A full dental bridge is a fixed prosthetic device designed to replace one or more missing teeth by anchoring artificial teeth to adjacent natural teeth or implants. This restoration helps restore chewing function, prevents structural shifting of the remaining dentition, and provides a seamless aesthetic appearance for patients experiencing partial edentulism.
Clinical Summary:
A full dental bridge serves as a highly effective, fixed prosthodontic solution for missing teeth, utilizing adjacent healthy teeth or implants as structural pillars. Modern all-porcelain and zirconia variations offer superior biocompatibility and aesthetic integration compared to traditional metal-fused options. Clinical success depends heavily on precise abutment preparation, accurate impression techniques, and optimal occlusal alignment to ensure long-term durability and periodontal health.
Key Takeaways:
- Restores masticatory function and prevents adjacent teeth from drifting into empty spaces.
- Requires irreversible preparation (enamel reduction) of the neighboring abutment teeth.
- All-porcelain materials provide exceptional translucency and biocompatibility for both anterior and posterior restorations.
- Treatment typically spans two to three clinical visits, from initial preparation to final cementation.
- Proper oral hygiene and routine professional maintenance are critical to prevent secondary caries under the bridge.
Clinical Definition and Biomechanics of a Full Dental Bridge
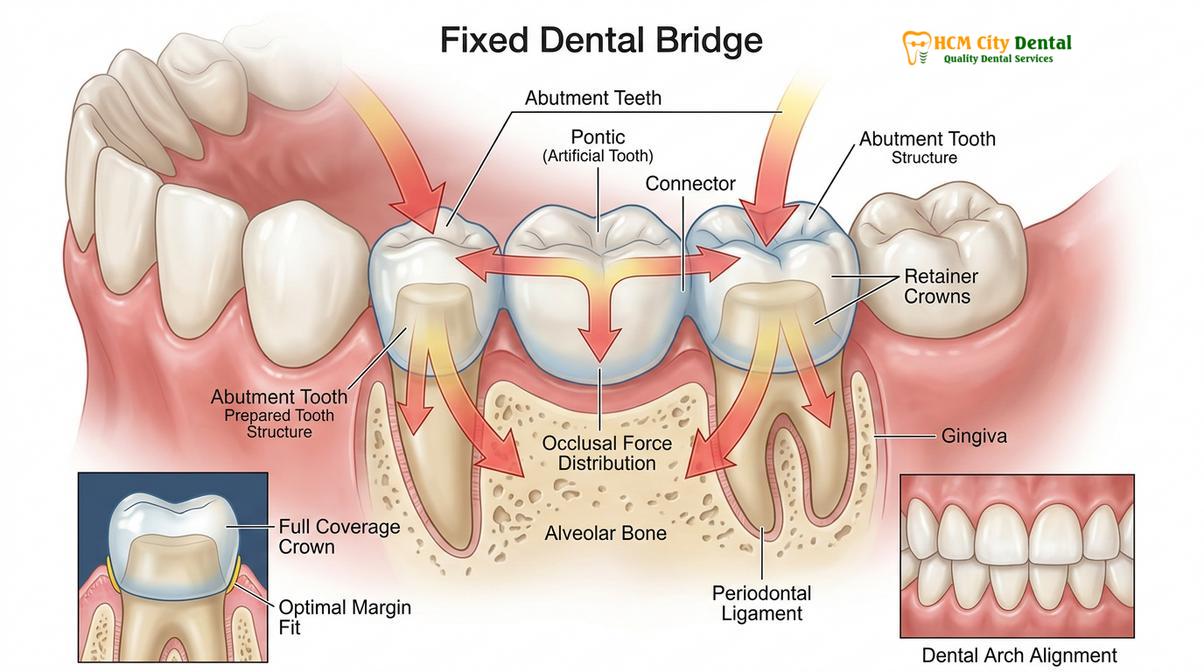
A full dental bridge relies on the structural integrity of adjacent abutment teeth to support an artificial pontic, effectively distributing occlusal forces across the dental arch to maintain stability.
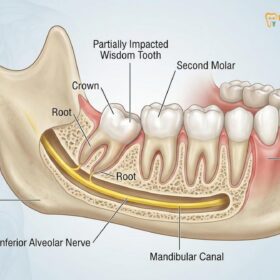
In the realm of fixed prosthodontics, a full dental bridge represents a cornerstone treatment for partial edentulism. When a tooth is lost, the surrounding dentition inevitably responds to the void. Adjacent teeth may tilt or drift into the space, while opposing teeth can super-erupt, leading to severe occlusal disharmony. A fixed bridge mitigates these complications by physically filling the gap and splinting the adjacent teeth together, thereby restoring optimal dental harmony across the arch.
The architecture of a standard dental bridge consists of two primary components: the abutments and the pontic. The abutments are the natural teeth (or dental implants) located on either side of the edentulous space. These teeth are meticulously reshaped to receive dental crowns, which serve as the anchors for the prosthesis. The pontic is the artificial tooth suspended between the abutment crowns, designed to replicate the exact morphology and function of the missing natural tooth. By fusing these elements into a single, continuous unit, the bridge effectively transfers the mechanical stress of mastication from the pontic to the robust root systems of the abutment teeth[1].
Understanding the biomechanics of a full dental bridge requires an appreciation of Ante’s Law, a fundamental principle in prosthodontics. Ante’s Law dictates that the combined pericemental area (root surface area) of the abutment teeth must be equal to or greater than that of the tooth or teeth being replaced. If a bridge is designed to replace multiple missing teeth using inadequate abutments, the excessive occlusal load can lead to periodontal ligament trauma, bone resorption, and eventual failure of the entire restoration.
“The long-term success of a fixed dental bridge is not merely about filling a gap; it is about engineering a restoration that respects the biological limits of the supporting teeth while seamlessly integrating into the patient’s dynamic occlusal scheme.”
— Dr. Nguyen Van Cuong, Prosthodontic Specialist
Furthermore, the design of the pontic plays a crucial role in maintaining periodontal health. The tissue-facing surface of the pontic must be highly polished and convex to allow for adequate plaque control. Modified ridge lap or ovate pontic designs are frequently utilized to create the illusion that the artificial tooth is emerging naturally from the gums, ensuring a fluid transition that mimics a natural contour along the gingival margin. This careful attention to soft tissue architecture helps prevent food impaction and subsequent gingival inflammation.
Indications and Contraindications for Bridge Placement
Candidacy for a fixed bridge requires healthy adjacent teeth with robust periodontal support, while severe bone loss or extensive edentulism may necessitate alternative prosthodontic treatments.
Determining the appropriate treatment modality for a missing tooth requires a thorough diagnostic workup, including clinical examination, periodontal probing, and radiographic analysis. While a full dental bridge is a highly versatile and predictable restoration, it is not universally applicable to all clinical scenarios. The decision to proceed with a fixed bridge hinges on a delicate balance between structural requirements and biological constraints.
The primary indication for a full dental bridge is the loss of one or two consecutive teeth in an arch where the adjacent teeth are structurally sound and periodontally stable. Ideal abutment teeth possess vital pulps, adequate coronal tooth structure for retention, and healthy surrounding gingival tissues. In cases where the adjacent teeth already exhibit structural damage or large existing restorations, a bridge can serve a dual purpose: replacing the missing tooth while simultaneously providing full-coverage protection to the compromised abutments.

Conversely, several clinical factors serve as absolute or relative contraindications for a traditional fixed bridge. Severe periodontal disease resulting in significant alveolar bone loss compromises the foundational support required to bear the additional occlusal load of a pontic. Mobile abutment teeth are generally unsuitable for bridge support, as the splinting effect of the bridge cannot overcome progressive attachment loss. Additionally, young patients with large pulp chambers are at a higher risk of iatrogenic pulpal exposure during the aggressive tooth preparation required for bridge abutments[2].
| Clinical Parameter | Favorable for Dental Bridge | Contraindicated for Dental Bridge |
|---|---|---|
| Abutment Health | Adequate bone support, minimal mobility | Severe periodontitis, Class II/III mobility |
| Span Length | 1-2 missing consecutive teeth | 3+ missing teeth (high risk of flexure) |
| Adjacent Teeth Status | Heavily restored or requiring crowns | Virgin, perfectly healthy teeth (implants preferred) |
| Occlusal Forces | Stable occlusion, normal mastication | Severe untreated bruxism or clenching |
Another critical consideration is the location of the edentulous space. Distal extension cases—where there is no posterior abutment tooth available (e.g., missing second and third molars)—cannot be treated with a traditional bridge. These scenarios typically require a removable partial denture or implant-supported restorations.
Material Selection: Why Porcelain Dominates Modern Prosthodontics
All-porcelain and zirconia bridges offer unmatched aesthetic translucency and tissue compatibility, largely replacing older metal-based restorations in modern clinical practice due to their superior biocompatibility.
The evolution of dental materials has profoundly transformed the fabrication of fixed prostheses. Historically, Porcelain-Fused-to-Metal (PFM) bridges were the gold standard, offering the mechanical strength of a cast metal substructure combined with the tooth-colored aesthetics of an overlying feldspathic porcelain layer. However, PFM restorations present inherent aesthetic limitations. The opaque metal substructure prevents natural light transmission, often resulting in a dull, lifeless appearance. Furthermore, as gingival recession occurs over time, the dark metal margin frequently becomes visible at the gum line, compromising the smile’s aesthetics.
Today, advancements in ceramic engineering have propelled all-porcelain and monolithic zirconia materials to the forefront of restorative dentistry. These materials allow clinicians to achieve exceptional aesthetics without sacrificing mechanical durability. Monolithic zirconia, specifically Yttria-stabilized tetragonal zirconia polycrystal (Y-TZP), exhibits extraordinary flexural strength, making it highly resistant to fracture even under heavy posterior occlusal loads. Unlike PFM bridges, zirconia is entirely metal-free, eliminating the risk of dark margins and providing excellent biocompatibility to support optimal periodontal tissue health[3].

For anterior restorations where aesthetic demands are paramount, lithium disilicate (commonly known as E.max) is frequently the material of choice. While slightly less robust than zirconia, lithium disilicate offers unparalleled translucency, opalescence, and fluorescence, closely mimicking the optical properties of natural enamel. In many cases, a hybrid approach is utilized: a strong zirconia framework is layered with translucent feldspathic porcelain to combine maximum strength with superior cosmetic outcomes, similar to the principles used in advanced cosmetic porcelain enhancements.
Clinical Warning: While all-ceramic materials are highly durable, they are not indestructible. Patients with severe, unmanaged bruxism (teeth grinding) may exert forces that exceed the fracture toughness of porcelain. In such cases, the fabrication of a custom occlusal night guard is strongly recommended to protect the investment and prevent catastrophic failure of the bridge.
The selection of the appropriate material is a highly individualized process. The clinician must evaluate the location of the bridge, the patient’s occlusal dynamics, the shade of the adjacent dentition, and the available interocclusal clearance.
The Clinical Workflow: From Preparation to Final Cementation
The bridge fabrication process involves precise enamel reduction, digital or physical impressions, temporary provisionalization, and the final bonding of the custom prosthetic using specialized dental cements.
The fabrication and placement of a full dental bridge is a highly technique-sensitive procedure that typically requires two to three clinical appointments. The workflow demands precision at every stage, from the initial biomechanical preparation of the abutment teeth to the final adhesive protocols used during cementation. Any deviation from established prosthodontic principles can compromise the marginal integrity, retention, and longevity of the restoration.
The first clinical phase involves the preparation of the abutment teeth. Following the administration of profound local anesthesia to ensure patient comfort, the clinician systematically reduces the enamel and dentin of the abutment teeth. This reduction creates the necessary three-dimensional space for the restorative material. The preparation must feature a specific geometric design, including a precise total occlusal convergence (taper) to provide adequate retention and resistance form. The margins are carefully placed to ensure a smooth, imperceptible transition that respects the biological width of the gingival tissues.
Clinical Case Overview: A 45-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City with a missing mandibular first molar, complaining of difficulty chewing and food impaction. The clinical team evaluated the adjacent second premolar and second molar, noting they were heavily restored but periodontally sound. A monolithic zirconia bridge was prescribed. Following precise margin preparation and digital intraoral scanning, a custom bridge was milled and cemented. The patient reported immediate restoration of masticatory function and excellent soft tissue adaptation at the follow-up appointment.
Once the teeth are optimally prepared, accurate replication of the dental arch is required. Modern practices increasingly utilize digital intraoral scanners to capture highly detailed 3D optical impressions, eliminating the discomfort associated with traditional gooey impression materials. If traditional methods are used, a dual-cord tissue retraction technique is often employed to temporarily displace the gingiva, ensuring the impression material captures the exact location of the preparation margins.
While the definitive bridge is being fabricated in the dental laboratory, a custom provisional (temporary) bridge is fabricated using bis-acryl composite resin. This provisional restoration is cemented with temporary cement and serves several critical functions: it protects the exposed dentin to assist in managing acute dental discomfort, maintains the position of the prepared teeth to prevent shifting, and allows the patient to evaluate the proposed aesthetics and function.
During the final insertion appointment, the provisional bridge is carefully removed, and the abutment teeth are thoroughly cleaned. The definitive porcelain bridge is then tried in to verify marginal fit, proximal contacts, and occlusal harmony. Once the fit is confirmed clinically and radiographically, the bridge is permanently bonded. The cementation protocol varies based on the material; zirconia may be cemented using resin-modified glass ionomer or adhesive resin cements, while lithium disilicate requires strict isolation, hydrofluoric acid etching, silanization, and dual-cure resin bonding for optimal adhesion[4].
Comparing Full Dental Bridges to Implant-Supported Alternatives
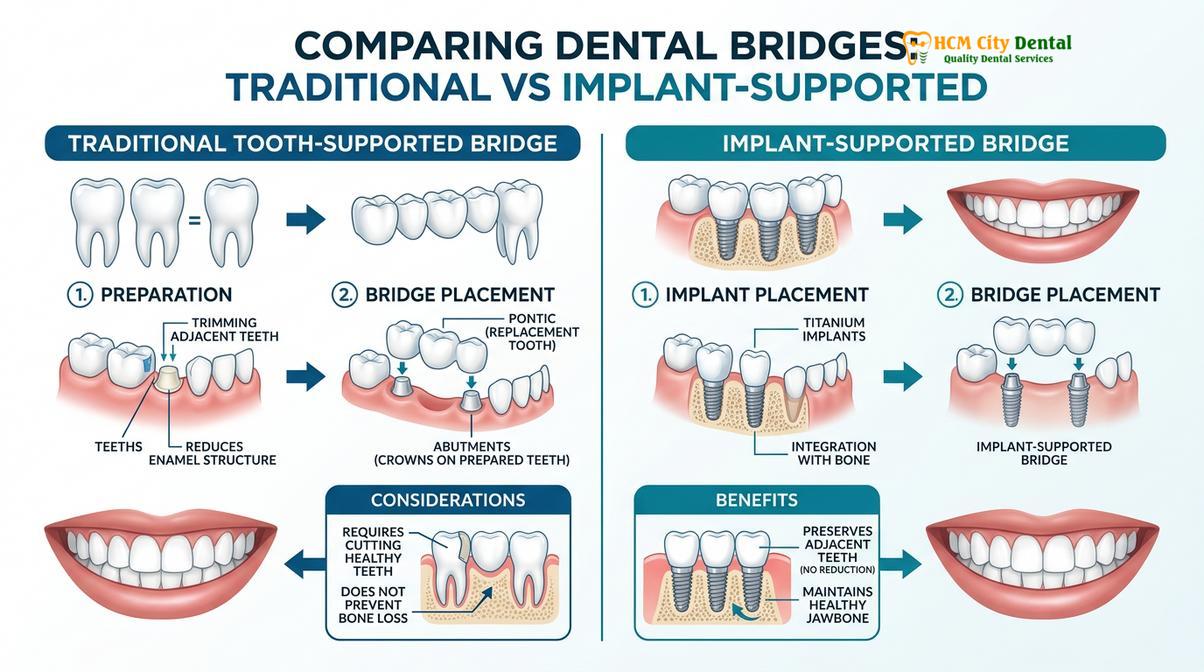
While traditional bridges utilize natural teeth for support, implant-supported bridges rely on titanium posts integrated into the jawbone, preserving adjacent healthy enamel and preventing bone resorption.
When evaluating options for replacing missing teeth, patients frequently weigh the benefits of a traditional full dental bridge against implant-supported restorations. Both modalities offer distinct advantages and are selected based on the patient’s unique anatomical, financial, and temporal considerations. Understanding the fundamental differences between these approaches is essential for informed clinical decision-making.
The primary advantage of a traditional fixed bridge is the speed and predictability of the treatment. A bridge can typically be completed within a few weeks, immediately restoring function and aesthetics without the need for surgical intervention. This makes it an excellent option for patients who have medical contraindications to surgery, lack adequate bone volume for implants, or desire a faster resolution. Furthermore, if the adjacent teeth already require full-coverage crowns due to extensive decay or large fillings, a bridge efficiently addresses multiple restorative needs simultaneously.
“The paradigm of tooth replacement has shifted towards conservative dentistry. Whenever possible, we aim to preserve virgin tooth structure. However, when adjacent teeth are already compromised, a well-executed fixed bridge remains an exceptionally elegant and functional solution.”
— Prosthodontic Clinical Guidelines
Conversely, dental implants represent the most biologically conservative approach to replacing a single missing tooth, provided the adjacent teeth are healthy and unrestored. Clinical studies evaluating the long-term maintenance and survival rates of fixed partial dentures indicate that while traditional bridges are highly reliable, implant-supported restorations often demonstrate superior longevity in cases of adjacent virgin teeth[5].
When to Consult a Prosthodontist and Important Clinical Notes
Timely professional evaluation is crucial if a patient experiences pain, mobility, or gingival inflammation around an existing dental bridge to prevent further structural or periodontal damage.
Maintaining the integrity of a full dental bridge requires ongoing vigilance. According to national clinical guidelines endorsed by the Vietnam Odonto-Stomatology Association (VOSA), patients should seek immediate professional evaluation if they experience persistent discomfort, mobility of the prosthesis, or signs of gingival inflammation around the abutment teeth[6]. Early intervention can often resolve minor occlusal discrepancies or localized gingivitis before they escalate into irreversible complications such as secondary decay or abutment failure.
Dr. Nguyen Van Cuong, a leading specialist at HCMC Dental Clinic, emphasizes that comprehensive diagnostic evaluation is the cornerstone of successful prosthodontic treatment. As detailed in his clinical insights on structural tooth decay, preserving the vitality of abutment teeth while ensuring optimal marginal adaptation is critical for long-term success. Regular maintenance and adherence to a strict daily oral hygiene routine are essential to protect your investment and maintain overall oral health.

Patients are strongly advised to attend biannual dental check-ups, during which the clinician will perform a detailed radiographic and clinical assessment of the bridge margins. Utilizing specialized interdental cleaning aids, such as floss threaders or water irrigators, is non-negotiable for removing plaque from beneath the pontic and ensuring the longevity of the restoration.
Frequently Asked Questions (FAQs)
How long does a full dental bridge typically last?
A full dental bridge generally lasts between a decade to over fifteen years with proper care. Longevity depends heavily on meticulous oral hygiene, routine professional cleanings, and avoiding excessive occlusal forces such as bruxism or chewing hard objects.
Is the tooth preparation process for a bridge painful?
The preparation process is virtually painless as it is performed under local anesthesia. Patients may experience mild, temporary sensitivity in the abutment teeth for a few days following the procedure, which typically resolves on its own.
Can a dental bridge be whitened if it becomes stained?
No, the porcelain or zirconia materials used in a dental bridge do not respond to traditional bleaching agents. If the surrounding natural teeth are whitened, the bridge may need to be replaced to match the new, lighter shade.
What is the difference between a traditional bridge and a Maryland bridge?
A traditional bridge requires reshaping adjacent teeth to fit full crowns, whereas a Maryland bridge uses metal or porcelain wings bonded to the back of adjacent teeth. Maryland bridges are more conservative but generally less durable for posterior chewing forces.
How do I clean underneath my fixed dental bridge?
Cleaning under a bridge requires specialized tools such as floss threaders, interdental brushes, or a water flosser. These tools allow you to remove plaque and food debris from beneath the pontic, helping to prevent gum inflammation and secondary decay.
References
- Journal of Prosthetic Dentistry. Biomechanical considerations and Ante’s Law in fixed prosthodontics. (2021).
- International Journal of Prosthodontics. Clinical performance of monolithic zirconia vs. lithium disilicate bridges. (2020).
- Journal of the American Dental Association. Periodontal response to subgingival crown margins in fixed restorations. (2019).
- Clinical Oral Investigations. Adhesive cementation protocols for all-ceramic dental bridges. (2022).
- Journal of Clinical Periodontology. Long-term maintenance and survival rates of fixed partial dentures. (2018).
- Vietnam Odonto-Stomatology Association (VOSA). National clinical guidelines on fixed prosthodontic restorations and oral health maintenance. (2022).
For personalized advice on restorative options and to determine if a full dental bridge is the right solution for you, schedule a comprehensive consultation at HCMC Dental Clinic in Ho Chi Minh City. Our dedicated team utilizes advanced digital dentistry to provide precise, aesthetic, and long-lasting prosthodontic care tailored to your unique clinical needs.