Yes, you can get dental implants even if you have experienced significant bone loss. Advanced clinical techniques, including bone grafting, sinus lifts, and specialized zygomatic implants, allow oral surgeons to rebuild or bypass deficient bone, providing a stable foundation for permanent tooth replacement.
Clinical Summary:
Patients presenting with jawbone atrophy are no longer disqualified from receiving implant-supported prosthetics. Modern implantology utilizes sophisticated regenerative procedures to restore lost alveolar volume or employs anatomically adapted implants that anchor into denser facial bones. The appropriate clinical pathway depends on the severity of resorption, the anatomical location of the defect, and the patient’s systemic health. Through comprehensive 3D imaging and precise surgical protocols, even cases of severe maxillary or mandibular deficiency can be successfully rehabilitated, restoring both masticatory function and facial aesthetics.
Key Takeaways:
- Bone loss occurs naturally after tooth extraction due to the absence of mechanical stimulation in the alveolar ridge.
- Bone grafting for implants can successfully rebuild localized defects before or during fixture placement.
- Sinus lifts increase vertical bone height in the posterior maxilla to safely accommodate titanium roots.
- Zygomatic dental implants offer a graftless solution for severe upper jawbone loss by anchoring directly into the cheekbone.
- Comprehensive 3D CBCT imaging is mandatory to assess bone density and plan the appropriate surgical intervention.
What Causes Jawbone Loss After Tooth Loss?
Jawbone loss primarily occurs because the alveolar bone requires constant mechanical stimulation from chewing forces transmitted through tooth roots to maintain its density and structural volume.
The human skeletal system is highly dynamic, constantly undergoing a process of remodeling where old bone is resorbed by osteoclasts and new bone is formed by osteoblasts. In the oral cavity, the alveolar bone—the specialized portion of the jawbone that houses the teeth—relies heavily on the mechanical stress generated during mastication (chewing). When a tooth is extracted or lost to disease, this vital stimulation ceases abruptly. According to Wolff’s Law of bone adaptation, bone that is not subjected to mechanical loading will gradually atrophy. Within the first six months following a tooth extraction, the surrounding alveolar ridge can lose up to 25% of its initial volume, with the resorption process continuing at a slower rate indefinitely[1].

Beyond disuse atrophy, several other pathological factors contribute to the degradation of jawbone architecture. Periodontal disease is the leading cause of bone loss in adults. Pathogenic bacteria accumulate in periodontal pockets, triggering a chronic inflammatory response. The body’s immune system, in an attempt to isolate the infection, inadvertently destroys the periodontal ligament and the supporting alveolar bone. If left untreated, this progressive destruction leads to tooth mobility and eventual loss, leaving behind a highly compromised bony foundation that complicates future restorative efforts.
“The preservation of alveolar bone is a race against time following tooth extraction. Without immediate intervention or the placement of an implant to mimic the natural root, the inevitable dimensional changes of the ridge can severely limit future prosthetic options.”
Furthermore, the long-term use of traditional removable dentures can actually accelerate bone resorption. Because conventional dentures rest directly on the soft mucosal tissues, the compressive forces of chewing are transferred to the underlying bone surface rather than being distributed internally through a root structure. This constant friction and pressure exacerbate the rate of atrophy, leading to the classic “sunken” facial appearance often seen in edentulous patients. Dr. Nguyen Van Cuong frequently emphasizes to patients that exploring Dental Implants early is the most effective strategy to halt this degenerative cycle and preserve facial structural integrity.
Trauma to the maxillofacial region, congenital anomalies, and certain systemic conditions or medications (such as long-term corticosteroid use) can also negatively impact bone density. Understanding the specific etiology of a patient’s bone loss is the critical first step in formulating effective jawbone resorption solutions that will yield predictable, long-term success.
The Impact of Bone Resorption on Traditional Implants
Severe bone resorption compromises the primary stability of traditional implants, increasing the risk of implant failure, nerve damage, or sinus perforation if placed without prior augmentation.
For a dental implant to function successfully over a patient’s lifetime, it must achieve osseointegration—a direct structural and functional connection between living bone and the surface of the load-bearing artificial implant. This biological process relies heavily on the initial mechanical stability of the implant at the time of surgery, known as primary stability. When a patient presents with inadequate bone volume, achieving this crucial primary stability becomes highly challenging. The implant fixture requires a minimum circumference of healthy bone (typically at least 1.5 to 2 millimeters of bone on all sides) to withstand the immense occlusal forces generated during chewing[2].
When attempting to place traditional implants in a severely resorbed ridge, oral surgeons face significant anatomical limitations. In the lower jaw (mandible), vertical bone loss brings the crest of the ridge dangerously close to the inferior alveolar nerve canal. This nerve supplies sensation to the lower lip and chin. Placing an implant without sufficient vertical bone height risks impinging upon or severing this nerve, which can result in temporary or permanent paresthesia (numbness). Consequently, patients seeking dental implants with severe bone loss in the mandible require meticulous 3D planning to avoid catastrophic neurological complications.
Clinical Warning: Attempting to place standard dental implants into inadequate bone volume without appropriate regenerative procedures significantly increases the risk of early implant failure, peri-implantitis, and damage to adjacent anatomical structures such as nerves and sinus cavities.
In the upper jaw (maxilla), the primary anatomical constraint is the maxillary sinus. Following the loss of upper posterior teeth, the sinus cavity often expands downward into the space previously occupied by the tooth roots—a process known as pneumatization. Combined with the upward resorption of the alveolar ridge, the remaining bone separating the oral cavity from the sinus can become paper-thin. Placing an implant into this compromised space without intervention risks perforating the Schneiderian membrane, potentially leading to acute sinusitis or the displacement of the implant into the sinus cavity.
Furthermore, inadequate bone width can lead to fenestrations (window-like defects) or dehiscences (cleft-like defects) where the titanium threads of the implant are exposed through the bone. These exposures are highly susceptible to bacterial colonization, leading to peri-implant mucositis and eventual implant failure. Therefore, addressing bone deficiencies is not merely an aesthetic consideration; it is a fundamental biomechanical requirement for the survival of the prosthetic restoration.
Clinical Solution 1: Alveolar Bone Grafting & Ridge Preservation
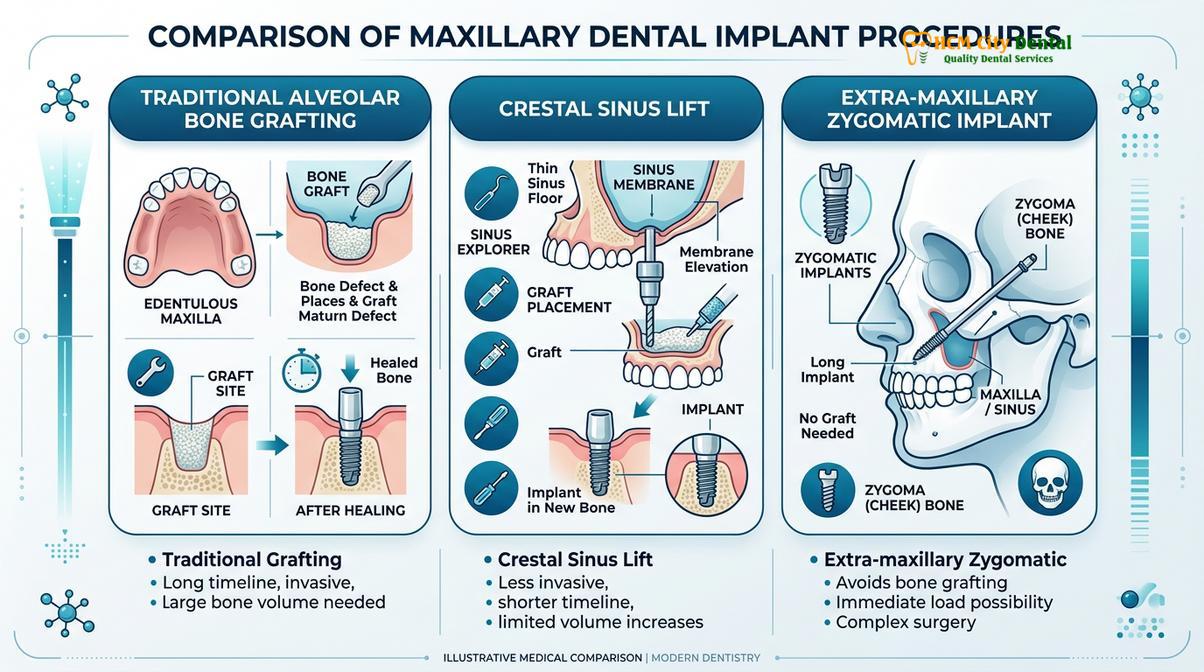
Alveolar bone grafting restores missing bone volume by placing graft material into the deficient site, acting as a scaffold for the body to regenerate its own natural bone over several months.
When diagnostic imaging reveals insufficient bone volume for immediate implant placement, alveolar bone grafting is the standard clinical protocol. This regenerative procedure aims to reconstruct the lost dimensions of the alveolar ridge, ensuring that the future implant will be entirely encased in healthy, dense bone. The fundamental principle behind bone grafting is osteoconduction—the graft material serves as a physical scaffold or framework into which the patient’s own osteoblasts (bone-forming cells) can migrate, proliferate, and deposit new bone matrix[3].

There are several classifications of bone graft materials utilized in modern implantology, each selected based on the specific requirements of the defect and the patient’s medical profile. Autografts involve harvesting bone from another site within the patient’s own body (such as the chin, ascending ramus, or hip). While autografts are considered the gold standard due to their osteogenic properties (containing living bone cells), they require a secondary surgical site. Allografts utilize processed bone from a human donor, while xenografts are derived from an animal source (typically bovine or porcine). Alloplasts are entirely synthetic materials, such as calcium phosphate or hydroxyapatite. These alternatives eliminate the need for a second surgical site and have demonstrated excellent clinical efficacy in routine ridge augmentation.
| Graft Type | Source Material | Primary Mechanism | Clinical Application |
|---|---|---|---|
| Autograft | Patient’s own bone | Osteogenic, Osteoinductive, Osteoconductive | Severe defects requiring rapid, robust regeneration. |
| Allograft | Human donor (tissue bank) | Osteoinductive, Osteoconductive | Routine ridge augmentation, socket preservation. |
| Xenograft | Animal source (bovine/porcine) | Osteoconductive | Sinus lifts, maintaining long-term volume stability. |
| Alloplast | Synthetic (calcium phosphate) | Osteoconductive | Small localized defects, patients refusing animal/human products. |
A highly effective technique frequently employed is Guided Bone Regeneration (GBR). In this procedure, the bone graft material is packed into the defect and subsequently covered with a specialized barrier membrane. This membrane prevents faster-growing soft tissue cells (fibroblasts) from invading the graft site, allowing the slower-growing bone cells exclusive access to the scaffold. Depending on the clinical scenario, these membranes may be resorbable (dissolving naturally over time) or non-resorbable (requiring removal at a later stage, often reinforced with titanium for structural support).
The timeline for bone grafting for implants varies depending on the extent of the augmentation. For minor defects, the graft and the implant may be placed simultaneously. However, for significant vertical or horizontal deficiencies, a staged approach is necessary. The graft is placed and allowed to heal and consolidate for a period of four to nine months before the implant fixture can be safely inserted. This meticulous approach ensures that the foundation is biologically sound, significantly reducing the risk of complications discussed in our Peri Implantitis Prevention: Clinical Guide.
Clinical Solution 2: Sinus Lifts for Upper Jaw Implants
A sinus lift is a specialized grafting procedure that elevates the Schneiderian membrane and places bone graft material beneath it to increase vertical bone height in the posterior upper jaw.
The rehabilitation of the posterior maxilla (upper back jaw) presents unique anatomical challenges. As previously noted, the combination of alveolar bone resorption and sinus pneumatization often leaves an inadequate vertical height of bone to support standard implants. To overcome this limitation, oral surgeons perform a maxillary sinus floor elevation, commonly referred to as a sinus lift. This procedure creates the necessary vertical dimension by utilizing the space within the lower portion of the sinus cavity[4].

There are two primary surgical approaches to performing a sinus lift, selected based on the amount of residual bone present. The lateral window technique (direct sinus lift) is utilized when there is severe bone deficiency (typically less than 4 millimeters of residual bone height). The surgeon creates a small, precise window in the lateral wall of the maxilla to access the sinus cavity. The delicate Schneiderian membrane lining the sinus is carefully detached and elevated upward. The newly created space beneath the elevated membrane is then densely packed with bone graft material (often a slow-resorbing xenograft to maintain long-term volume). The lateral window is covered with a barrier membrane, and the surgical site is sutured closed. Healing typically requires six to nine months before implants can be placed.
Conversely, the crestal approach (indirect sinus lift) is a less invasive technique employed when there is a moderate amount of residual bone (typically 5 to 8 millimeters). In this method, the surgeon accesses the sinus floor through the same osteotomy (drilled hole) created for the implant placement. Using specialized instruments or hydraulic pressure, the sinus floor is gently fractured and elevated, and graft material is pushed upward through the osteotomy. Because this technique relies on the initial stability provided by the residual bone, the implant is often placed simultaneously during the same surgical visit.
Achieving adequate sinus lift bone volume is critical for the long-term success of posterior maxillary implants. The procedure requires a high degree of surgical precision to avoid perforating the sinus membrane, which can compromise the graft and lead to infection. Advanced 3D imaging is indispensable for mapping the sinus anatomy, identifying septa (bony partitions within the sinus), and measuring the exact thickness of the membrane prior to surgery. When executed correctly, sinus lifts boast a remarkably high success rate, providing a robust foundation for single crowns or Multiple Dental Implants in the upper jaw.
Clinical Solution 3: Zygomatic Implants for Severe Upper Jaw Loss
Zygomatic implants bypass the severely resorbed upper jawbone entirely by anchoring extra-long titanium posts directly into the dense, stable bone of the zygomatic arch (cheekbone).
For patients presenting with extreme maxillary atrophy—where traditional bone grafting or sinus lifts are either unfeasible, have previously failed, or would require an unacceptably long and complex treatment timeline—zygomatic implants offer a revolutionary graftless alternative. Developed specifically to address severe bone loss in the upper jaw, these specialized implants are significantly longer than conventional fixtures, ranging from 30 to 60 millimeters in length. Instead of relying on the compromised alveolar ridge, zygomatic implants are anchored into the body of the zygoma (the cheekbone)[5].
The zygomatic bone is exceptionally dense and cortical in nature, providing superior primary stability compared to the softer, trabecular bone typically found in the maxilla. This high degree of initial stability is a critical advantage, as it frequently allows for immediate loading protocols. In many cases, patients can have the zygomatic implants placed and a fixed, functional provisional prosthesis attached on the exact same day, drastically reducing the overall treatment time and psychological burden associated with prolonged edentulism.
Clinical Case Example: A 62-year-old patient visited HCMC Dental Clinic in Ho Chi Minh City after being told by multiple providers that she was not a candidate for implants due to severe maxillary resorption from decades of denture wear. Utilizing 3D computer-guided surgery, the clinical team successfully placed bilateral zygomatic implants combined with two anterior conventional implants. The patient received a fixed provisional bridge on the same day, bypassing the need for extensive sinus grafting and a 12-month healing period.
The surgical placement of zygomatic dental implants is highly complex and requires specialized training and expertise in maxillofacial surgery. The trajectory of the implant must be meticulously planned to navigate safely past the maxillary sinus, the orbital floor (eye socket), and critical neurovascular structures. Depending on the anatomical presentation, the implant body may pass entirely within the sinus cavity (intrasinus approach) or run along the exterior wall of the maxilla (extrasinus approach). In cases of absolute maxillary deficiency, a “Quad Zygoma” protocol may be employed, utilizing four zygomatic implants to support a full-arch prosthesis without any conventional implants.
While the procedure is more invasive than standard implant placement, the functional and aesthetic outcomes are profound. Zygomatic implants eliminate the morbidity associated with harvesting large block grafts from the hip or skull, and they offer a predictable solution for patients who previously had no viable options for fixed dental rehabilitation. For international patients seeking advanced restorative care, understanding the Dental Implant Cost associated with these specialized procedures is an important part of the comprehensive treatment planning process.
Am I a Candidate for Implants with Bone Loss?
Candidacy is determined through comprehensive 3D CBCT imaging and clinical evaluation to assess remaining bone architecture, systemic health, and the most appropriate regenerative or graftless surgical pathway.
Determining whether a patient is a suitable candidate for dental implants with severe bone loss requires a rigorous diagnostic protocol. The cornerstone of this evaluation is Cone Beam Computed Tomography (CBCT). Unlike traditional two-dimensional dental X-rays, a CBCT scan provides a highly detailed, three-dimensional reconstruction of the maxillofacial skeleton. This allows the implantologist to precisely measure the height, width, and density (measured in Hounsfield units) of the available bone, map the exact location of nerves and sinuses, and virtually simulate the surgical placement of the implants before any physical intervention occurs.
“The advent of 3D CBCT imaging has fundamentally transformed implantology. We no longer guess the topography of the bone; we navigate it with sub-millimeter precision, allowing us to safely treat patients who were previously deemed inoperable.”
Beyond anatomical considerations, systemic health plays a pivotal role in determining candidacy. Conditions that impair healing or compromise the immune system must be carefully evaluated. Uncontrolled diabetes, for instance, significantly impairs microcirculation and increases the risk of post-operative infection and implant failure. However, patients with well-managed diabetes are generally excellent candidates. Similarly, patients undergoing active treatment with intravenous bisphosphonates (often prescribed for osteoporosis or certain cancers) may be at risk for medication-related osteonecrosis of the jaw (MRONJ) and require specialized medical clearance.

Smoking is another critical factor. The toxins in tobacco smoke constrict blood vessels, reducing the oxygen supply to the surgical site and severely impeding the integration of bone grafts and implants. While smoking is not an absolute contraindication, patients are strongly advised to adhere to a strict cessation protocol before and after surgery to optimize clinical outcomes. Dr. Cuong emphasizes that a thorough review of medical history and a collaborative approach with the patient’s primary physician are essential components of the Implant Consultation process.
Ultimately, the vast majority of patients with bone loss can be successfully treated. The question is rarely “Can I get implants?” but rather “Which specific clinical pathway is required to ensure my implants are safe, functional, and long-lasting?” Whether through localized grafting, sinus elevation, or advanced zygomatic techniques, modern dentistry offers a tailored solution for nearly every anatomical challenge.
When to Consult a Clinical Implantologist
Patients experiencing loose dentures, facial collapse, or difficulty chewing should consult a specialized implantologist promptly to evaluate bone volume and prevent further irreversible structural degradation.
If you have been missing teeth for an extended period or have worn removable dentures for years, it is highly probable that some degree of bone resorption has occurred. Early clinical intervention is paramount. The longer the alveolar ridge remains unstimulated, the more complex and extensive the required regenerative procedures become. You should seek a comprehensive evaluation if you notice your dentures becoming increasingly loose or requiring frequent relines, as this is a primary indicator of changing bone topography beneath the gums.
Additionally, signs of facial collapse—such as a deepening of the nasolabial folds, a protruding lower jaw, or a “caved-in” appearance around the mouth—suggest significant loss of vertical bone height. Patients who have been previously diagnosed with advanced periodontal disease should also seek specialized consultation, as the infection may have severely compromised the bony housing. To explore your specific options and understand how underlying conditions are managed, reviewing resources like Implants and Gum Disease: Clinical Protocols & Success can provide valuable insight before your clinical appointment.
Frequently Asked Questions
Can dental implants reverse jawbone loss?
Dental implants cannot reverse existing bone loss, but they do halt further deterioration. By acting as artificial tooth roots, implants provide the necessary mechanical stimulation to the surrounding alveolar bone, preserving its current volume and density over time. To regain lost bone, regenerative procedures like bone grafting must be performed prior to or in conjunction with implant placement.
How long after bone grafting can I get implants?
The healing period after bone grafting typically ranges from three to six months. This timeframe allows the graft material to fully integrate and regenerate solid natural bone, ensuring a stable foundation before the titanium implant fixture is surgically placed. In cases of minor defects, the graft and implant may occasionally be placed during the same surgical visit.
Are zygomatic implants safe for patients with severe bone loss?
Yes, zygomatic implants are a safe and highly effective clinical solution for severe upper jawbone loss. Because they anchor into the dense cheekbone rather than the deficient maxillary bone, they offer excellent primary stability without the need for extensive grafting. However, the procedure requires a highly skilled maxillofacial surgeon due to the complex anatomical structures involved.
Does bone grafting for dental implants hurt?
Bone grafting is performed under local anesthesia or intravenous sedation, ensuring the procedure itself is virtually painless. Post-operative discomfort is typically mild to moderate and can be effectively managed with prescribed analgesics and cold compresses during the initial healing phase. Most patients report that the recovery is much easier than anticipated.
Can I get All-on-4 implants if I have bone loss?
Yes, the All-on-4 concept is specifically designed to maximize the use of available bone. By tilting the posterior implants at a 45-degree angle, oral surgeons can often bypass areas of severe bone loss, avoiding the need for complex grafting procedures. This technique utilizes the denser anterior bone to support a full-arch fixed prosthesis.
References
- Journal of Clinical Periodontology. Alveolar bone remodeling following tooth extraction and ridge preservation. (2020).
- International Journal of Oral & Maxillofacial Implants. Primary stability and osseointegration in compromised bone. (2021).
- Clinical Implant Dentistry and Related Research. Efficacy of guided bone regeneration using various graft materials. (2019).
- Journal of Oral and Maxillofacial Surgery. Maxillary sinus floor elevation techniques and survival rates. (2022).
- International Journal of Prosthodontics. Long-term clinical outcomes of zygomatic implants in severely resorbed maxillae. (2018).