

Experiencing a bad taste after wisdom teeth removal is a common occurrence that often stems from normal physiological healing, such as minor bleeding or temporary dry mouth. However, a persistent, foul, or metallic taste accompanied by pain may indicate underlying complications requiring immediate clinical evaluation.
Clinical Summary:
A transient bad taste following third molar extraction is frequently linked to the iron content in residual blood, the breakdown of the initial fibrin clot, or xerostomia (dry mouth) induced by post-operative medications. While these are standard aspects of the recovery timeline, a sudden shift to an intensely bitter, putrid, or salty taste can serve as an early diagnostic indicator of pathological issues. Complications such as alveolar osteitis (dry socket), localized purulent infections, or the mechanical impaction of fermenting food debris within the socket require targeted intervention. Dental professionals emphasize the importance of distinguishing between normal healing malodor and the warning signs of infection, advocating for timely clinical assessment to ensure optimal tissue regeneration and prevent systemic spread.
Key Takeaways:
- A metallic taste is a normal byproduct of trace bleeding and iron oxidation during early clot formation.
- Dry mouth (xerostomia) accelerates bacterial proliferation, leading to the release of foul-tasting volatile sulfur compounds.
- Intensely bitter or rotting tastes, especially when paired with radiating pain, are hallmark signs of dry socket.
- Trapped food debris can rapidly ferment in the extraction hole, necessitating gentle clinical or at-home irrigation.
- Persistent bad tastes lasting beyond the first week of recovery warrant a comprehensive evaluation by an oral surgeon.
Normal Physiological Causes of a Bad Taste After Extraction
A mild, temporary bad taste is a standard part of the physiological healing process, primarily caused by residual blood, clot stabilization, and temporary dry mouth.
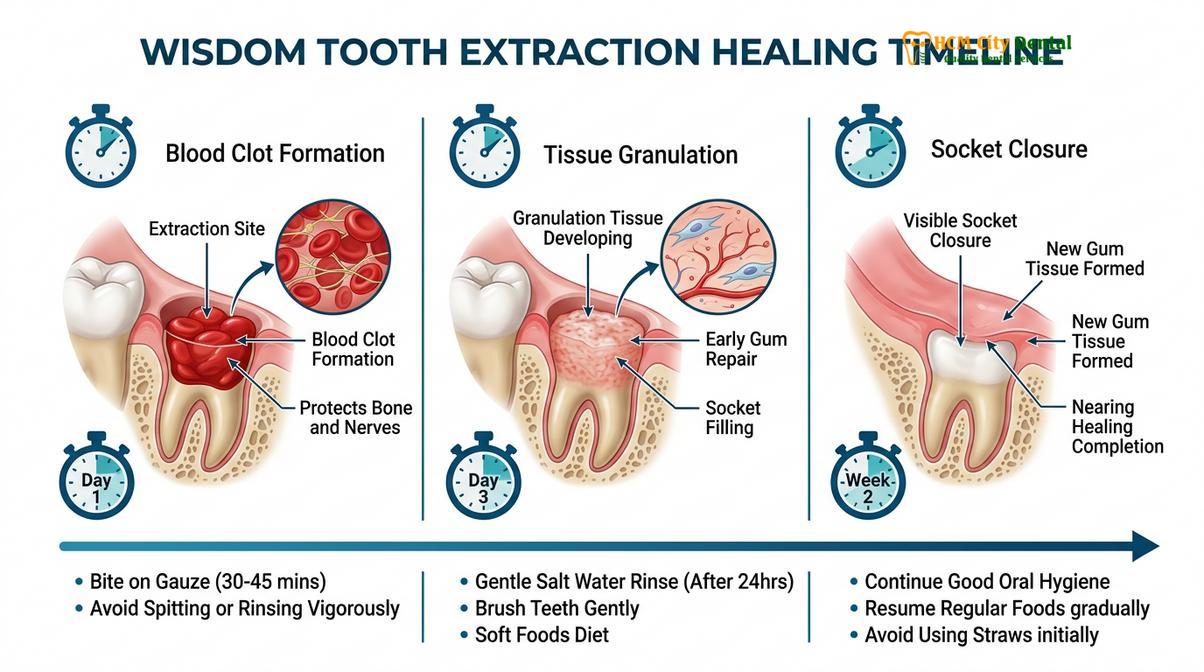
The human oral cavity is a complex biome, and any surgical intervention, such as tooth extraction, temporarily disrupts its delicate equilibrium. When a wisdom tooth is removed, the body immediately initiates a highly orchestrated cascade of biological events designed to achieve hemostasis, protect the exposed alveolar bone, and begin tissue regeneration. During these initial phases of wound healing, patients frequently report an altered gustatory perception—commonly described as a weird, metallic, or slightly sour taste. Understanding the underlying mechanisms of these normal physiological responses can help alleviate unnecessary anxiety during the recovery period.
The foremost contributor to this sensory alteration is the presence of residual blood. Following the surgical extraction of a tooth, the severed blood vessels within the periodontal ligament and surrounding medullary bone bleed into the empty socket. This bleeding is essential for the formation of the primary blood clot, which acts as a biological dressing. Blood is rich in hemoglobin, a protein complex that contains iron. As trace amounts of blood mix with saliva and wash over the taste buds, the oxidation of this iron produces a distinct, lingering metallic taste.[1] It is entirely normal for minor oozing to continue for 24 to 48 hours post-surgery, meaning this metallic sensation may persist during the early days of recovery.

Furthermore, the biochemical breakdown of the clot itself contributes to taste alterations. As the healing progresses from the inflammatory phase to the proliferative phase, the initial fibrin clot undergoes structural changes. Enzymes in the saliva and localized immune cells begin to break down cellular debris and damaged tissue. This natural enzymatic degradation releases various proteins and cellular byproducts into the oral cavity, which can temporarily impart a stale or slightly unpleasant taste. Dr. Nguyen Van Cuong, a leading specialist at HCMC Dental Clinic, frequently reassures patients that this transient malodor is a sign of active cellular remodeling rather than an immediate cause for concern.
Another significant, yet often overlooked, factor is post-operative xerostomia, commonly known as dry mouth. Saliva plays a critical role in maintaining oral health; it physically washes away food particles, buffers acidic pH levels, and contains antimicrobial enzymes like lysozyme that regulate bacterial populations. Following wisdom teeth removal, salivary flow is frequently reduced. This reduction can be attributed to several factors: the physiological stress of the surgery, mouth breathing due to localized swelling or gauze placement, and the side effects of prescribed medications, particularly opioid analgesics or certain antibiotics. When the mouth becomes dry, the anaerobic bacteria naturally present in the oral microbiome thrive. These bacteria metabolize exfoliated epithelial cells and salivary proteins, releasing volatile sulfur compounds (VSCs) such as hydrogen sulfide and methyl mercaptan.[2] These VSCs are the primary culprits behind halitosis (bad breath) and the accompanying sour or stale taste experienced during periods of reduced salivary flow.
Pathological Complications: When a Foul Taste Indicates Trouble
When a bad taste becomes persistently foul, bitter, or salty, it often signals underlying complications such as alveolar osteitis, bacterial infection, or trapped food debris.
While a mild metallic or stale taste is expected, a sudden shift to an intensely foul, putrid, or bitter taste is a clinical red flag. The oral cavity is constantly exposed to a vast array of microorganisms, and the open surgical wound left by a bottom wisdom teeth removal provides an ideal environment for opportunistic pathogens if the normal healing trajectory is disrupted. Differentiating between the taste of normal healing and the taste of a developing complication is crucial for timely intervention.
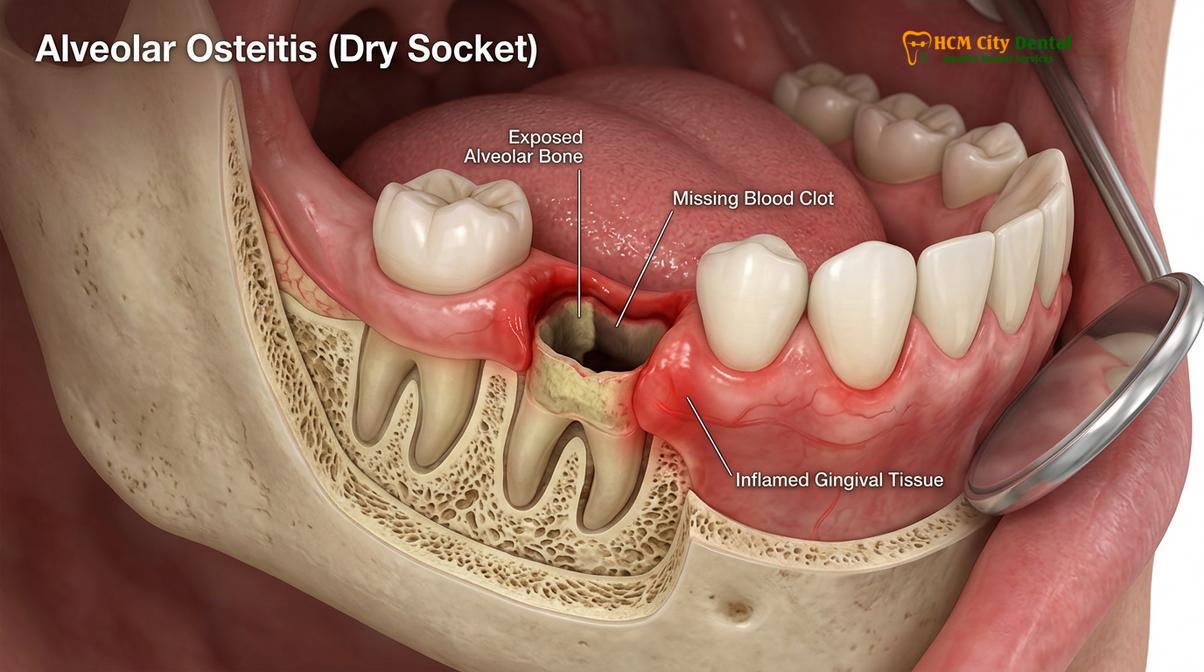
One of the most notorious complications associated with third molar extractions is alveolar osteitis, universally known as dry socket. This condition occurs when the protective blood clot that forms in the extraction site fails to develop properly, is prematurely dislodged, or dissolves before the underlying tissue has had time to granulate. The exact etiology of dry socket is multifactorial, involving an increase in localized fibrinolytic activity—where enzymes prematurely break down the fibrin network of the clot.[3] When the clot is lost, the underlying alveolar bone and highly sensitive nerve endings are left completely exposed to the oral environment.
“Alveolar osteitis is not merely a localized pain phenomenon; the exposure of necrotic bone and the subsequent bacterial colonization of the empty socket produce a highly specific, intensely foul odor and a bitter taste that patients often describe as ‘rotting.’ This sensory feedback is a direct result of tissue degradation and requires immediate palliative intervention.”
In addition to dry socket, localized bacterial infections present another significant risk. The extraction site can become a focal point for purulent exudate (pus) formation if pathogenic bacteria overwhelm the local immune defenses. Infections are more common in lower wisdom teeth due to the anatomical structure of the mandible, where gravity allows fluids and debris to pool in the socket. As the immune system dispatches neutrophils (white blood cells) to combat the invading bacteria, the resulting cellular casualties, dead bacteria, and tissue fluid combine to form pus. If this purulent material begins to drain from the surgical site into the mouth, patients will experience a distinctly salty, bitter, and highly unpleasant taste.[4] This is often accompanied by increasing localized swelling, erythema (redness), and a throbbing pain that does not respond well to standard over-the-counter analgesics.
Mechanical impaction of food debris is a less severe but highly common cause of a persistent bad taste. The removal of a large molar leaves a significant anatomical void. Even with careful eating habits, small particles of food—such as grains of rice, seeds, or soft carbohydrates—can easily become lodged deep within the socket. Because the area is tender, patients naturally avoid brushing near the surgical site, allowing this debris to remain undisturbed. Within 24 to 48 hours, the oral bacteria begin to ferment these trapped carbohydrates. This localized fermentation process produces acidic byproducts and foul-smelling gases, leading to a localized bad taste that mimics an infection but is primarily mechanical in nature. If left unaddressed, this trapped debris can irritate the healing tissue and eventually precipitate a true secondary infection.
Comprehensive Clinical Evaluation and Diagnostic Workflows
Dental professionals utilize visual inspection, gentle irrigation, and radiographic imaging to diagnose the root cause of post-extraction malodor and implement targeted therapeutic interventions.
When a patient presents with complaints of a persistent bad taste following an extraction, a systematic clinical evaluation is paramount. The diagnostic workflow is designed to accurately identify the source of the malodor, assess the integrity of the healing tissue, and rule out systemic involvement. At facilities like HCMC Dental Clinic in Ho Chi Minh City, the approach is highly methodical, prioritizing patient comfort while ensuring diagnostic accuracy.
The clinical examination begins with a thorough review of the patient’s post-operative timeline and a detailed history of their symptoms. The clinician will inquire about the exact nature of the taste (e.g., metallic vs. putrid), the onset of the symptom, and the presence of any accompanying signs such as pain, swelling, or restricted jaw movement (trismus). Following the anamnesis, a meticulous visual and tactile inspection of the surgical site is performed under high-intensity operatory lighting. The dentist evaluates the socket for the presence of a stable, organizing blood clot, the color and contour of the surrounding gingival margins, and any visible signs of purulent discharge or trapped debris.
If the visual inspection reveals an empty socket with exposed bone, the diagnosis of alveolar osteitis is confirmed. The treatment workflow for dry socket focuses on palliative care rather than curative surgery, as the condition is self-limiting but highly painful. The clinician will first gently irrigate the socket with sterile saline or a dilute chlorhexidine gluconate solution to remove any necrotic debris or food particles. Following irrigation, a medicated intra-alveolar dressing is carefully packed into the void. These dressings typically contain a combination of eugenol (an essential oil with potent analgesic and antibacterial properties), a topical anesthetic like butamben, and an antimicrobial agent such as iodoform. The dressing provides almost immediate pain relief and physically blocks the socket from further food impaction, eliminating the foul taste associated with the exposed bone.

In cases where a localized infection is suspected, the diagnostic protocol may include radiographic imaging. A panoramic radiograph or a localized periapical X-ray can help the clinician assess the underlying bone for signs of osteomyelitis or to ensure that no root fragments or foreign bodies were inadvertently left behind during the initial surgery. If a fluctuant swelling (an abscess) is present, the clinician may need to perform a minor incision and drainage procedure to evacuate the purulent material, immediately resolving the salty/bitter taste. Systemic antibiotics, such as Amoxicillin or Clindamycin, are typically prescribed only when there is clear evidence of spreading infection, such as facial cellulitis or lymphadenopathy, rather than for localized socket inflammation.[5]
| Symptom Profile | Primary Taste Description | Accompanying Clinical Signs | Probable Diagnosis | Standard Clinical Action |
|---|---|---|---|---|
| Days 1-3 Post-Op | Metallic, slightly sour | Minor blood oozing, normal post-op swelling, manageable discomfort | Normal physiological healing | Observation, gentle saline rinses, standard oral hygiene |
| Days 3-5 Post-Op | Intensely bitter, rotting | Severe radiating pain, empty socket, loss of blood clot, bad breath | Alveolar Osteitis (Dry Socket) | Clinical irrigation, placement of medicated eugenol dressing |
| Days 4-7+ Post-Op | Salty, foul, putrid | Increasing swelling, throbbing pain, visible pus, possible fever | Localized Bacterial Infection | Incision and drainage, antimicrobial therapy, possible antibiotics |
| Variable (Days 3+) | Stale, sour, garbage-like | Feeling of pressure in socket, visible debris, mild gingival inflammation | Food Impaction | Mechanical debridement, instruction on monojet syringe use |
Clinical Case Review: Managing Post-Extraction Malodor
A 24-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City five days after the surgical removal of an impacted lower right third molar. The patient reported a sudden onset of a “rotting” taste in their mouth, accompanied by a dull ache that radiated to their right ear. Clinical examination revealed the absence of the primary blood clot and localized accumulation of food debris within the deep socket. The surrounding tissues showed mild erythema but no signs of fluctuant swelling or purulent exudate. The diagnosis of mild alveolar osteitis complicated by food impaction was established. The attending oral surgeon performed gentle irrigation with 0.12% chlorhexidine to flush out the fermenting debris, immediately neutralizing the foul taste. A soothing eugenol-based dressing was placed, and the patient was instructed on proper at-home irrigation techniques. Complete resolution of the bad taste and pain was achieved within 48 hours.
Advanced Prevention and At-Home Care Strategies
Proactive oral hygiene, including gentle saline rinses and proper mechanical cleaning, is essential to prevent bacterial accumulation and food impaction during the recovery phase.
The success of a tooth extraction recovery relies heavily on the patient’s adherence to post-operative care instructions. Preventing a bad taste requires a delicate balance: maintaining rigorous oral hygiene to minimize bacterial load while simultaneously protecting the fragile healing tissue from mechanical disruption. A structured, phased approach to at-home care is the most effective strategy for ensuring a smooth, odor-free recovery.
During the first 24 to 48 hours, the primary objective is clot preservation. Patients must strictly avoid any actions that create negative pressure in the oral cavity, such as smoking, vaping, using drinking straws, or vigorous spitting. These actions can easily dislodge the newly formed clot, leading directly to dry socket. Oral hygiene during this initial phase should be modified; patients should continue to brush their teeth but must carefully avoid the surgical sites. Rinsing should be entirely avoided on the first day to prevent washing away the stabilizing fibrin network.
Starting on the second or third day, gentle rinsing becomes a critical component of preventing malodor. A warm saline solution (half a teaspoon of salt dissolved in eight ounces of warm water) is highly recommended. Salt water acts as a mild, natural antiseptic, altering the osmotic balance of the oral environment to inhibit bacterial growth while soothing inflamed tissues. Patients should gently bathe the surgical site by tilting their head, allowing the fluid to pool over the area, and then letting it passively fall out of the mouth into the sink, rather than forcefully spitting.
As healing progresses into the second week, the risk of dislodging the clot diminishes, but the risk of food impaction increases as the socket begins to close from the bottom up. At this stage, many oral surgeons provide patients with a curved plastic monojet syringe. This tool is invaluable for targeted irrigation. Patients are instructed to fill the syringe with warm salt water or a prescribed antimicrobial rinse, place the curved tip just inside the edge of the socket, and gently flush the area after every meal. This mechanical flushing is the most effective way to remove fermenting food debris and eliminate the associated bad taste.
“Aggressive brushing or the premature use of high-pressure water flossers near an extraction site can severely traumatize granulating tissue and delay healing. Mechanical cleaning must be reintroduced gradually, respecting the biological timeline of tissue regeneration.”
Once the surgical site has significantly closed and the soft tissue has re-epithelialized—typically around the third week—patients can begin to normalize their oral hygiene routine. It is at this stage that tools like a mono-tufted brush or carefully maneuvering wisdom dental floss around the adjacent second molars can be safely reintroduced. Using wisdom dental floss helps remove plaque that may have accumulated on the distal surface of the neighboring tooth during the period of modified brushing, further reducing the overall bacterial load and improving breath freshness. However, direct flossing into the healing socket itself should always be avoided until cleared by a dental professional.
When to See a Doctor: Critical Warning Signs
While many post-operative symptoms can be managed with diligent at-home care, certain clinical presentations require immediate professional intervention. Relying solely on internet research or home remedies when facing aggressive symptoms can lead to severe, rapidly spreading infections. It is crucial to understand the threshold between normal healing discomfort and pathological warning signs.
You should seek immediate evaluation from an oral surgeon or visit a facility like HCMC Dental Clinic if the bad taste in your mouth is accompanied by any of the following systemic or localized symptoms. A persistent, foul taste that does not improve with gentle saline irrigation after several days is a primary indicator that the normal healing process has been compromised. If this taste is paired with a sudden escalation in pain—particularly pain that throbs, radiates to the ear, temple, or neck, and is unresponsive to prescribed pain medication—it is highly indicative of a dry socket or a deep tissue infection.
Urgent Clinical Warning Signs
Immediate medical attention is required if you experience:
- Visible yellow, green, or white purulent discharge (pus) oozing from the extraction site.
- Progressive swelling of the face, jaw, or neck that worsens after the third day post-surgery.
- Systemic symptoms including a fever above 101°F (38.3°C), chills, or swollen lymph nodes.
- Severe trismus (inability to open the mouth more than a few millimeters) or difficulty swallowing and breathing.
Furthermore, if you notice that the bad taste is specifically triggered when you attempt to clean the adjacent teeth, even when cautiously using wisdom dental floss, it may indicate that a periodontal pocket has formed or that the adjacent tooth’s root has been compromised. Never attempt to forcefully dig out suspected food debris with toothpicks, tweezers, or aggressive water flossing, as this can cause severe lacerations and drive bacteria deeper into the medullary bone. Always defer to a clinical examination for a safe, definitive diagnosis and appropriate therapeutic management. For comprehensive care and expert evaluation of any post-extraction concerns, consulting the general dental guide and scheduling a follow-up appointment is the safest course of action.

Frequently Asked Questions
How long does a bad taste last after wisdom teeth removal?
A mild bad taste typically lasts for 3 to 7 days as the initial blood clot stabilizes and minor oozing stops. During this initial week, the body is actively remodeling the surgical site, and the breakdown of cellular debris naturally produces temporary malodor. If the foul taste persists beyond a week, or if it progressively worsens instead of improving, it requires clinical evaluation to rule out complications like infection, dry socket, or deeply impacted food debris.
Is a metallic taste normal after tooth extraction?
Yes, a metallic taste is entirely normal during the first few days of recovery. It is caused by the iron content in the trace amounts of blood that naturally ooze from the surgical site as the body forms a protective clot. As this minor bleeding subsides and the clot fully solidifies—usually within 48 to 72 hours—the metallic sensation should gradually fade. Gentle salt water rinses can help neutralize this taste without disrupting the healing tissue.
Can trapped food cause a bad taste in the extraction hole?
Absolutely. Food debris trapped in the extraction socket can rapidly ferment due to oral bacteria, producing volatile sulfur compounds that cause a noticeably foul taste and odor. Because the extraction site creates a physical void, small particles like rice or seeds easily accumulate. While this is not an infection initially, the fermenting debris irritates the tissue and causes malodor. Gentle irrigation with a curved syringe is usually required to dislodge these particles safely.
What does a dry socket taste like?
Patients often describe the taste of a dry socket as intensely bitter, foul, or rotting. This is accompanied by severe, radiating pain that typically begins three to five days after the extraction, signaling the premature loss of the blood clot. Without the protective clot, the underlying bone and nerves are exposed to the oral environment, leading to localized tissue necrosis and bacterial colonization, which directly produces the characteristic putrid taste and severe discomfort.
When can I start using wisdom dental floss around the extraction site?
You should wait until the surgical site has significantly healed and closed, usually after two to three weeks, before using wisdom dental floss near the area. Premature flossing near the socket can accidentally lacerate the fragile granulating tissue or dislodge the healing clot. Once the oral surgeon confirms that the soft tissue has sufficiently closed, you can carefully resume flossing the adjacent second molars to maintain optimal hygiene and prevent plaque buildup.
References
- Journal of Oral and Maxillofacial Surgery. Pathophysiology and clinical management of alveolar osteitis. (2021).
- International Journal of Oral Science. Volatile sulfur compounds and oral malodor post-extraction. (2020).
- British Dental Journal. Clinical protocols for third molar extraction complications and wound healing. (2019).
- Journal of the American Dental Association. Efficacy of chlorhexidine in preventing alveolar osteitis and surgical site infections. (2022).
- Clinical Oral Investigations. Microbiological profile and biochemical analysis of infected extraction sockets. (2018).



