

The average cost of a routine teeth cleaning without insurance typically ranges from $75 to $200, depending on geographic location and clinical complexity. However, if periodontal disease is present, advanced scaling and root planing procedures will significantly increase the overall out-of-pocket expense.
Clinical Summary:
For patients navigating dental care without active coverage, understanding the financial and clinical scope of oral prophylaxis is essential. A standard preventive cleaning focuses on removing supragingival plaque and calculus to maintain gingival health and prevent structural decay. Conversely, when a patient presents with active periodontal disease, a more intensive, therapeutically driven scaling and root planing procedure is required to halt bone loss. Exploring alternative payment structures, in-house discount plans, or specialized community clinics can help mitigate these out-of-pocket costs while ensuring that critical preventive and therapeutic oral health standards are maintained.
Key Takeaways:
- Routine prophylaxis without insurance generally costs between $75 and $200 per visit.
- Periodontal deep cleaning (scaling and root planing) is a therapeutic procedure that carries a higher fee, often billed per quadrant.
- New patient appointments frequently incur additional diagnostic fees for comprehensive clinical exams and radiographic imaging.
- Preventive cleanings are biologically crucial for halting the progression of reversible gingivitis into irreversible periodontitis.
- Uninsured patients can utilize dental savings plans, flexible payment installments, or seek care at educational institutions to manage costs.
The Clinical Reality: Average Cost of Dental Services for Prophylaxis
The financial investment for a dental cleaning varies based on the required clinical intervention, with standard preventive prophylaxis costing significantly less than advanced periodontal therapy.
When evaluating the financial landscape of oral healthcare, patients without active coverage often experience anxiety regarding out-of-pocket expenses. The comprehensive dental care guide emphasizes that the cost of a cleaning is not a single, static figure. Instead, it is determined by the specific Current Dental Terminology (CDT) codes utilized during the visit, which reflect the clinical complexity of the procedure performed. The average cost of dental services fluctuates based on regional economic factors, the overhead costs of the specific dental practice, and the baseline oral health of the patient presenting for care.[1]
For a new patient, the initial visit is rarely just a cleaning. Comprehensive diagnostic data must be gathered to establish a baseline of oral health. This typically includes a comprehensive oral evaluation (CDT code D0150) and a full-mouth series of radiographs or a panoramic X-ray (D0210 or D0330). These diagnostic tools are non-negotiable from a clinical standpoint, as they allow the practitioner to detect interproximal decay, evaluate alveolar bone levels, and identify any asymptomatic pathology. Consequently, the first visit without insurance can range from $200 to $400 when combining the exam, X-rays, and the prophylaxis itself.

Once established as a patient of record, the ongoing costs become more predictable. A standard adult prophylaxis (D1110) is designed for patients with a healthy periodontium—meaning those without active bone loss or deep periodontal pockets. This preventive service is generally the most affordable tier of professional cleaning. However, if a patient has neglected their oral hygiene for an extended period, they may require a full mouth debridement (D4355) to remove gross calculus before a comprehensive exam can even be accurately performed. Understanding these distinctions is vital for patients trying to budget for their healthcare.
| Procedure Type | Clinical Indication | Estimated Out-of-Pocket Cost (Without Insurance) |
|---|---|---|
| Routine Prophylaxis (Adult) | Healthy gums, preventive maintenance, removal of supragingival plaque. | $75 – $200 |
| New Patient Exam & X-Rays | Initial diagnostic baseline, caries detection, bone level assessment. | $150 – $350 (in addition to cleaning) |
| Full Mouth Debridement | Severe calculus buildup obscuring the teeth, preventing accurate diagnosis. | $150 – $300 |
| Scaling and Root Planing (Per Quadrant) | Active periodontal disease, pocket depths >4mm, subgingival calculus. | $150 – $350 per quadrant |
| Periodontal Maintenance | Ongoing management following active periodontal therapy (SRP). | $115 – $250 per visit |
It is important to note that these figures represent national averages and can vary. Patients seeking more affordable options might look for a sliding scale dentist—practitioners or community health centers that adjust their fees based on the patient’s income and ability to pay. These facilities are crucial safety nets for uninsured populations, ensuring that financial barriers do not entirely preclude access to essential preventive care.[2]
Diagnostic Workflows: What Happens During a Professional Dental Cleaning?
A professional cleaning involves a systematic clinical workflow including ultrasonic scaling, hand instrumentation, coronal polishing, and targeted fluoride application to restore gingival health.
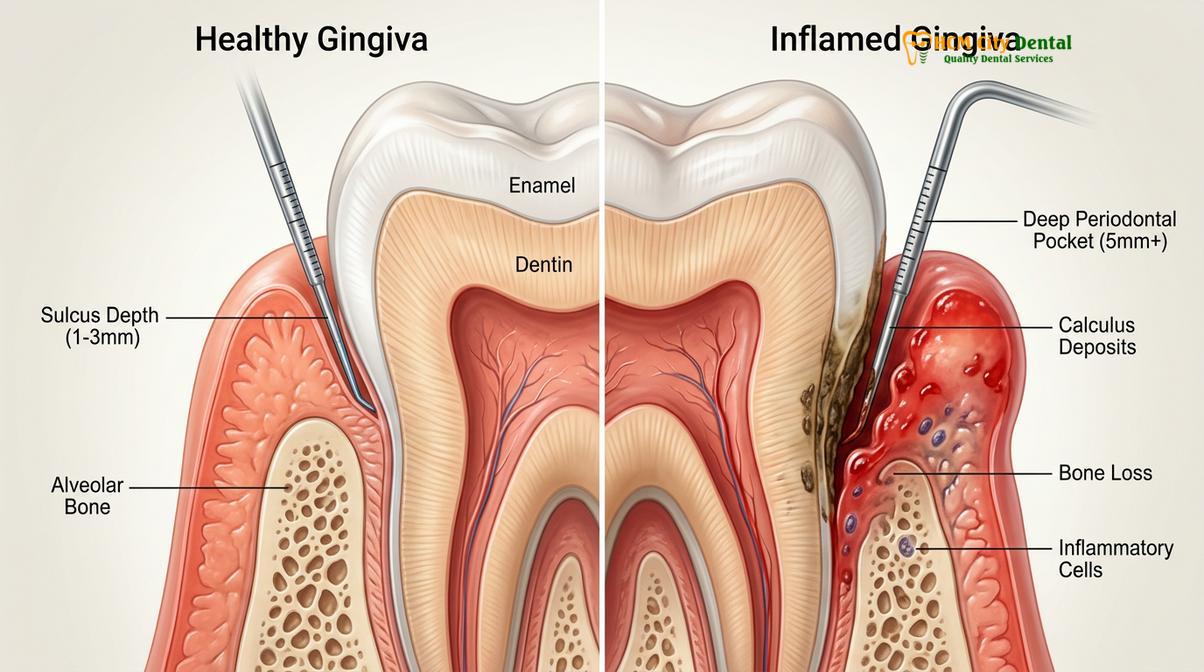
A professional dental prophylaxis is a meticulous clinical procedure that goes far beyond the capabilities of at-home brushing and flossing. The primary objective is the disruption and removal of the bacterial biofilm and calcified deposits (tartar) that adhere to the tooth surfaces. The workflow begins with a thorough periodontal assessment. The clinician uses a periodontal probe to measure the depth of the gingival sulcus—the space between the tooth and the surrounding gum tissue. In a healthy state, these measurements range from 1 to 3 millimeters. Measurements of 4 millimeters or greater indicate inflammation, attachment loss, and the potential presence of periodontal disease.
Following the assessment, the mechanical removal of deposits begins. Modern dental practices heavily utilize ultrasonic scalers. These sophisticated devices use high-frequency vibrations (ranging from 25,000 to 45,000 cycles per second) to shatter the crystalline structure of calculus. Simultaneously, a continuous stream of water cools the instrument tip and creates a phenomenon known as cavitation. The collapsing water bubbles produce shockwaves that disrupt the cell walls of pathogenic bacteria, effectively flushing the periodontal pocket and reducing the bacterial load.[3]
“The integration of ultrasonic instrumentation has revolutionized preventive care. Not only does it efficiently remove tenacious calculus, but the acoustic microstreaming actively destroys the biofilm matrix, promoting a faster and more robust healing response in the gingival tissues.”
— Dr. Nguyen Van Cuong, Clinical Director
After the bulk of the calculus is removed via ultrasonic technology, the clinician transitions to hand instrumentation. Using specialized tools such as Gracey curettes and universal scalers, the practitioner meticulously adapts the blade to the contours of each tooth. This step requires profound knowledge of dental anatomy to ensure that all residual deposits are removed from the interproximal spaces and the cementoenamel junction without damaging the underlying tooth structure. This professional dental prophylaxis is critical for creating a smooth surface that is less conducive to future plaque accumulation.
The final stages of the cleaning involve coronal polishing and, frequently, fluoride application. Polishing is performed using a slow-speed handpiece and a mildly abrasive prophylaxis paste. This step removes extrinsic stains caused by dietary factors like coffee, tea, and tobacco, while also smoothing the enamel surface. Finally, a topical fluoride varnish may be applied. Fluoride ions integrate into the hydroxyapatite structure of the enamel, converting it into fluorapatite, which is significantly more resistant to acid attacks from cariogenic bacteria. This biochemical reinforcement is a cornerstone of preventive dentistry.
Routine Prophylaxis vs. Periodontal Scaling and Root Planing (Deep Cleaning)
While routine prophylaxis focuses on the visible crown of the tooth, scaling and root planing addresses subgingival calculus and bacterial biofilms in deep periodontal pockets.
One of the most common sources of confusion—and unexpected expense—for uninsured patients is the distinction between a “regular cleaning” and a “deep cleaning.” From a clinical perspective, these are entirely different procedures with distinct therapeutic goals. A routine prophylaxis (D1110) is strictly preventive. It is indicated for patients who exhibit a healthy periodontium, characterized by pink, firm gingiva, no bleeding upon probing, and pocket depths of 3 millimeters or less. The focus is on the supragingival environment (above the gumline) to prevent the onset of gingivitis.
Conversely, Scaling and Root Planing (SRP), commonly referred to as a deep cleaning, is a non-surgical periodontal therapy. It is indicated when a patient has transitioned from reversible gingivitis to irreversible periodontitis. Periodontitis is characterized by the apical migration of the junctional epithelium and the destruction of the alveolar bone that supports the teeth. As the bone recedes, deep periodontal pockets form, creating an anaerobic environment where highly virulent, gram-negative bacteria thrive. These bacteria calcify into subgingival calculus, which acts as a porous reservoir for endotoxins, perpetuating a chronic inflammatory response.[4]
Clinical Case Study: Periodontal Intervention
Patient Profile: A 45-year-old male presented to HCMC Dental Clinic in Ho Chi Minh City complaining of chronic halitosis and gums that bled easily during brushing. He had not received professional dental care in over five years due to a lack of insurance.
Clinical Findings: Periodontal probing revealed generalized pocket depths of 5-6mm, significant subgingival calculus, and localized bleeding on probing (BOP). Radiographs confirmed early to moderate horizontal bone loss.
Treatment Protocol: Dr. Nguyen Van Cuong diagnosed the patient with Stage II Periodontitis. A comprehensive treatment plan was initiated, consisting of Scaling and Root Planing (SRP) across all four quadrants, performed under local anesthesia to ensure patient comfort. The procedure successfully removed the subgingival endotoxins and calculus.
Outcome: At the 6-week re-evaluation, tissue inflammation had dramatically subsided, and pocket depths had reduced to a manageable 3-4mm. The patient was placed on a 3-month periodontal maintenance schedule to sustain the clinical improvements.
During an SRP procedure, the clinician must instrument deep below the gumline. Local anesthesia is almost always required to ensure patient comfort, as the roots of the teeth are highly sensitive. The “scaling” portion removes the calculus, while the “root planing” portion involves smoothing the root surfaces (cementum and dentin) to remove necrotic tissue and bacterial toxins. This smooth surface facilitates the reattachment of the gingival tissues to the tooth, thereby reducing the pocket depth. Because of the time, skill, and anesthesia required, SRP is significantly more expensive than a routine cleaning and is usually billed per quadrant. Understanding the standard pricing for oral hygiene treatments helps patients anticipate these necessary therapeutic costs.
Navigating Financials: How to Manage Costs Without Coverage
Uninsured patients can access affordable care by leveraging dental savings plans, exploring flexible payment options, or seeking treatment at community health centers.
The financial barrier to dental care is a significant public health issue. When patients lack employer-sponsored benefits, they must proactively seek alternative methods to fund their oral healthcare. One of the first steps many take is to attempt to find dental insurance on the private market. However, it is crucial to critically evaluate the dental insurance cost against the actual benefits provided. Many private plans have waiting periods for major restorative work, high deductibles, and annual maximums that cap the insurer’s payout. Patients must calculate whether the monthly premiums justify the coverage, or if paying out-of-pocket for preventive care is more economically viable.
When asking how much is dental insurance, individuals often find that premiums can range from $20 to $50 per month for an individual. Over a year, this equates to $240 to $600. If a patient only requires two routine cleanings and an exam (which might cost $300 out-of-pocket), purchasing insurance solely for preventive care may not yield a positive return on investment. In these scenarios, alternative financial strategies become highly relevant.

Many modern dental practices recognize the challenges faced by uninsured patients and have implemented in-house membership plans or dental savings plans. For a flat annual fee, patients typically receive two cleanings, exams, and necessary X-rays, along with a percentage discount on restorative procedures like fillings or crowns. This model eliminates the middleman, removes waiting periods, and provides transparent pricing. Furthermore, for patients requiring extensive periodontal therapy, discussing flexible dental payment structures or third-party financing (such as CareCredit) can break a large treatment plan into manageable monthly installments.
Important Financial Consideration
Delaying routine preventive care due to immediate cost concerns is a false economy. The progression of untreated gingivitis into periodontitis, or a small enamel lesion into deep dentinal decay, will inevitably require complex, high-cost interventions such as root canal therapy, extractions, or dental implants. Investing in biannual prophylaxis is the most effective strategy for minimizing long-term dental expenditures.
For those facing severe financial hardship, seeking care at a dental hygiene school or a university dental clinic is a viable option. These institutions offer services at a fraction of the cost of private practice. While appointments may take longer because students are meticulously supervised by licensed clinical instructors, the standard of care remains exceptionally high. Additionally, researching local community health centers that operate on a sliding fee scale based on income can provide access to essential services for vulnerable populations, ensuring that managing oral health expenses without coverage is achievable.
The Hidden Costs of Neglecting Oral Hygiene
Foregoing routine cleanings allows pathogenic bacteria to proliferate, leading to systemic inflammation, tooth mobility, and the eventual need for complex restorative procedures.
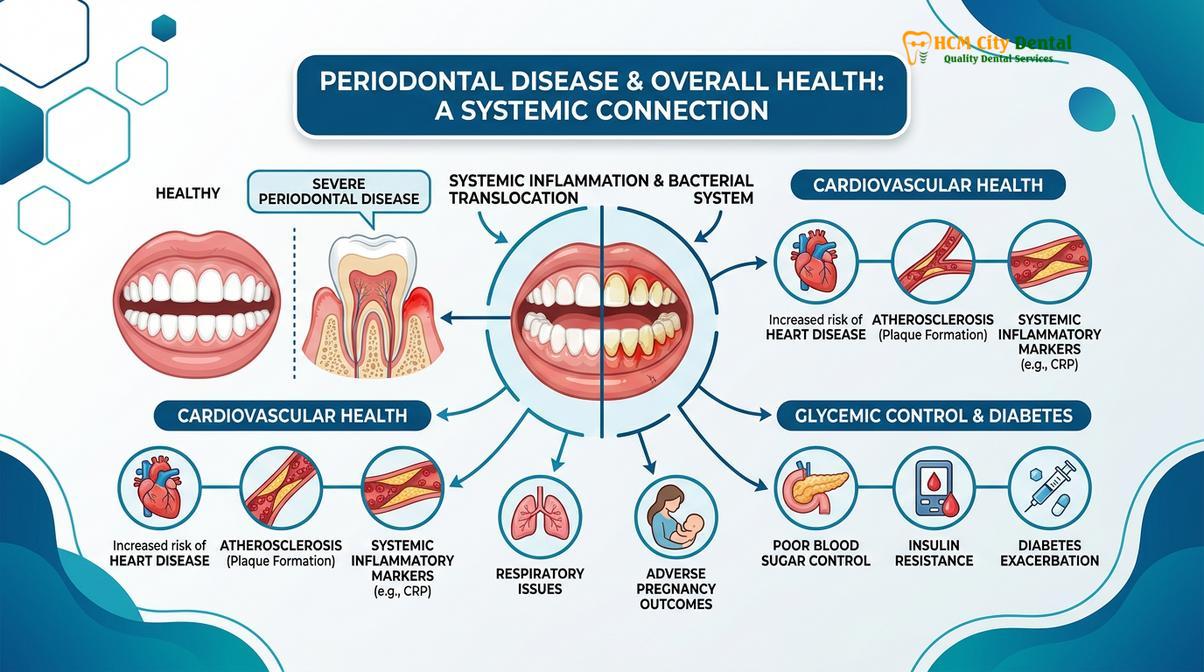
The decision to skip routine dental cleanings often stems from a misunderstanding of the profound impact oral health has on the entire body. The oral cavity is not an isolated system; it is the primary gateway to the gastrointestinal and respiratory tracts. When plaque is allowed to accumulate and calcify into calculus, it creates an impenetrable fortress for pathogenic bacteria. These bacteria, particularly gram-negative anaerobes like Porphyromonas gingivalis and Treponema denticola, trigger a chronic, hyper-inflammatory immune response in the host.[5]
This localized inflammation in the gingiva does not remain confined to the mouth. The ulcerated epithelial lining of deep periodontal pockets provides a direct portal of entry for these bacteria and their inflammatory cytokines (such as Interleukin-1 beta and Tumor Necrosis Factor-alpha) into the systemic bloodstream. This phenomenon, known as bacteremia, has far-reaching clinical implications. Extensive medical literature has established strong bidirectional links between severe periodontitis and systemic conditions, most notably cardiovascular disease and diabetes mellitus.
“We must view periodontal disease not merely as a threat to dentition, but as a systemic inflammatory burden. Managing oral biofilm through regular professional prophylaxis is a critical component of comprehensive medical wellness, particularly for patients with compromised glycemic control or cardiovascular risk factors.”
— Dr. Nguyen Van Cuong, Clinical Director
In diabetic patients, the presence of chronic periodontal inflammation exacerbates insulin resistance, making it significantly more difficult to maintain stable blood glucose levels (HbA1c). Conversely, poorly controlled diabetes impairs wound healing and increases susceptibility to periodontal destruction, creating a vicious cycle. Furthermore, the inflammatory mediators released during periodontal disease contribute to endothelial dysfunction and the progression of atherosclerosis, increasing the risk of myocardial infarction and stroke. Therefore, the cost of a dental cleaning is negligible when compared to the medical expenses associated with managing these severe systemic complications. Reviewing patient clinical outcomes and reviews often highlights the life-changing impact of establishing a consistent preventive care routine.
When to See a Doctor: Critical Signs of Periodontal Disease
While understanding the financial aspects of dental care is important, recognizing the clinical warning signs that necessitate immediate professional intervention is paramount. Patients should not wait for their scheduled biannual cleaning if they experience acute symptoms of periodontal distress. Early intervention is the key to preserving the natural dentition and minimizing the need for invasive surgical procedures.
You should schedule an immediate clinical evaluation if you observe any of the following symptoms:
- Spontaneous Gingival Bleeding: Gums that bleed easily during normal brushing, flossing, or even while eating soft foods indicate severe inflammation and ulceration of the sulcular epithelium.
- Purulent Exudate (Pus): The presence of pus expressing from the gumline when pressure is applied is a definitive sign of an active, localized bacterial infection (periodontal abscess) that requires immediate drainage and therapeutic scaling.
- Increased Tooth Mobility: Teeth that feel loose or shift in position indicate significant destruction of the underlying alveolar bone and periodontal ligament. This is a late-stage sign of periodontitis.
- Gingival Recession: Gums that are pulling away from the teeth, exposing the sensitive root surfaces, increase the risk of root caries and indicate a loss of clinical attachment.
- Persistent Halitosis: Chronic bad breath or a metallic taste in the mouth that does not improve with oral hygiene is often caused by the volatile sulfur compounds produced by anaerobic bacteria residing in deep periodontal pockets.

If you are experiencing any of these symptoms, it is critical to seek a comprehensive periodontal evaluation. At HCMC Dental Clinic in Saigon, our clinical team utilizes advanced diagnostic imaging and precise periodontal charting to develop targeted, evidence-based treatment plans. Do not let financial concerns delay necessary medical care; open communication with your provider can often lead to viable solutions that prioritize your health while respecting your budget.
Frequently Asked Questions
Clear, clinical answers to common patient inquiries regarding the costs, frequency, and necessity of professional dental cleanings without insurance.
Can I negotiate the price of a dental cleaning if I pay in cash?
Yes, many private dental practices offer a cash discount for uninsured patients who pay in full at the time of service. Inquiring about an in-house membership plan or a direct-pay discount can significantly reduce your overall out-of-pocket expenses. Dental offices save on administrative costs and credit card fees when patients pay in cash, and they are often willing to pass a portion of those savings on to the patient. Always ask the financial coordinator about available self-pay fee schedules prior to your appointment.
Is a deep cleaning always necessary if I haven’t been to the dentist in years?
Not always, but it is highly likely if periodontal pockets have formed. A clinical examination and periodontal probing are required to determine if subgingival calculus and bone loss are present, which dictate the need for scaling and root planing. If a patient has excellent home care and genetics, they may only require a standard prophylaxis or a full mouth debridement to remove supragingival buildup. The diagnosis is based entirely on objective clinical measurements, not merely the time elapsed since the last visit.
Are dental savings plans worth it for just routine cleanings?
Dental savings plans can be highly cost-effective even for routine care. By paying an annual fee, patients often receive two standard cleanings, comprehensive exams, and necessary radiographs at no additional charge, alongside discounts on restorative work. When calculating the individual out-of-pocket costs for these preventive services, the annual membership fee is frequently lower than the sum of the individual procedures, providing immediate financial value and encouraging consistent attendance.
How often should I get a cleaning if I am paying entirely out of pocket?
Clinical guidelines recommend a professional prophylaxis every six months for individuals with healthy gums. Patients with a history of periodontal disease may require periodontal maintenance visits every three to four months to prevent disease recurrence. While paying out of pocket can be challenging, adhering to these recommended intervals is the most effective way to prevent the development of severe pathology that would require vastly more expensive restorative or surgical interventions in the future.
Does a standard dental cleaning remove deep teeth stains?
A standard cleaning includes coronal polishing, which effectively removes extrinsic surface stains caused by coffee, tea, or tobacco. However, it will not alter the intrinsic color of the dentin, which requires professional chemical whitening treatments. The prophylaxis paste used during a cleaning is mildly abrasive and designed to smooth the enamel and remove biofilm and superficial discoloration, restoring the tooth to its natural baseline shade, but it cannot bleach the internal tooth structure.
References
- Journal of the American Dental Association. The economic impact of preventive dental care and prophylaxis. (2022).
- Journal of Periodontology. Clinical efficacy of scaling and root planing in the management of chronic periodontitis. (2021).
- International Dental Journal. Global variations in the average cost of dental services and out-of-pocket expenditures. (2020).
- Clinical Oral Investigations. The role of ultrasonic instrumentation in modern periodontal therapy. (2019).
- Journal of Dental Hygiene. Systemic health implications of untreated periodontal disease and biofilm accumulation. (2023).



