

Buck teeth, clinically known as overjet, can be effectively corrected using orthodontic braces. Treatment involves applying continuous, controlled pressure to retract protruding upper anterior teeth, improving facial aesthetics, restoring functional bite alignment, and preventing long-term dental complications.
Clinical Summary:
Overjet, commonly referred to as buck teeth, is a malocclusion characterized by the horizontal protrusion of the maxillary anterior teeth beyond the mandibular incisors. Orthodontic intervention using traditional braces, ceramic brackets, or clear aligners is the primary modality for correction. The clinical workflow involves comprehensive cephalometric diagnostics, biomechanical space closure (often utilizing extractions or temporary anchorage devices), and strict post-treatment retention. Addressing this condition not only enhances dentofacial aesthetics but also mitigates the risks of anterior dental trauma, abnormal enamel wear, and temporomandibular joint (TMJ) dysfunction. Treatment timelines generally range from 12 to 24 months, depending on the severity of the skeletal or dental discrepancy.
Key Takeaways:
- Overjet (buck teeth) is a horizontal protrusion, whereas an overbite is a vertical overlap of the anterior teeth.
- Treatment typically requires 12 to 24 months of continuous orthodontic force to safely retract the teeth.
- Severe cases may necessitate premolar extractions or Temporary Anchorage Devices (TADs) to create space for retraction.
- Untreated overjet significantly increases the risk of traumatic dental injuries and abnormal enamel wear.
- Post-treatment retention is mandatory to prevent the periodontal ligaments from pulling teeth back into a protrusive position.
Understanding Buck Teeth (Overjet) and Its Clinical Implications
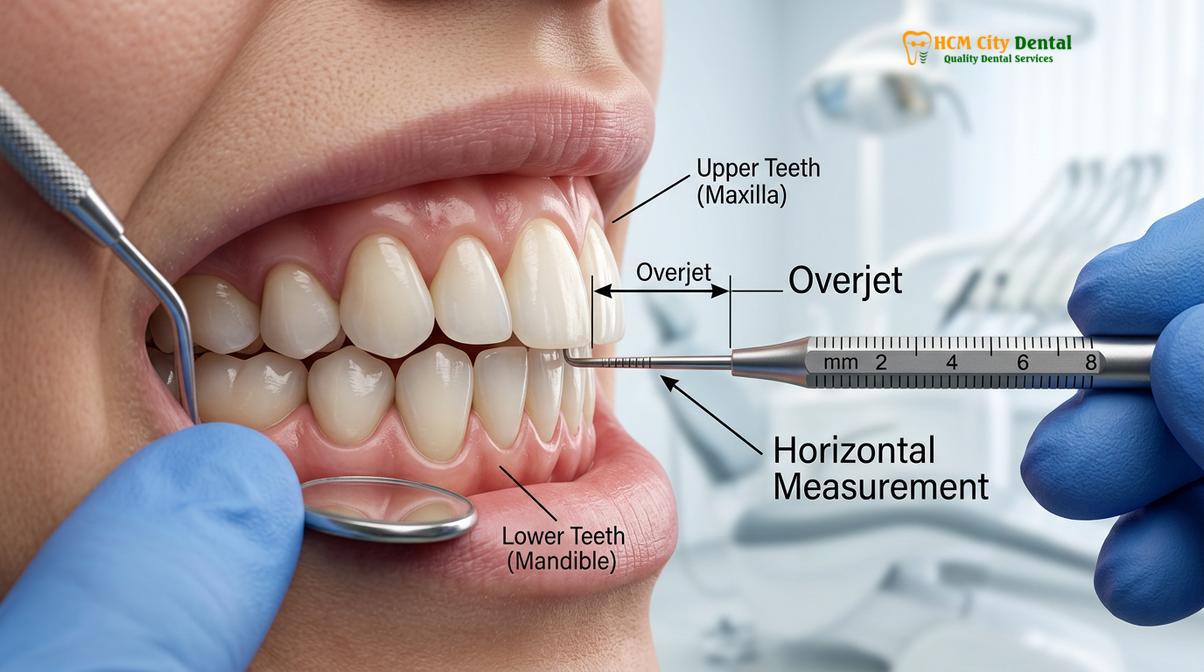
Overjet is a malocclusion where the upper front teeth horizontally protrude past the lower teeth. Correcting it prevents abnormal enamel wear, jaw joint dysfunction, and an increased risk of dental trauma.
In orthodontic terminology, the condition colloquially known as “buck teeth” is formally diagnosed as an overjet. While many patients seek treatment primarily for aesthetic reasons, the clinical implications of an untreated overjet extend far beyond facial appearance. A normal, healthy occlusion typically features a slight horizontal overlap of approximately 1 to 2 millimeters. When this measurement exceeds 3 millimeters, it is classified as an overjet, and in severe cases, the protrusion can extend beyond 8 to 10 millimeters [1].
It is crucial to differentiate between an overjet and an overbite, as patients frequently confuse the two terms. An overbite refers to the vertical overlap of the upper teeth over the lower teeth (a “deep bite”), whereas an overjet refers strictly to the horizontal distance. A patient can present with both an overbite and an overjet simultaneously, a condition often categorized under Class II Division 1 malocclusions [2].
The etiology of protruding anterior teeth is multifactorial, encompassing both genetic predispositions and environmental factors. Skeletal discrepancies, such as a prognathic (forward-positioned) maxilla or a retrognathic (underdeveloped) mandible, are often inherited traits. However, functional habits during early childhood play a significant role in exacerbating or directly causing dental overjet. Prolonged non-nutritive sucking habits, such as thumb or finger sucking beyond the age of four, exert continuous outward pressure on the developing maxillary alveolar bone and anterior teeth. Similarly, tongue thrusting—an atypical swallowing pattern where the tongue pushes against the lingual surfaces of the upper incisors—can gradually force the teeth outward over time.
From a clinical perspective, leaving an overjet untreated poses several functional risks. The protruding upper incisors are highly susceptible to trauma, particularly during sports or accidental falls, as they lack the protective coverage of the lower lip. Furthermore, the inability to achieve a proper lip seal (lip incompetence) often leads to chronic mouth breathing, which can dry out the oral cavity, reduce salivary flow, and increase the risk of caries and gingival inflammation. Patients with severe overjet may also experience difficulties with mastication and speech articulation, particularly with sibilant sounds.
Diagnostic Workflows for Protruding Anterior Teeth
A comprehensive orthodontic diagnosis utilizes cephalometric radiography and 3D intraoral scanning to evaluate skeletal discrepancies and dental angulations before formulating a precise treatment plan.
The foundation of successful overjet correction lies in a meticulous diagnostic phase. Orthodontic treatment is not merely about moving teeth; it is about managing the complex biomechanical relationship between the teeth, the alveolar bone, and the facial soft tissues. At specialized centers like HCMC Dental Clinic in Ho Chi Minh City, the diagnostic workflow begins with a comprehensive clinical examination and advanced radiographic imaging.
A lateral cephalometric radiograph is the gold standard for diagnosing the underlying cause of an overjet [3]. This specialized X-ray provides a profile view of the patient’s skull, allowing the orthodontist to measure specific angles and distances between skeletal landmarks. Key measurements, such as the SNA (Sella-Nasion-A Point) and SNB (Sella-Nasion-B Point) angles, help determine whether the protrusion is primarily dental (teeth tipping forward) or skeletal (the upper jaw is positioned too far forward relative to the cranial base). Understanding this distinction is critical, as skeletal overjets in adult patients may require orthognathic surgery in conjunction with braces, whereas dental overjets can typically be resolved with orthodontics alone.

In addition to 2D radiography, modern orthodontic diagnostics heavily rely on 3D intraoral scanning. Digital scanners capture highly accurate, high-resolution impressions of the patient’s dentition, eliminating the need for uncomfortable traditional alginate molds. These digital models are then imported into specialized orthodontic software, allowing the clinician to perform a virtual setup. Dr. Nguyen Van Cuong emphasizes that this digital workflow enables the precise calculation of the space required to retract the anterior teeth and allows the patient to visualize the projected outcome before treatment even begins.
The diagnostic phase also includes a thorough periodontal evaluation. Moving teeth through bone requires a healthy periodontium. If a patient presents with active gingivitis or periodontitis, these conditions must be stabilized before orthodontic forces are applied. Furthermore, the clinician will assess the patient’s airway and temporomandibular joint (TMJ) function, ensuring that the planned retraction of the anterior teeth will not negatively impact the patient’s breathing or jaw comfort.
Treatment Modalities: Braces for Buck Teeth
Orthodontic correction of overjet typically utilizes traditional metal braces, aesthetic ceramic brackets, or clear aligner therapy, depending on the severity of the protrusion and patient compliance.
Once a definitive diagnosis is established, the clinician will recommend the most appropriate orthodontic appliance to correct the overjet. The choice of modality depends on the severity of the malocclusion, the patient’s aesthetic preferences, and the specific biomechanical movements required to achieve an optimal result.
Traditional metal braces remain one of the most robust and predictable methods for correcting severe overjet. Composed of high-grade stainless steel brackets and archwires, metal braces offer unparalleled control over three-dimensional tooth movement. They are particularly effective in extraction cases where significant bodily movement of the teeth (moving the crown and the root simultaneously) is required to close spaces and retract the anterior segment [4].
For patients seeking a more discreet option, ceramic braces function similarly to metal braces but utilize clear or tooth-colored brackets that blend seamlessly with the natural enamel. While aesthetically superior, ceramic brackets can be slightly more fragile and may generate more friction against the archwire during the sliding mechanics of space closure. However, advancements in polycrystalline alumina have significantly improved the durability and performance of modern ceramic systems.

During the active phase of treatment, orthodontists frequently utilize rubber chain braces (elastomeric power chains) to consolidate spaces and apply continuous retracting force to the protruding teeth. These interconnected elastic rings are stretched across multiple brackets, slowly pulling the anterior teeth backward into their correct positions. The force applied must be carefully calibrated; excessive force can lead to root resorption or loss of anchorage, while insufficient force will stall tooth movement.
Clear aligner therapy (such as Invisalign) has also become a popular modality for correcting mild to moderate overjet. Aligners use a series of custom-fabricated, removable thermoplastic trays to incrementally push the teeth into alignment. While highly aesthetic and comfortable, clear aligners rely on pushing forces rather than the pulling forces of fixed braces. Consequently, severe skeletal overjets or cases requiring complex root torquing may still be better suited for traditional fixed appliances.
| Treatment Modality | Aesthetic Profile | Suitability for Severe Overjet | Biomechanical Control |
|---|---|---|---|
| Traditional Metal Braces | Highly visible | Excellent (Ideal for extraction cases) | Maximum 3D root control |
| Ceramic Braces | Discreet (tooth-colored) | Very Good | High control, slightly higher friction |
| Clear Aligners | Nearly invisible | Limited (Best for mild/moderate cases) | Moderate (Relies on attachments) |
| Lingual Braces | Completely hidden | Good | High control, complex adjustments |
Advanced Orthodontic Mechanics and Adjunctive Procedures
Severe overjet cases may require tooth extractions, temporary anchorage devices (TADs), or orthognathic surgery to achieve optimal retraction and a stable, functional occlusion.
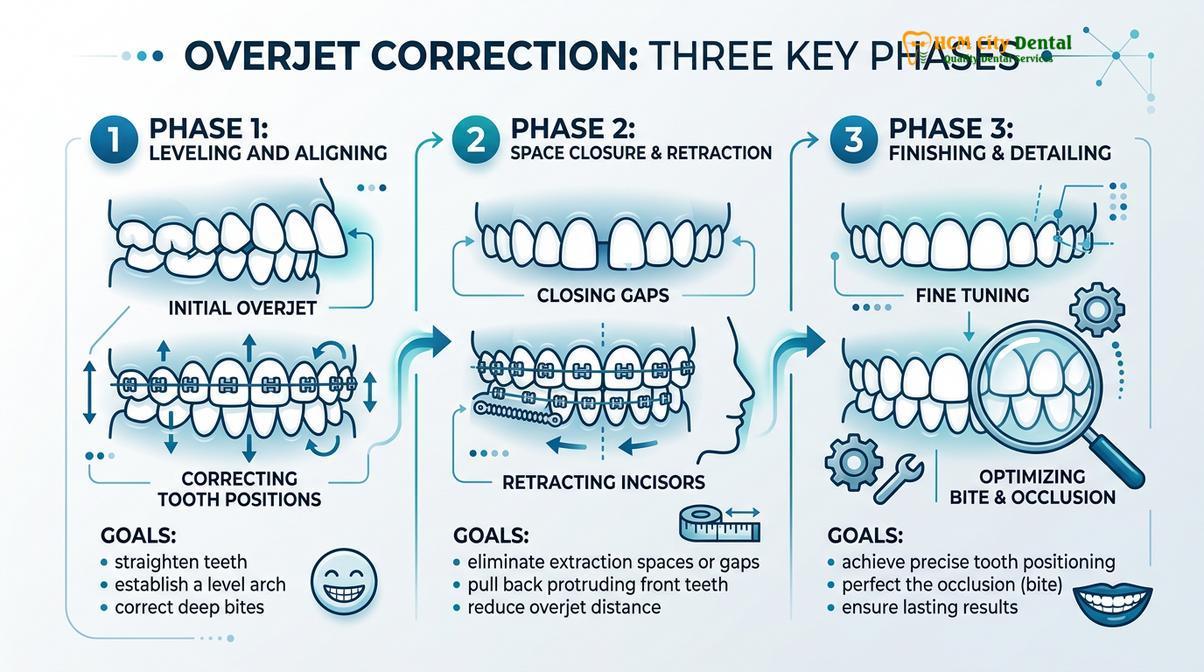
Correcting a significant overjet is rarely as simple as just pushing the front teeth backward. According to the principles of physics, every action has an equal and opposite reaction. When an orthodontist applies force to pull the front teeth back, an equal force is exerted on the back teeth (molars), pulling them forward. If the back teeth move forward too much, the space needed to retract the front teeth is lost. This concept is known as “anchorage control,” and managing it is the most challenging aspect of overjet correction.
In cases of severe dental protrusion, there is often insufficient space in the dental arch to simply align and retract the teeth. In such scenarios, the extraction of the maxillary first premolars is a standard clinical protocol. Removing these teeth creates approximately 7 to 8 millimeters of space on each side of the arch. The orthodontist then utilizes the posterior molars as an anchor to pull the six anterior teeth (canines and incisors) backward into the extraction spaces.
“The successful management of Class II malocclusions with severe overjet relies heavily on absolute anchorage. Without proper biomechanical control, the posterior dentition will drift mesially, compromising the retraction of the anterior segment and leading to suboptimal facial aesthetics.”
To prevent the back teeth from moving forward during this process, modern orthodontics frequently employs Temporary Anchorage Devices (TADs) [5]. TADs are biocompatible titanium mini-screws that are temporarily implanted into the alveolar bone. Because they are anchored directly into the bone, they do not move. The orthodontist can attach springs or elastomeric chains from the TADs directly to the anterior teeth, allowing for maximum retraction without any unwanted forward movement of the molars.
Occasionally, overjet is complicated by the presence of impacted or ectopic teeth. If an ectopic cuspid is present, collaboration with an oral surgeon or a specialized canine dentist is critical to surgically expose the tooth and bond an attachment to it. The orthodontist can then apply targeted traction to guide the impacted canine into the dental arch while simultaneously managing the overjet.
Clinical Case Review: Severe Overjet Management
A 24-year-old patient presented at HCMC Dental Clinic in Ho Chi Minh City with an 8mm overjet, lip incompetence, and a history of childhood thumb sucking. Cephalometric analysis revealed a severe Class II dental protrusion with a stable skeletal base. Dr. Nguyen Van Cuong formulated a treatment plan involving the extraction of the upper first premolars. Traditional metal braces were placed, and TADs were utilized in the maxillary arch to provide absolute anchorage. Over a period of 22 months, the anterior segment was successfully retracted, closing the extraction spaces entirely. The patient achieved a Class I canine relationship, a normal 2mm overjet, and a significantly improved facial profile with relaxed lip closure.
As the treatment nears completion, the focus shifts to the finishing and detailing phase. The orthodontist makes micro-adjustments to the archwires to ensure that the roots are perfectly parallel and the marginal ridges of the teeth align correctly. Once the overjet is fully reduced and the braces are removed, teeth reshaping after braces (enameloplasty or cosmetic contouring) is frequently performed. Because protruding teeth often wear unevenly prior to treatment, aligning them can reveal jagged or asymmetrical incisal edges. Gentle reshaping of the enamel ensures a harmonious, aesthetically pleasing smile line.
Timeline, Retention, and Post-Treatment Care
Correcting buck teeth generally takes between 12 to 24 months, followed by a strict retention phase to prevent the anterior teeth from relapsing to their original protrusive positions.
Patients frequently inquire about the duration of orthodontic treatment for overjet. The timeline is highly variable and depends on the biological response of the patient’s periodontal tissues, the severity of the initial malocclusion, and the specific mechanics employed. Mild dental overjets that do not require extractions can often be resolved in 12 to 15 months. However, severe cases involving premolar extractions, maximum anchorage retraction, or surgical interventions typically require 18 to 24 months of active treatment.
Bone remodeling is a biological process that cannot be rushed. Osteoclasts must break down bone on the pressure side of the moving tooth, while osteoblasts build new bone on the tension side. Applying excessive force in an attempt to speed up treatment can lead to hyalinization (tissue death) in the periodontal ligament, which actually halts tooth movement and increases the risk of root resorption.
The day the braces are removed is a milestone, but it does not mark the end of orthodontic care. The retention phase is arguably the most critical component of overjet correction. The gingival and periodontal fibers—specifically the supracrestal and transseptal fibers—have a “memory” and will actively try to pull the teeth back into their original protrusive positions. This phenomenon is known as orthodontic relapse [6].
“Retention is a lifelong commitment. The biological forces that cause teeth to shift do not cease once braces are removed. Without strict adherence to a retention protocol, the hard-earned correction of an overjet can rapidly deteriorate, necessitating retreatment.”
To combat relapse, patients are fitted with retainers immediately after the removal of their braces. There are several types of retainers utilized in clinical practice:
- Essix Retainers: Clear, removable thermoplastic trays that fit snugly over the entire arch, holding the teeth in their exact final positions.
- Hawley Retainers: Traditional removable retainers consisting of an acrylic palate and a metal wire that wraps around the anterior teeth. These are highly durable and allow for minor occlusal settling.
- Fixed Lingual Retainers: A custom-adapted braided wire bonded to the lingual (tongue) surfaces of the anterior teeth. This provides permanent, passive retention and is highly recommended for patients with a history of severe overjet or spacing.
Patients are typically instructed to wear their removable retainers full-time for the first three to six months post-treatment, transitioning to nighttime wear indefinitely. Regular follow-up appointments are essential to monitor the stability of the occlusion and ensure the retainers fit correctly.
When to See a Doctor for Overjet Correction
While minor overjets may be purely cosmetic, moderate to severe protrusions require professional clinical evaluation. It is highly recommended that children receive their first orthodontic screening by the age of seven. Early interceptive orthodontics (Phase I treatment) can utilize growth modification appliances to guide jaw development, potentially preventing a severe overjet from forming and reducing the need for extractions or surgery later in life.
For adolescents and adults, you should schedule a consultation with an orthodontic specialist if you experience any of the following functional symptoms associated with buck teeth:
- Difficulty closing the lips: If you must strain your chin muscles to close your lips over your teeth, or if you sleep with your mouth open, the overjet is likely affecting your airway and facial musculature.
- Speech impediments: Difficulty pronouncing certain consonants, particularly “S,” “F,” and “V” sounds, can be a direct result of anterior tooth protrusion.
- Trauma to the soft tissues: If your lower front teeth bite into the roof of your mouth (palatal impingement), or if your upper teeth frequently bite your lower lip, immediate intervention is required to prevent tissue damage and bone loss.
- Jaw pain or TMJ discomfort: A severe overjet often forces the lower jaw into an unnatural backward position during closure, leading to chronic muscle tension, clicking joints, and headaches.
Clinical Warning:
Never attempt to correct protruding teeth using DIY aligners, rubber bands, or at-home methods. Applying uncontrolled forces to the teeth can cause irreversible damage to the periodontal ligament, leading to severe root resorption, bone loss, and ultimately, tooth loss. Always seek a comprehensive general dental guide and consult a licensed professional for safe orthodontic care.
Dr. Cuong advises that a personalized clinical examination is the only way to determine the exact nature of the malocclusion. Through advanced diagnostics, a tailored treatment plan can be developed to safely and effectively retract the teeth, ensuring a stable, functional, and aesthetically pleasing outcome. Maintaining routine dental visits during and after orthodontic treatment is vital to monitor oral health and the integrity of the retention appliances.
Furthermore, patients undergoing orthodontic treatment must maintain impeccable oral hygiene. The presence of brackets and wires creates numerous plaque retentive areas. Utilizing specialized orthodontic toothbrushes, interdental brushes, and water flossers is essential to prevent decalcification (white spot lesions) and gingivitis. Understanding fluoride safety and enamel remineralization can also help protect the teeth during the active phase of braces. For patients engaged in contact sports, wearing custom mouthguards over the braces is mandatory to protect the protruding teeth and the soft tissues of the lips and cheeks from severe lacerations.
If you are considering orthodontic treatment, it is important to understand the risks of removing braces at home or abandoning treatment prematurely. Orthodontic care is a precise medical procedure that requires professional oversight from start to finish. Dentists seeking to expand their knowledge in this field often pursue orthodontic courses for general dentists to better understand the biomechanics of overjet correction and interdisciplinary case management.

Frequently Asked Questions
How long does it take to fix buck teeth with braces?
Correcting buck teeth typically takes between 12 to 24 months, depending on the severity of the overjet. Mild cases may resolve in 15 months, while severe skeletal protrusions requiring extractions or maximum anchorage can take up to two years or longer to ensure safe, stable tooth movement.
Can clear aligners fix severe buck teeth?
Clear aligners can effectively treat mild to moderate buck teeth, but severe skeletal overjet often requires traditional braces. Complex cases may necessitate auxiliary mechanics like premolar extractions, heavy rubber bands, or temporary anchorage devices (TADs) that are generally better suited for the robust control of fixed brackets.
Will fixing my buck teeth change my face shape?
Yes, correcting significant buck teeth can subtly improve your facial profile. By retracting protruding upper teeth, the upper lip can relax into a more natural, less strained position. This enhances facial symmetry, improves lip competence (the ability to close the lips naturally), and creates a more balanced side profile.
Do I need teeth extracted to fix an overjet?
Tooth extraction is not always necessary, but it is common in severe overjet cases. Removing the first premolars creates the required space in the dental arch to retract the protruding anterior teeth safely. Without extractions in severe cases, pushing the front teeth back would improperly force the back teeth out of alignment.
Why do my teeth still look uneven after my overjet is fixed?
Uneven wear patterns often develop before treatment due to the malocclusion and improper bite forces. Once the teeth are properly aligned, these pre-existing discrepancies become visible. This is why teeth reshaping after braces (enamel contouring) is frequently recommended by orthodontists to smooth jagged edges and achieve a perfectly symmetrical smile.
References
- American Journal of Orthodontics and Dentofacial Orthopedics. Biomechanics of anterior tooth retraction and anchorage control. (2021).
- Journal of Clinical Orthodontics. Etiology and management of Class II Division 1 malocclusions. (2020).
- International Journal of Dentistry. Cephalometric evaluation of overjet and overbite in orthodontic diagnostics. (2019).
- European Journal of Orthodontics. Comparative efficacy of self-ligating brackets versus conventional systems in space closure. (2022).
- Angle Orthodontist. The role of temporary anchorage devices (TADs) in maximum anterior retraction. (2018).
- Journal of Oral Rehabilitation. Long-term stability and retention protocols following severe overjet correction. (2023).



