unaware of the injections being administered.
Clinical Case Study: Achieving Profound Anesthesia in a Complex Case
Advanced anesthetic techniques, including the use of Articaine and supplemental periodontal ligament injections, are crucial for ensuring patient comfort during complex endodontic treatments.
Clinical Case Study: Managing Irreversible Pulpitis
Patient Profile: A 42-year-old male presented to HCMC Dental Clinic in Ho Chi Minh City with severe, throbbing pain in his lower right molar (Tooth #46). Clinical diagnostics confirmed irreversible pulpitis requiring immediate endodontic therapy.
Clinical Challenge: The tooth was highly inflamed (“hot tooth”), making standard anesthesia difficult due to the acidic tissue environment causing ion trapping.
Treatment Protocol: Dr. Nguyen Van Cuong initiated the procedure with a standard Inferior Alveolar Nerve Block (IANB) using 2% Lidocaine with 1:100,000 epinephrine. After 15 minutes, the patient exhibited profound lip numbness, but cold testing on the tooth still elicited a sharp pain response. Recognizing the anesthetic failure due to inflammation, Dr. Cuong administered a supplemental buccal infiltration using 4% Articaine, leveraging its superior bone penetration properties. This was followed by an intraligamentary (PDL) injection directly into the periodontal space.
Outcome: Within 3 minutes of the supplemental injections, the tooth achieved profound pulpal anesthesia. The root canal procedure was completed seamlessly, and the patient reported zero discomfort during the instrumentation phase. This case highlights the necessity of utilizing advanced pharmacological agents and varied injection techniques to overcome localized tissue acidosis.
When to See a Doctor: Managing Anesthesia Side Effects and Complications
Local dental anesthesia is overwhelmingly safe, and adverse reactions are exceedingly rare. However, because these are potent pharmacological agents, complications can occasionally arise. It is crucial for patients to recognize the difference between normal post-operative sensations and signs that require immediate medical or dental evaluation.
Important Clinical Considerations & Warning Signs
While minor bruising or soreness at the injection site is normal, you should contact your dentist or seek medical attention if you experience any of the following:
- Prolonged Paresthesia: If your lips, tongue, or jaw remain completely numb or tingly for more than 12 hours after the procedure, it may indicate nerve irritation or minor trauma from the needle. While most cases resolve spontaneously over a few weeks, clinical evaluation is necessary.
- Severe Swelling or Hematoma: A rapidly expanding swelling or large bruise on the cheek or jaw immediately after an injection suggests a hematoma (blood pooling outside a vessel).
- Signs of Allergic Reaction: True allergies to amide anesthetics are incredibly rare. However, allergies to the preservatives (like sodium metabisulfite) can occur. Seek emergency care if you develop hives, a rash, severe itching, or difficulty breathing.
- Systemic Toxicity (LAST): Local Anesthetic Systemic Toxicity is a rare but serious event where too much anesthetic enters the bloodstream. Symptoms include dizziness, metallic taste, visual disturbances, muscle twitching, or confusion.
“Patient safety during the administration of local anesthesia requires meticulous aspiration techniques to prevent intravascular injection and strict adherence to maximum dosage calculations based on the patient’s body weight and medical history.”[3]
— British Dental Journal, Management of Local Anesthetic Systemic Toxicity
For patients preparing for extensive treatments, maintaining routine dental visits and practicing proper brushing habits can prevent the severe infections that make numbing difficult. If you suffer from chronic bad breath or tooth pain, early intervention is key. When choosing a qualified dental provider, ensure they offer comprehensive pain management options, including advanced local anesthetics and sedation protocols.
Frequently Asked Questions
Do dentists still use Novocaine to numb teeth?
No, modern dentists rarely use Novocaine. Today, dental professionals rely on safer, faster-acting, and more effective amide anesthetics like Lidocaine and Articaine, which have a significantly lower risk of allergic reactions compared to the older ester-based Novocaine. The term “Novocaine” is now mostly used colloquially by patients to refer to any dental numbing shot.
Does the dental numbing injection hurt?
The injection itself causes minimal discomfort because dentists apply a topical numbing gel to the gums beforehand. Patients typically feel a slight pinch or a sensation of mild pressure as the anesthetic fluid enters the tissue, rather than sharp pain. Deep breathing and relaxation techniques can further minimize any perceived discomfort.
How long does it take for dental numbing to wear off?
Dental numbing typically lasts between one to three hours for the tooth, while the lips and tongue may remain numb for three to five hours. The exact duration depends on the type of anesthetic used, the presence of epinephrine, and your individual metabolism. It is important to avoid chewing hard foods until full sensation returns.
Can I request not to have a numbing shot for a filling?
Yes, you can decline a numbing shot, but it is generally not recommended for procedures that penetrate the dentin or approach the nerve. If you have severe needle phobia, discuss alternative comfort options like nitrous oxide or sedation with your dentist. For very shallow, surface-level cavities, numbing may occasionally be skipped at the dentist’s discretion.
Why does my heart race after getting a dental numbing shot?
A racing heart is a common, temporary reaction caused by epinephrine, a vasoconstrictor mixed into the anesthetic to prolong numbness and reduce bleeding. This sensation is harmless for most patients and typically subsides within a few minutes as the body processes the adrenaline. If you have a history of heart issues, inform your dentist so they can use an epinephrine-free alternative.
References
- Journal of the American Dental Association. Pharmacology and clinical efficacy of local anesthetics in dentistry. (2021).
- International Journal of Oral and Maxillofacial Surgery. Articaine versus Lidocaine for inferior alveolar nerve blocks. (2020).
- British Dental Journal. Management of local anesthetic systemic toxicity and adverse reactions. (2019).
- Journal of Endodontics. Overcoming anesthetic failure in teeth with irreversible pulpitis. (2022).
- Clinical Oral Investigations. The role of vasoconstrictors in modern dental local anesthesia. (2018).




