

White stains after braces, clinically known as white spot lesions (WSLs), are early signs of enamel demineralization. They occur when plaque and bacterial acids accumulate around orthodontic brackets, stripping essential minerals from the teeth. Prompt clinical intervention can halt and reverse this damage, restoring your natural smile.
Clinical Summary:
White spot lesions are a prevalent complication of fixed orthodontic therapy, resulting from prolonged plaque retention and localized enamel demineralization. Clinicians classify these opacities as early non-cavitated carious lesions. Treatment ranges from conservative remineralization using topical fluorides and casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) to minimally invasive resin infiltration (Icon) and microabrasion. Preventive strategies, including rigorous oral hygiene and considering removable aligners, significantly mitigate the risk of developing these permanent aesthetic defects. Comprehensive diagnostic evaluation is essential to differentiate these lesions from other enamel hypoplasias and to formulate an effective, individualized restorative protocol.
Key Takeaways:
- White stains are early-stage cavities caused by acid-producing bacteria trapped around orthodontic hardware.
- Enamel demineralization alters light reflection, creating a distinct, chalky white appearance on the tooth surface.
- Resin infiltration is a highly effective, drill-free clinical treatment designed to blend the spots with natural enamel.
- Topical fluoride and specialized remineralizing pastes can help reverse mild, superficial lesions over time.
- Strict oral hygiene, dietary control, and regular professional cleanings are essential during orthodontic treatment.
The Pathophysiology of White Spot Lesions (WSLs)
White spot lesions develop when acidogenic bacteria in dental plaque ferment dietary carbohydrates, producing organic acids that dissolve the calcium and phosphate minerals within the enamel matrix.
Understanding the formation of white stains after braces requires a deep dive into the biochemical interactions that occur at the tooth surface. The oral cavity is a dynamic environment where cycles of demineralization and remineralization occur continuously. Under normal circumstances, saliva acts as a natural buffer, neutralizing dietary acids and supplying calcium and phosphate ions to repair microscopic enamel damage. However, the introduction of fixed orthodontic appliances fundamentally alters this delicate balance.
Orthodontic brackets, archwires, and elastomeric ligatures create numerous retention sites that are highly challenging to clean with standard brushing techniques. These irregular surfaces facilitate the rapid accumulation and maturation of cariogenic biofilms, predominantly composed of Streptococcus mutans and Lactobacilli species. When a patient consumes fermentable carbohydrates, these bacteria metabolize the sugars and excrete lactic acid as a byproduct. This localized acid production causes the plaque fluid pH to drop rapidly below the critical threshold of 5.5, initiating the dissolution of hydroxyapatite crystals within the enamel[1].

The structural architecture of a white spot lesion is clinically fascinating. Unlike a traditional cavity that forms a physical hole, a WSL is characterized by an intact, albeit highly porous, surface layer overlying a severely demineralized subsurface body. The loss of minerals increases the porosity of the enamel, altering its refractive index. Healthy enamel is translucent, allowing light to pass through and reflect off the underlying dentin. In contrast, the porous subsurface of a WSL scatters light irregularly, resulting in the characteristic opaque, chalky white appearance.
“The presence of fixed orthodontic appliances creates multiple retention sites for cariogenic biofilms, shifting the oral microbiome towards acid-producing strains and accelerating localized enamel dissolution at an unprecedented rate.”
According to Dr. Nguyen Van Cuong, a leading specialist at HCMC Dental Clinic, the onset of these lesions can be remarkably rapid. Clinical observations indicate that visible decalcification can occur within just four weeks of bracket placement if oral hygiene is severely neglected. This underscores the critical importance of proactive preventive measures and continuous monitoring throughout the duration of Orthodontics.
Clinical Diagnosis: Differentiating White Stains
Accurate diagnosis requires distinguishing orthodontic white spot lesions from other enamel defects like dental fluorosis, molar incisor hypomineralization, or genetic enamel hypoplasia through careful visual and tactile examination.
Not all white spots on teeth are caused by orthodontic treatment. A precise differential diagnosis is paramount for determining the appropriate therapeutic intervention. Clinicians utilize a combination of visual inspection, tactile assessment, and patient history to accurately identify the etiology of the enamel opacities.
Orthodontic white spot lesions typically present in specific patterns. They are most commonly located on the cervical third of the tooth (near the gumline) or outlining the exact perimeter of where the orthodontic bracket was bonded. The lesions often appear dull, chalky, and rough when gently probed with a dental explorer. In contrast, developmental defects like dental fluorosis usually present as diffuse, bilateral, and symmetrical opacities that are present from the moment the tooth erupts.
To aid in diagnosis, clinicians often employ the International Caries Detection and Assessment System (ICDAS). Under this system, early white spot lesions are classified as Code 1 (first visual change in enamel visible only after prolonged air drying) or Code 2 (distinct visual change in enamel visible when wet). Advanced diagnostic tools, such as quantitative light-induced fluorescence (QLF) and optical coherence tomography (OCT), can also be utilized to measure the depth and severity of the demineralization objectively[2].
| Condition | Etiology (Cause) | Clinical Appearance | Location Pattern |
|---|---|---|---|
| Orthodontic WSLs | Plaque accumulation and acid demineralization | Chalky, opaque, rough surface, distinct borders | Cervical third, outlining bracket footprint |
| Dental Fluorosis | Excess fluoride ingestion during tooth development | Diffuse, cloudy, sometimes with brown mottling | Symmetrical, affecting multiple teeth globally |
| Enamel Hypoplasia | Genetic or systemic disruption during enamel matrix formation | Pits, grooves, or generalized thin enamel | Variable, often horizontal bands across teeth |
| Molar Incisor Hypomineralization (MIH) | Idiopathic disruption during early childhood | Creamy, yellow, or brown demarcated opacities | Specifically affects first molars and incisors |
Establishing the correct diagnosis dictates the treatment pathway. While post-orthodontic decalcification responds well to remineralization and infiltration techniques, developmental defects may require entirely different restorative approaches, such as composite bonding or porcelain veneers.
Professional Treatment Workflows for Enamel Remineralization
Modern dentistry offers a spectrum of treatments for white stains, ranging from non-invasive remineralizing agents to advanced resin infiltration and microabrasion techniques designed to restore enamel aesthetics.
The management of white stains after braces follows a minimally invasive philosophy. The primary goal is to arrest the demineralization process, promote the uptake of lost minerals, and restore the optical properties of the tooth without unnecessarily removing healthy tooth structure. The choice of treatment depends heavily on the depth, age, and severity of the lesion.
Topical Fluoride and CPP-ACP Therapy
For mild, early-stage lesions, conservative remineralization is the first line of defense. High-concentration topical fluoride varnishes (typically 5% sodium fluoride) are applied professionally to the affected areas. Fluoride works by replacing the hydroxyl ions in the enamel matrix, forming fluorapatite—a crystal structure that is significantly more resistant to future acid attacks than natural hydroxyapatite[3].
In addition to fluoride, Casein Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP), commonly known as MI Paste, is frequently prescribed. This bioactive material delivers a high concentration of bioavailable calcium and phosphate directly to the porous enamel surface. By maintaining a state of supersaturation at the tooth surface, CPP-ACP facilitates deep subsurface remineralization, gradually reducing the chalky appearance of the lesion over several months of consistent application.
Resin Infiltration (Icon Treatment)
When remineralization therapies are insufficient to resolve the aesthetic defect, resin infiltration (often referred to by the brand name Icon) is considered the gold standard for treating post-orthodontic white spots. This innovative, micro-invasive technique bridges the gap between prevention and traditional restorative dentistry.
The principle behind resin infiltration is optical blending. The porous subsurface of the white spot lesion contains trapped air and water, which have a lower refractive index than healthy enamel, causing the opaque appearance. The infiltration process replaces this trapped air with a low-viscosity light-curing resin that has a refractive index nearly identical to natural enamel, effectively masking the lesion.
The clinical workflow for resin infiltration is highly precise:
- Surface Preparation: The pseudo-intact surface layer of the lesion is eroded using a 15% hydrochloric acid (HCl) gel for approximately two minutes. This opens the pore system of the demineralized enamel.
- Desiccation: The lesion is thoroughly rinsed and dried. An ethanol-based drying agent is applied to completely evaporate any residual moisture within the microporosities. At this stage, the lesion often appears temporarily more pronounced.
- Infiltration: A highly fluid, low-viscosity TEGDMA-based resin is applied to the surface and allowed to penetrate deep into the capillary system of the lesion for several minutes.
- Polymerization: Excess material is removed, and the resin is light-cured, locking it into the enamel matrix. The application and curing steps are often repeated to ensure complete saturation.
Clinical Case Study: HCMC Dental Clinic
A 19-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City immediately following the removal of traditional metal braces. The patient exhibited severe, highly visible white spot lesions across the maxillary anterior teeth, causing significant aesthetic distress. Dr. Cuong evaluated the lesions and determined they were non-cavitated but too deep for topical remineralization alone. A single-visit resin infiltration protocol was executed. Post-operatively, the chalky opacities were virtually eliminated, blending seamlessly with the surrounding healthy enamel, restoring the patient’s confidence without the need for any drilling or anesthesia.
Enamel Microabrasion
For superficial lesions that are resistant to remineralization but do not warrant infiltration, enamel microabrasion is a viable alternative. This technique involves the simultaneous application of a mild acid (typically 18% hydrochloric acid) and an abrasive pumice slurry. The clinician uses a slow-speed rubber cup to gently polish away the outermost microscopic layer of defective enamel (usually less than 0.1mm)[4].
Microabrasion leaves behind a dense, highly polished enamel surface that is often more resistant to future decay. While effective for shallow stains, it is contraindicated for deep lesions, as excessive enamel removal can lead to dentin exposure and subsequent tooth sensitivity.
Composite Bonding and Veneers
In severe cases where the demineralization has progressed to structural cavitation (actual holes in the teeth), minimally invasive techniques are no longer sufficient. These advanced lesions require traditional restorative approaches. The decayed tissue must be carefully excavated, and the tooth restored using highly aesthetic composite resin bonding. For patients with extensive, generalized damage across multiple teeth, porcelain veneers may be recommended to provide a durable, long-lasting aesthetic rehabilitation.
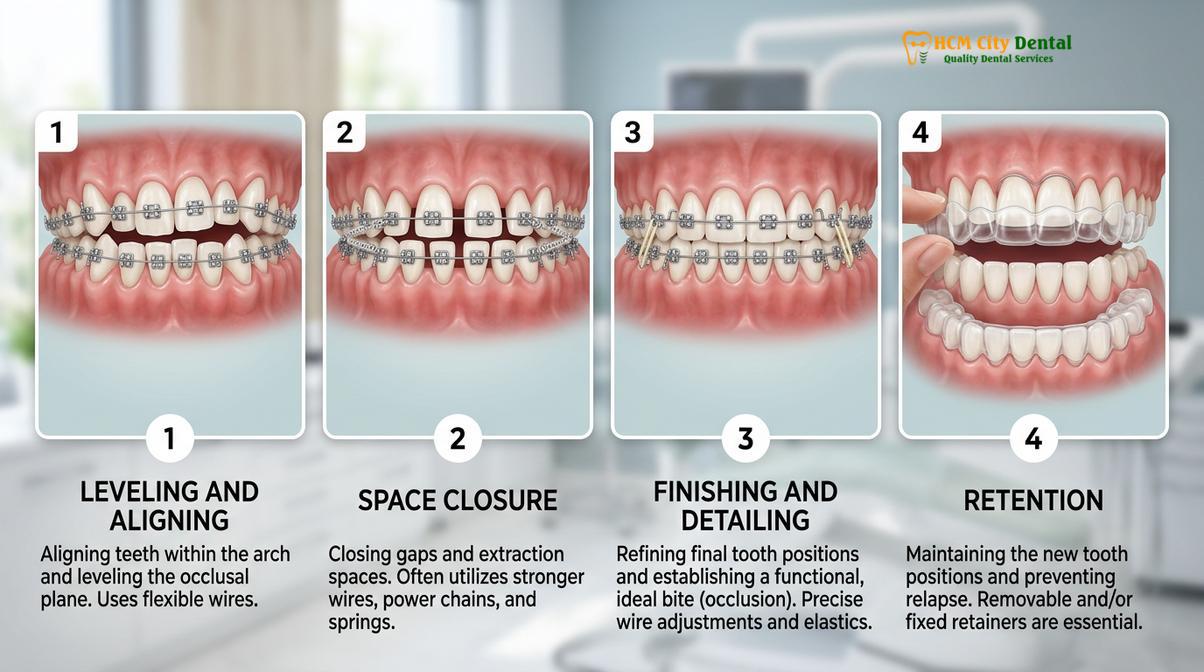
Prevention Strategies During Orthodontic Treatment
Preventing white stains requires meticulous oral hygiene, dietary modifications, and sometimes choosing removable orthodontic appliances that facilitate easier cleaning and reduce plaque retention.
The most effective treatment for white spot lesions is preventing their occurrence entirely. Orthodontic patients must adopt a rigorous, multi-faceted approach to oral hygiene to protect their enamel during the alignment process. The presence of brackets and wires demands specialized tools and techniques.
Patients are instructed to brush after every meal using a soft-bristled orthodontic toothbrush or an electric toothbrush with a specialized ortho head. Interdental cleaning is non-negotiable; traditional flossing is often supplemented or replaced by water flossers and interproximal brushes, which are highly effective at dislodging plaque from beneath the archwires and around the bracket bases.

Dietary counseling is equally critical. Patients must minimize their intake of fermentable carbohydrates, particularly sticky sweets and acidic beverages like sodas and sports drinks. Frequent snacking should be avoided to allow the saliva sufficient time to buffer the oral pH and facilitate natural remineralization.
Clinical Warning: Avoid using highly abrasive whitening toothpastes or over-the-counter bleaching strips while wearing braces or immediately after their removal if white spots are present. These products can aggressively abrade the already weakened, porous enamel and may cause the surrounding healthy tooth structure to lighten, making the white stains appear even more prominent.
For patients with a high caries risk or those who struggle with manual dexterity, clinicians may recommend alternative orthodontic systems. Utilizing self-ligating bracket systems can slightly reduce plaque retention compared to traditional elastomeric ties. However, the most significant preventive advantage is found in removable clear aligner therapy.
Choosing clear aligner therapy allows patients to remove their orthodontic appliances completely during meals and oral hygiene routines. This eliminates the physical barriers to effective brushing and flossing, drastically reducing the incidence of white spot lesions. For adults seeking affordable adult braces or those focused on treating severe dental crowding without compromising enamel aesthetics, aligners present a compelling clinical advantage.
“Proactive prevention through rigorous home care, dietary discipline, and regular professional fluoride applications remains the absolute gold standard in avoiding permanent post-orthodontic enamel scarring.”
Regular professional monitoring is essential. Orthodontists and dental hygienists should evaluate the patient’s oral hygiene at every adjustment appointment. If early signs of demineralization are detected, immediate interventions, such as prescribing high-concentration fluoride toothpaste (5000 ppm) or applying professional fluoride varnishes, can arrest the progression before the damage becomes irreversible.
Important Clinical Considerations (When to See a Doctor)
While many patients experience mild, transient decalcification that improves slightly with natural salivary remineralization, certain clinical signs warrant immediate professional evaluation. You should schedule a consultation with a qualified dental professional if you observe any of the following symptoms following the removal of your orthodontic appliances:
- Surface Cavitation: If the white spots feel rough, pitted, or if you can feel a distinct physical indentation with your tongue or fingernail, the lesion has progressed beyond simple demineralization and requires restorative treatment.
- Color Changes: White spots that begin to turn yellow, brown, or black indicate that the porous enamel is absorbing dietary stains or that active carious decay is progressing deeper into the dentin layer.
- Thermal Sensitivity: Experiencing sharp pain or lingering discomfort when consuming hot, cold, or sweet foods and beverages suggests that the enamel layer has been significantly compromised, exposing the sensitive underlying dentin.
- Lack of Improvement: If the chalky white appearance persists for more than six months post-debonding despite rigorous home care and the use of fluoridated products, professional intervention like resin infiltration is likely necessary to resolve the aesthetic defect[5].

At HCMC Dental Clinic, our specialists, including Dr. Cuong, emphasize the importance of a comprehensive post-orthodontic evaluation. Whether you have just completed treatment for correcting horizontal overjet or are exploring orthodontic options, ensuring the long-term health and aesthetics of your enamel is our primary clinical objective. We encourage patients in Ho Chi Minh City to seek timely assessments to explore the most conservative and effective treatment pathways for their specific needs, ensuring their orthodontic transformations are truly flawless.
Frequently Asked Questions
Do white spots from braces go away on their own?
White spots rarely disappear completely on their own without clinical intervention. While natural saliva provides some remineralization, the highly porous enamel usually requires professional treatments like fluoride varnish, CPP-ACP pastes, or resin infiltration to fully restore its structural integrity and aesthetic appearance. Relying solely on natural healing often leaves a permanent, albeit slightly faded, chalky scar on the tooth surface.
Can I use whitening strips to fix white stains after braces?
No, using over-the-counter whitening strips is not recommended for treating white spot lesions. Bleaching agents lighten the surrounding healthy enamel, which can actually make the opaque white stains appear more prominent and exacerbate underlying enamel sensitivity. Professional remineralization or infiltration focuses on restoring the optical properties of the damaged area specifically, rather than bleaching the entire tooth.
How long does resin infiltration treatment take?
Resin infiltration is typically completed in a single dental visit lasting approximately 45 to 60 minutes. The procedure is minimally invasive, requires no drilling or local anesthesia, and provides immediate aesthetic improvements by altering the light-reflecting properties of the damaged enamel. Multiple teeth can usually be treated simultaneously during this single appointment.
Are white spot lesions actually cavities?
White spot lesions are classified as early, non-cavitated carious lesions. They represent the initial stage of tooth decay where minerals have been lost, but the physical surface of the enamel has not yet collapsed to form a structural hole or cavity. If left untreated and exposed to continuous acid attacks, these lesions will eventually progress into full clinical cavities requiring traditional fillings.
Does Invisalign cause white spots on teeth?
Clear aligners pose a significantly lower risk of causing white spots compared to traditional fixed braces. Because the aligners are removable, patients can maintain their normal brushing and flossing routines, drastically reducing the prolonged plaque accumulation that leads to enamel demineralization. However, if a patient consumes sugary drinks while wearing the aligners or fails to brush before reinserting them, decalcification can still occur.
References
- American Journal of Orthodontics and Dentofacial Orthopedics. Incidence and severity of white spot lesions during orthodontic treatment. (2019).
- Journal of Dentistry. The efficacy of resin infiltration on post-orthodontic white spot lesions: A clinical review. (2021).
- Caries Research. Enamel remineralization protocols utilizing CPP-ACP and fluoride varnishes. (2020).
- International Journal of Paediatric Dentistry. Microabrasion techniques for aesthetic management of enamel decalcification. (2018).
- Journal of Clinical Orthodontics. Preventive strategies for enamel demineralization in fixed appliance therapy. (2022).



