

The average lumineers cost per tooth typically ranges from $800 to $2,000 in Western healthcare markets, though international dental facilities often provide these premium ultra-thin restorations at a significantly reduced price. Exact clinical pricing depends on the complexity of the smile design, geographic location, and the cosmetic dentist’s specialized expertise.
Clinical Summary:
Lumineers represent a highly specialized category of ultra-thin porcelain veneers designed to require minimal to zero enamel reduction. While the initial financial investment reflects the proprietary Cerinate ceramic material and specialized laboratory fabrication processes, their exceptional long-term survival rate and conservative clinical approach make them a highly viable option for patients seeking mild to moderate aesthetic corrections. Comprehensive diagnostic imaging, periodontal evaluation, and precise occlusal analysis are absolute prerequisites to determine patient candidacy, ensure optimal marginal adaptation, and guarantee the long-term structural integrity of the restorations.
Key Takeaways:
- The global financial investment for ultra-thin veneers varies significantly based on geographic location, clinical overhead, and provider specialization.
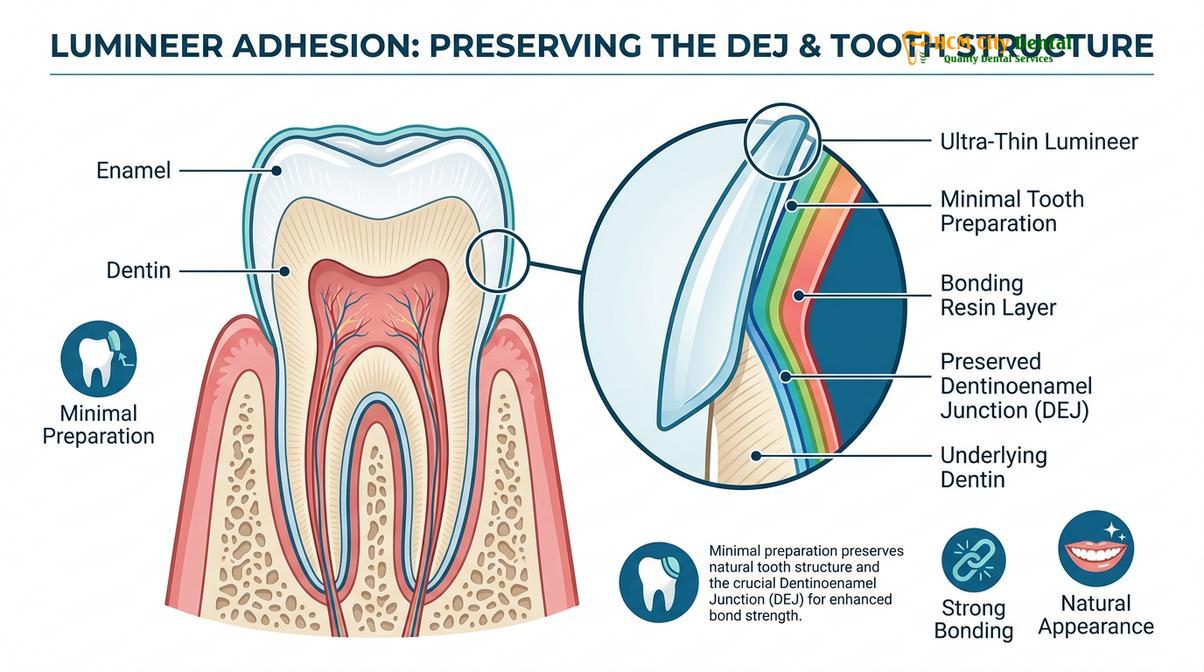
- These proprietary restorations preserve maximum natural tooth structure by utilizing a minimal-prep or no-prep clinical protocol.
- Optimal candidacy is crucial; patients presenting with severe intrinsic discoloration or significant malocclusion may require alternative restorative approaches.
- Long-term clinical success relies heavily on maintaining excellent gingival health and a stable, balanced occlusal bite.
- Selecting a highly credentialed cosmetic dentist ensures precise marginal fit, preventing plaque accumulation and achieving natural optical translucency.
What Determines the Lumineers Cost Per Tooth?
The financial investment required for each restoration is primarily driven by the proprietary Cerinate porcelain material, exclusive laboratory fabrication fees, and the geographic location of the treating dental practice.
When evaluating the lumineers cost per tooth, patients must understand that they are not merely paying for a piece of ceramic; they are investing in advanced material science, specialized clinical workflows, and the preservation of their natural biological tooth structure. Unlike generic composite bonding or standard ceramic shells, Lumineers are fabricated from a highly specific, proprietary material known as Cerinate porcelain. This unique glass-ceramic formulation allows the restoration to be pressed to an ultra-thin dimension—often as thin as 0.2 millimeters, comparable to the thickness of a contact lens—without sacrificing the flexural strength required to withstand the dynamic forces of human mastication[1].
The proprietary nature of this material means that the clinical impressions or digital scans must be sent to specialized, certified dental laboratories. The laboratory technicians utilize advanced CAD/CAM (Computer-Aided Design and Computer-Aided Manufacturing) technology alongside meticulous hand-layering techniques to create a restoration that mimics the natural light-scattering properties of human enamel. These exclusive laboratory fees constitute a significant portion of the overall treatment cost.

Furthermore, the clinical expertise of the treating physician plays a paramount role in the pricing structure. Placing a minimal-prep veneer is arguably more technically demanding than placing a traditional veneer. Because the dentist is not removing a significant layer of enamel to create a “seating margin” for the ceramic, they must possess an exceptional understanding of emergence profiles and gingival contours to ensure the final restoration does not appear bulky or create a plaque-retentive ledge at the gumline. Dr. Nguyen Van Cuong, a leading specialist in cosmetic restorations, frequently emphasizes that the true value of a premium veneer lies in the meticulous diagnostic planning and the precision of the adhesive bonding protocol, rather than just the physical ceramic itself.
“The integration of ultra-thin ceramics requires a profound respect for the periodontium. A restoration that is merely bonded to the tooth without precise marginal adaptation will inevitably lead to localized gingival inflammation, compromising both the aesthetic outcome and the biological health of the patient.”
Geographic location also heavily influences the final fee schedule. Dental practices operating in high-cost urban centers in North America or Western Europe face substantial overhead costs, including facility leasing, staff compensation, and regulatory compliance, which are inevitably reflected in the patient’s final bill. Conversely, internationally accredited clinics in emerging medical hubs can offer the exact same proprietary materials and clinical protocols at a fraction of the cost, a concept that will be explored further in the context of global dental economics.
Lumineers vs. Traditional Veneers: A Clinical and Financial Comparison
While Lumineers offer a highly conservative, minimal-prep approach that preserves enamel, traditional veneers provide greater structural thickness necessary for masking severe discoloration or correcting moderate misalignment.
A comprehensive understanding of the lumineers cost per tooth requires a direct clinical comparison with traditional porcelain veneers. Both modalities aim to enhance the aesthetic appearance of the anterior dentition, but their biomechanical principles, preparation requirements, and specific clinical indications differ significantly. Patients exploring General Dentistry options for smile enhancement must undergo a thorough diagnostic evaluation to determine which restorative pathway aligns with their anatomical realities and aesthetic goals.
Traditional porcelain veneers typically require the irreversible removal of 0.5 to 0.8 millimeters of facial enamel. This subtractive preparation serves two critical purposes: it creates physical space for the ceramic material so the final tooth does not appear artificially bulky, and it allows the ceramist to incorporate opaque masking layers to hide severe intrinsic stains, such as those caused by tetracycline exposure or endodontic treatment. Because traditional veneers are thicker, they offer the clinician greater latitude in altering the shape, length, and apparent alignment of the teeth.
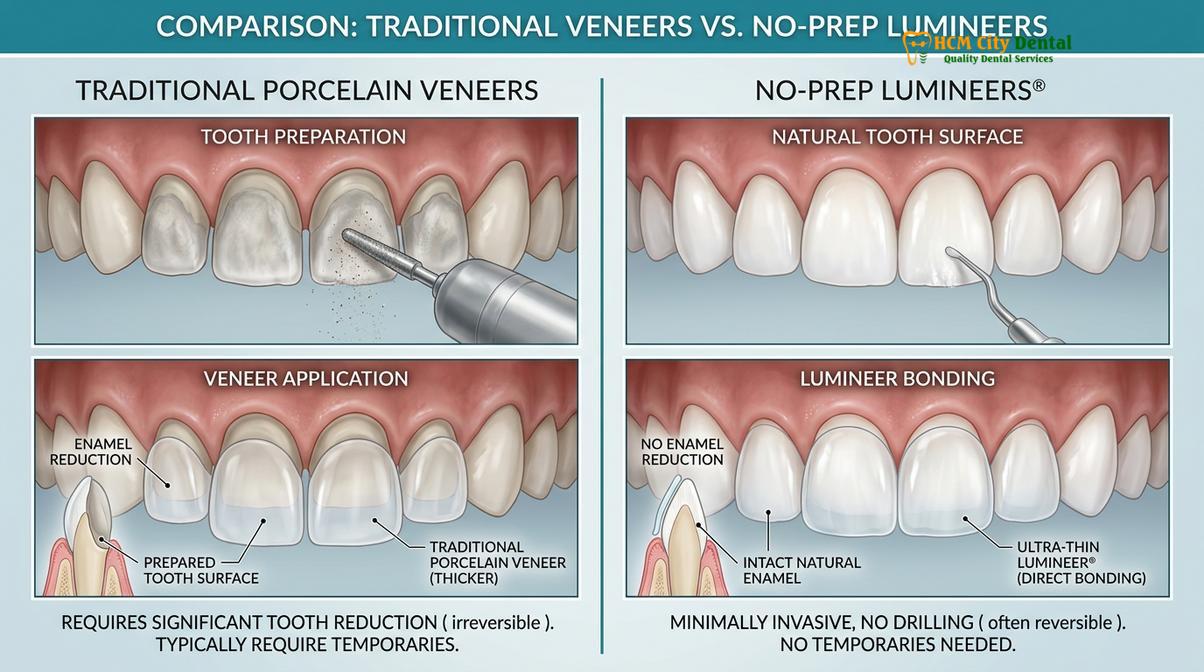
In contrast, Lumineers are championed for their additive, minimal-prep philosophy. Because they are exceptionally thin, they can often be bonded directly to the unprepared or minimally contoured enamel surface. This preservation of the enamel layer is biologically advantageous; the shear bond strength of dental resin cement to natural enamel is significantly higher and more predictable than its bond to the underlying dentin layer[2]. Consequently, restorations bonded entirely to enamel exhibit superior long-term retention rates and a lower incidence of microleakage.
| Clinical Parameter | Ultra-Thin Lumineers | Traditional Porcelain Veneers |
|---|---|---|
| Enamel Preparation | Minimal to none (highly conservative) | 0.5mm – 0.8mm reduction (irreversible) |
| Material Thickness | Approx. 0.2mm – 0.3mm | Approx. 0.5mm – 1.0mm |
| Anesthesia Requirement | Rarely required | Typically required during preparation |
| Stain Masking Ability | Low to Moderate (highly translucent) | High (can incorporate opaque layers) |
| Reversibility | Potentially reversible (enamel intact) | Irreversible (requires lifelong coverage) |
Financially, the cost per unit for both options is often comparable within the same geographic market. While Lumineers require less clinical chair time for tooth preparation, the specialized laboratory fees associated with the proprietary Cerinate porcelain often offset those savings. Patients interested in a deeper dive into the material science and aesthetic outcomes of these specific restorations can review our comprehensive Porcelain Lumineers: Clinical Guide & Comparison | HCMC Dental.
The Clinical Workflow for Ultra-Thin Veneer Placement
The successful placement of minimal-prep veneers involves a meticulous multi-step workflow, encompassing precise digital diagnostics, specialized laboratory fabrication, and highly controlled adhesive bonding protocols.
The journey to a restored smile via ultra-thin ceramics is a highly orchestrated clinical process. It begins with a comprehensive diagnostic phase. The clinician must evaluate the patient’s periodontal health, occlusal dynamics (bite relationship), and overall facial aesthetics. Active periodontal disease or untreated dental caries must be resolved prior to any cosmetic intervention. Additionally, the dentist will perform a functional analysis to ensure the patient’s bite forces will not place undue stress on the delicate ceramic margins.
Once candidacy is confirmed, the clinical workflow proceeds to the data acquisition phase. Modern cosmetic practices utilize advanced intraoral 3D scanners to capture highly accurate digital impressions of the dental arches. These digital files, along with a series of standardized clinical photographs, are transmitted to the specialized dental laboratory. The ceramists then utilize digital smile design software to engineer the restorations, ensuring optimal proportions, symmetry, and functional harmony with the opposing dentition.

Clinical Case Study: Minimal-Prep Smile Makeover
A 32-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City with concerns regarding mild diastemas (spacing) and slight enamel wear on the maxillary anterior teeth. Because the patient possessed healthy, bright underlying enamel and a stable occlusal relationship, Dr. Cuong recommended a conservative approach utilizing ultra-thin Cerinate veneers. By avoiding aggressive enamel reduction, the clinical team successfully closed the interdental spaces and restored the incisal edges while maintaining the biological integrity of the natural teeth. The final result demonstrated exceptional optical integration and optimal gingival health at the one-year follow-up.
The final, and arguably most critical, phase is the adhesive bonding protocol. Because Lumineers are so thin, the color of the underlying tooth and the shade of the resin cement will directly influence the final aesthetic outcome. The clinician will first perform a “try-in” using water-soluble try-in pastes to verify the fit and allow the patient to approve the color. Once approved, the teeth are isolated to prevent moisture contamination. The enamel is treated with a mild phosphoric acid etchant to create microscopic porosities, while the internal surface of the ceramic is treated with hydrofluoric acid and a silane coupling agent[3]. A premium light-cured resin cement is then used to chemically fuse the ceramic to the enamel, creating a monolithic, highly durable structure.
International Cost Variations and Dental Tourism
Patients are increasingly leveraging global dental tourism to access premium cosmetic dentistry, securing high-quality ultra-thin veneers at a fraction of the cost found in their home countries.
The globalization of healthcare has profoundly impacted the cosmetic dental industry. The lumineers cost per tooth in regions like North America, the United Kingdom, and Australia is heavily inflated by high domestic overhead costs, stringent insurance administration fees, and elevated laboratory expenses. As a result, a full smile makeover involving eight to ten anterior teeth can represent a prohibitive financial burden for many individuals.
This economic disparity has fueled the rise of dental tourism, with Southeast Asia emerging as a premier destination for world-class restorative care. Clinics in metropolitan centers like Ho Chi Minh City have invested heavily in state-of-the-art digital infrastructure, CBCT imaging, and international accreditation. These facilities are staffed by highly credentialed specialists who frequently undergo advanced training in Europe or the United States, ensuring that the clinical standards meet or exceed global benchmarks.
Important Clinical Warning Regarding Dental Tourism
While international treatment offers significant financial advantages, patients must exercise rigorous due diligence when selecting an overseas provider. Ensure the clinic utilizes authentic, verifiable dental materials and adheres to strict international sterilization protocols. Furthermore, complex restorative cases require adequate time for laboratory fabrication and post-operative evaluation; patients should never rush a medical procedure to fit a tight vacation schedule.
By traveling to a reputable facility like HCMC Dental Clinic, patients can often reduce their total treatment expenditure by up to 60-70%, even when factoring in the costs of international flights and premium accommodations. For patients seeking to manage their investment effectively, many modern clinics also provide structured financial solutions. You can learn more about navigating these options in our comprehensive resource: Dentist That Offer Payment Plans: Clinical Guide | HCMC Dental. This globalization of care democratizes access to advanced aesthetic dentistry, allowing more patients to achieve optimal oral health and confidence[4].
When to See a Doctor for Cosmetic Dental Assessment
Deciding to pursue cosmetic dental enhancements requires a professional clinical assessment to ensure the chosen treatment aligns with your biological health and functional needs. Patients should schedule a formal consultation with a credentialed cosmetic dentist if they experience persistent dissatisfaction with the color, shape, or alignment of their anterior teeth, or if they have sustained minor structural damage such as chips or micro-fractures.
However, it is critical to understand that cosmetic restorations are not a substitute for foundational oral healthcare. If a patient is experiencing symptoms of active dental pathology—such as spontaneous toothache, bleeding gums, tooth mobility, or chronic halitosis—these issues must be diagnosed and treated prior to any aesthetic intervention. Placing a ceramic veneer over an actively decaying tooth or inflamed periodontal tissue will inevitably lead to severe clinical complications, including restoration failure and potential tooth loss.

Furthermore, patients who exhibit signs of severe bruxism (chronic teeth grinding or clenching) must be evaluated carefully. The excessive occlusal forces generated during bruxism can easily fracture even the strongest ceramic materials. In such cases, the clinician may recommend alternative restorative strategies or mandate the nightly use of a custom-fabricated occlusal splint to protect the investment. If underlying alignment issues are severe, orthodontic intervention may be required first; patients can explore these options in our guide on Invisalign vs Braces Cost: Clinical Guide & Pricing | HCMC Dental.
“Aesthetic dentistry must always be built upon a foundation of absolute biological health. The most beautiful ceramic restoration in the world will fail if the underlying periodontium is compromised or if the biomechanical forces of the patient’s bite are ignored during the diagnostic phase.”
Routine preventive care remains the cornerstone of oral health. Before embarking on a smile makeover, ensure your foundational hygiene is optimal by reviewing resources like How Much Does a Teeth Cleaning Cost Without Insurance | HCMC Dental. Additionally, if impacted third molars are causing crowding or discomfort, a surgical consultation may be necessary, as detailed in our Best Dentist for Wisdom Teeth Removal: Clinical Guide | HCMC Dental. A comprehensive, multidisciplinary approach is the only way to ensure long-lasting, predictable clinical outcomes[5].
Frequently Asked Questions
Are Lumineers covered by standard dental insurance?
No, standard dental insurance typically does not cover the Lumineers cost per tooth because it is classified as an elective cosmetic procedure. However, if a veneer is deemed medically necessary to restore structural integrity after trauma, partial coverage may occasionally apply. Patients should consult their insurance provider and clinic financial coordinator to explore available payment plans or third-party financing options.
How long do ultra-thin Lumineers typically last?
With proper oral hygiene and a stable occlusal bite, Lumineers can last between 10 to 20 years. Their longevity is heavily dependent on the quality of the adhesive bond to the natural enamel and the patient’s daily habits. Avoiding excessive bite forces, wearing a nocturnal occlusal guard if bruxism is present, and maintaining regular professional periodontal cleanings will significantly extend the lifespan of the restorations.
Can Lumineers be removed later if I change my mind?
Yes, because Lumineers require minimal to no enamel reduction, the procedure is generally considered more reversible than traditional veneers. However, the removal process requires meticulous clinical precision to safely dissolve or polish away the high-strength resin cement without damaging the underlying natural enamel. A professional cosmetic dentist must perform this delicate procedure to ensure the tooth structure remains intact.
Do no-prep veneers look bulky on natural teeth?
Lumineers are fabricated to be ultra-thin (approximately 0.2 mm), which minimizes added bulk, but improper case selection can lead to a slightly thicker appearance. If a patient’s natural teeth are already prominent or slightly misaligned, adding even a thin ceramic layer without any enamel preparation can alter the emergence profile. A skilled clinician will carefully evaluate the arch form to ensure a natural, seamless aesthetic.
Is the Lumineers placement procedure painful?
The Lumineers placement procedure is virtually painless and typically does not require local anesthesia. Because the protocol involves minimal or no drilling into the sensitive dentin layer of the tooth, patients rarely experience intraoperative discomfort. Some individuals may notice mild, transient thermal sensitivity immediately following the bonding process, but this usually resolves within a few days as the teeth acclimate to the new restorations.
References
- Journal of Esthetic and Restorative Dentistry. Clinical performance of ultra-thin porcelain veneers: A long-term survival analysis. (2021).
- International Journal of Periodontics & Restorative Dentistry. Periodontal response to minimal-prep and no-prep ceramic veneers. (2020).
- Journal of Prosthetic Dentistry. Adhesive protocols and shear bond strength of Cerinate porcelain to enamel and dentin. (2019).
- British Dental Journal. Health economics and cost-benefit analysis of cosmetic dental tourism in Southeast Asia. (2022).
- American Dental Association (ADA). Clinical guidelines on the indications and contraindications for conservative aesthetic restorations. (2018).



