A full dental bridge is a fixed prosthetic restoration designed to replace one or more missing teeth by anchoring an artificial tooth (pontic) to adjacent natural teeth or implants (abutments). This clinical solution aims to restore chewing function, prevent adjacent tooth shifting, and rehabilitate the patient’s natural smile architecture.
Clinical Summary:
A full dental bridge serves as a highly effective, non-surgical intervention for treating partial edentulism. By utilizing healthy adjacent teeth as structural pillars, the prosthesis bridges the gap left by missing teeth, restoring both occlusal stability and phonetic function. Modern advancements in dental materials, particularly monolithic zirconia and lithium disilicate, allow these restorations to achieve exceptional fracture toughness while mimicking the optical properties of natural enamel. The clinical workflow requires precise tooth preparation, accurate impression taking, and meticulous cementation protocols to support marginal integrity and long-term periodontal health. While highly durable, the success of a fixed partial denture relies heavily on the structural capacity of the abutment teeth and the patient’s commitment to specialized interdental hygiene.
Key Takeaways:
- A full dental bridge requires the irreversible preparation (reduction) of adjacent healthy teeth to serve as supportive abutments.
- Biomechanical stability is guided by Ante’s Law, which suggests the root surface area of abutments should exceed that of the missing teeth.
- Advanced materials like Y-TZP zirconia offer superior tensile strength, making them highly suitable for posterior load-bearing regions.
- Meticulous marginal fit is critical to help prevent microleakage, secondary caries, and subsequent endodontic complications.
- Unlike dental implants, bridges do not stimulate the underlying alveolar bone, which may lead to gradual localized bone resorption over time.
Clinical Definition and Biomechanics of a Full Dental Bridge
A full dental bridge utilizes adjacent healthy teeth as structural pillars to support a suspended prosthetic tooth, effectively bridging the edentulous gap. This fixed restoration relies on precise biomechanical distribution of occlusal forces to promote long-term stability.
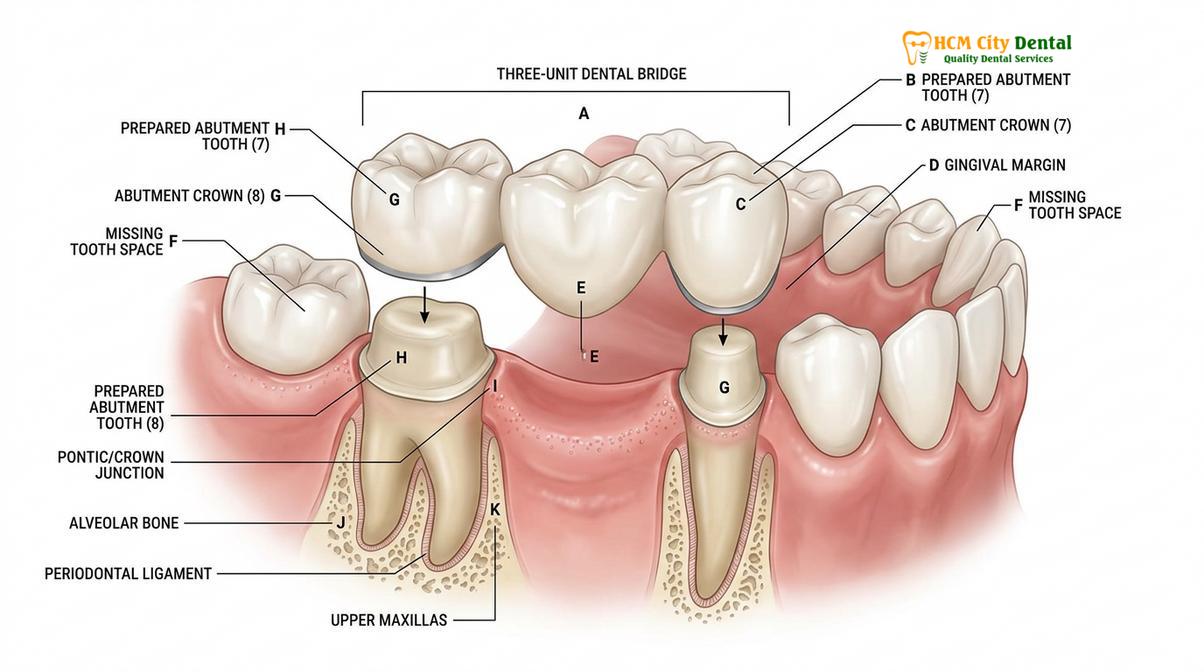
In the realm of fixed prosthodontics, a full dental bridge—technically referred to as a fixed partial denture (FPD)—is a cornerstone treatment for rehabilitating localized tooth loss. The architecture of a standard bridge consists of two primary components: the abutments and the pontic. The abutments are the natural teeth (or dental implants) located on either side of the edentulous space, which are clinically prepared to receive full-coverage crowns. The pontic is the artificial tooth suspended between these retainers, designed to seamlessly replace the missing coronal structure.
The biomechanical success of a full dental bridge is heavily governed by the principles of physics, specifically the behavior of beams under load. When a patient chews, the pontic acts as a suspended beam. According to the laws of structural mechanics, the deflection (bending) of this beam is proportional to the cube of its length. Therefore, a bridge replacing two missing teeth will bend significantly more than a bridge replacing a single tooth under the same occlusal force[1]. This exponential increase in stress highlights the critical need for robust material selection and adequate abutment support, particularly in posterior regions[2].
To support optimal load distribution and reduce the risk of structural failure, clinicians generally adhere to Ante’s Law. This fundamental prosthodontic principle states that the combined pericemental (root surface) area of the abutment teeth should ideally be equal to or greater than the root surface area of the teeth being replaced. If this biomechanical ratio is violated, the excessive occlusal forces can lead to periodontal ligament trauma, abutment mobility, and eventual failure of the entire restoration. Achieving proper dental harmony across the arch requires the clinician to meticulously evaluate the root morphology, crown-to-root ratio, and bone support of the prospective abutment teeth before initiating treatment.
Diagnostic Criteria and Patient Candidacy
Ideal candidates for a full dental bridge possess healthy, structurally sound adjacent teeth and adequate periodontal support to withstand the additional chewing loads. Comprehensive radiographic evaluation is mandatory to rule out active infections before preparation.
Not every instance of tooth loss can be appropriately managed with a full dental bridge. The diagnostic phase is arguably the most critical step in the clinical workflow. During the initial consultation, the prosthodontist conducts a thorough clinical and radiographic examination to assess the viability of the adjacent teeth. The ideal abutment tooth must have a vital pulp or a successfully treated and sealed root canal system, along with sufficient remaining coronal tooth structure to provide adequate retention and resistance form for the overlying crown.
Periodontal health is an absolute prerequisite. The supporting alveolar bone must be stable, and the gingival tissues must be free of active inflammation. Placing a bridge on periodontally compromised teeth can accelerate bone loss due to the increased functional load[3]. Furthermore, patients presenting with severe, untreated halitosis often have underlying periodontal pockets or deep carious lesions that must be fully resolved before any fixed prosthodontic work can commence. The crown-to-root ratio is carefully measured on periapical radiographs; an ideal ratio is 1:2, though a minimum ratio of 1:1 may be acceptable under favorable occlusal conditions.
Dr. Nguyen Van Cuong, a leading restorative specialist, emphasizes that patient compliance is a major factor in determining candidacy for fixed prosthetics. He notes that understanding how to find a good dentist helps ensure patients receive accurate diagnostic assessments before irreversible tooth preparation begins. According to Dr. Cuong, the long-term prognosis of a fixed bridge is inextricably linked to the patient’s ability to maintain meticulous plaque control beneath the pontic, as abutment margins are highly susceptible to recurrent decay without proper interdental hygiene.
Step-by-Step Clinical Workflow for Bridge Fabrication
The clinical workflow involves abutment tooth preparation, highly accurate digital or elastomeric impressions, temporary bridge placement, and the final cementation of the permanent prosthesis. This multi-step process typically requires two to three clinical visits.
The fabrication and placement of a full dental bridge is a highly precise procedure that demands meticulous attention to detail at every stage. The process begins with the administration of profound local anesthesia to support patient comfort. The clinician then proceeds with tooth preparation, which involves the circumferential reduction of the enamel and dentin on the abutment teeth. This reduction creates the necessary three-dimensional space for the restorative material. The preparation must feature a specific degree of taper (typically 6 to 10 degrees of convergence) to allow the bridge to seat fully while providing maximum frictional retention.
Creating a precise finish line (the margin where the crown meets the natural tooth) is paramount. Depending on the chosen material, the clinician may utilize a chamfer or a shoulder margin design. To capture this margin accurately, gingival retraction cords are carefully packed into the sulcus to displace the tissue laterally and control moisture. Following retraction, an impression is taken. While traditional polyvinyl siloxane (PVS) materials are still widely used, many modern facilities utilize advanced intraoral 3D scanners. These digital impressions eliminate the discomfort of traditional putty and provide the dental laboratory with a highly accurate, distortion-free virtual model of the patient’s arch.

Once the impression is secured, a provisional (temporary) bridge is fabricated chairside using bis-acrylic composite resin. This temporary restoration is cemented with a non-eugenol temporary cement. The provisional bridge serves multiple critical functions: it protects the exposed dentinal tubules from thermal and chemical stimuli, prevents the abutment teeth from shifting, and helps contour the healing gingival tissues around the pontic site to create a natural emergence profile.
“The provisional restoration is not merely a placeholder; it acts as the architectural blueprint for the final prosthesis. It allows clinicians to evaluate phonetics, occlusal function, and gingival response before the definitive bridge is milled and finalized.”
During the final insertion appointment, the provisional bridge is carefully removed, and the abutment teeth are thoroughly cleaned and isolated. The permanent bridge is then tried in to verify marginal adaptation, interproximal contacts, and occlusal harmony. Once the fit and aesthetics are confirmed, the internal surfaces of the retainers are treated (e.g., sandblasted or etched), and the bridge is permanently bonded using a high-strength adhesive resin cement or a conventional luting agent, depending on the substrate material.
Material Selection: Achieving Aesthetic and Functional Excellence
Modern full dental bridges are fabricated from advanced materials like monolithic zirconia, lithium disilicate (E.max), or porcelain-fused-to-metal (PFM). The choice of material depends on the required tensile strength and the aesthetic demands of the restoration site.
The evolution of dental biomaterials has dramatically expanded the options available for fixed partial dentures. The selection of the appropriate material is a complex clinical decision that balances the need for mechanical durability against the desire for lifelike aesthetics. The three primary categories of materials used today are all-ceramic, porcelain-fused-to-metal (PFM), and full metal alloys.
Monolithic Zirconia (Y-TZP): Yttria-stabilized tetragonal zirconia polycrystal is currently a leading standard for posterior bridges. Zirconia is a polycrystalline ceramic that exhibits exceptional fracture toughness and flexural strength, often exceeding 1000 MPa[4]. Its unique ability to undergo “phase transformation toughening”—where the crystal structure expands slightly to help stop the propagation of micro-cracks—makes it incredibly resistant to the heavy occlusal forces of the molar regions. While older generations of zirconia were highly opaque, modern highly translucent zirconia offers excellent aesthetics while maintaining robust strength.
Lithium Disilicate (E.max): For anterior bridges where aesthetic demands are paramount, lithium disilicate glass-ceramic is often the material of choice. It provides unparalleled translucency, allowing light to scatter through the restoration much like natural enamel. This makes it ideal for achieving a seamless harmony dental aesthetic in the smile zone. However, because its flexural strength is lower than that of zirconia, its use is generally restricted to three-unit bridges in the anterior or premolar regions where chewing forces are less severe.
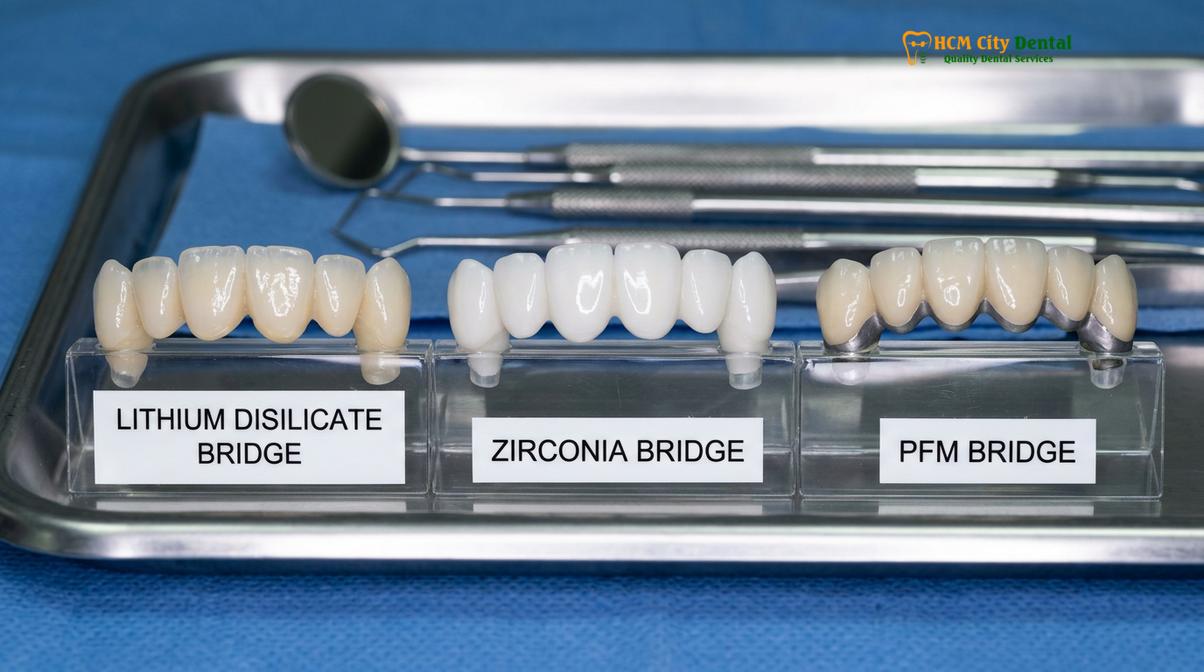
Porcelain-Fused-to-Metal (PFM): For decades, PFM bridges were the standard of care. They consist of a cast metal alloy substructure layered with feldspathic porcelain. While they offer excellent strength and a long track record of clinical success, they have distinct aesthetic limitations. The underlying metal requires an opaque masking layer, which can make the final restoration look somewhat lifeless compared to all-ceramic options. Additionally, if gingival recession occurs over time, the dark metal margin may become visible, compromising the aesthetic outcome.
| Material Type | Primary Indication | Flexural Strength | Aesthetic Quality |
|---|---|---|---|
| Monolithic Zirconia | Posterior Bridges (High Load) | 900 – 1200 MPa | Good to Excellent |
| Lithium Disilicate (E.max) | Anterior Bridges (Smile Zone) | 400 – 500 MPa | Superior / Lifelike |
| Porcelain-Fused-to-Metal | Long-span Bridges | Variable (Metal Core) | Moderate (Opaque) |
| Gold Alloy | Posterior (Heavy Bruxism) | Extremely High | Poor (Metallic) |
Patients seeking the highest level of cosmetic integration often combine bridge work with Porcelain Veneers on adjacent teeth to help ensure a perfectly uniform smile makeover. The laboratory technician must carefully manipulate the ceramic powders to match the exact hue, chroma, and value of the patient’s natural dentition.
Full Dental Bridge vs. Dental Implants: A Clinical Comparison
While a full dental bridge is a rapid, non-surgical method for tooth replacement, dental implants offer independent support without altering adjacent teeth and actively preserve alveolar bone. The optimal choice depends on anatomical, financial, and systemic health factors.
When a patient presents with a missing tooth, the two primary fixed restorative options are a traditional dental bridge and a single dental implant. Understanding the clinical distinctions between these modalities is essential for informed patient consent. A full dental bridge is a tooth-supported prosthesis. Its primary advantage is the speed of treatment; a bridge can typically be completed in a matter of weeks without the need for surgical intervention or prolonged healing periods. It is also highly effective in situations where the adjacent teeth already require full-coverage crowns due to extensive decay or large failing restorations.
However, the biological cost of a bridge is significant. The irreversible removal of healthy enamel and dentin from the abutment teeth increases their lifetime risk of endodontic complications. Furthermore, because the pontic merely rests above the gums, it does not provide mechanical stimulation to the underlying alveolar bone. Over time, this lack of stimulation leads to localized bone resorption (atrophy) in the edentulous ridge, which can create a visible gap beneath the pontic and alter the gingival architecture.
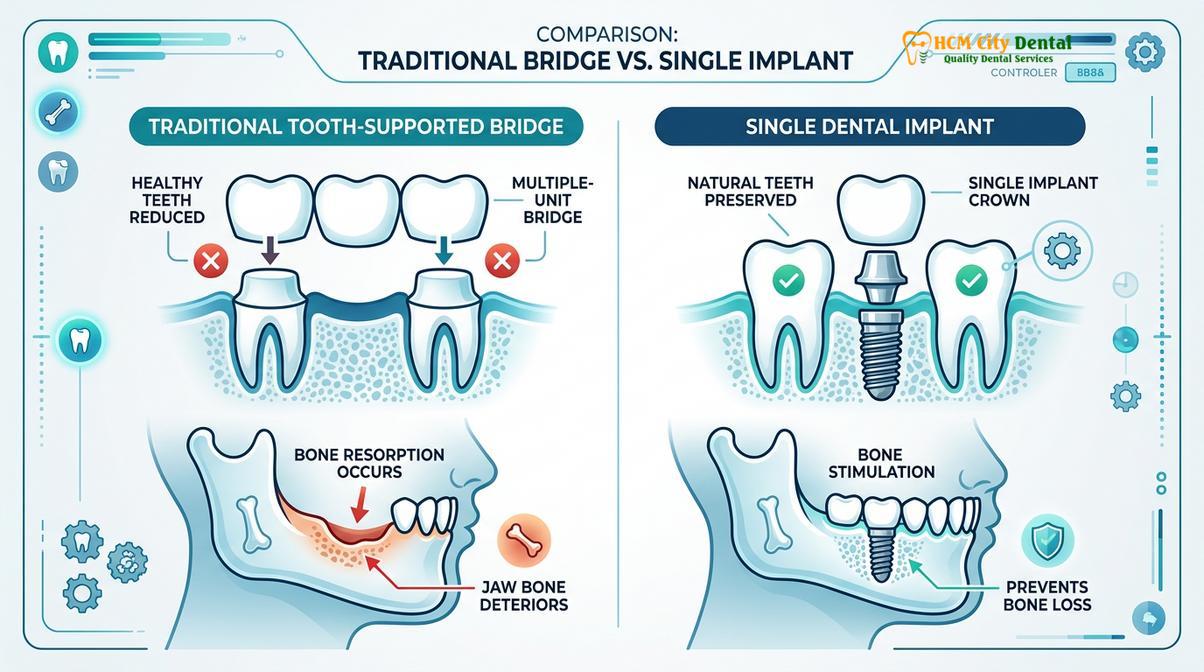
Conversely, a dental implant is a titanium post surgically inserted into the jawbone to act as an artificial tooth root. Implants are independent restorations; they do not require the preparation or alteration of adjacent teeth. Crucially, the integration of the titanium implant with the surrounding bone (osseointegration) helps preserve the bone volume and prevents the collapse of the facial structures. While implants boast a higher initial cost and require a longer treatment timeline (often 3 to 6 months for integration), their long-term survival rates generally compare favorably to those of traditional bridges[5].
Case Study: Restoring Function at HCMC Dental Clinic
Clinical case studies demonstrate the practical application of prosthodontic principles. A well-executed treatment plan can restore both the mechanical function and the aesthetic appearance of a patient’s smile.
A recent clinical case at HCMC Dental Clinic in Ho Chi Minh City involved a 45-year-old patient presenting with a missing mandibular first molar. The adjacent second premolar and second molar both exhibited large, failing amalgam restorations with recurrent decay, making them ideal candidates for full-coverage crowns. After a comprehensive radiographic assessment confirmed adequate bone support and favorable root morphology, a three-unit monolithic zirconia bridge was recommended.
The clinical team at HCMC Dental Clinic utilized an intraoral scanner to capture precise digital impressions following the conservative preparation of the abutment teeth. A highly translucent zirconia block was selected to match the patient’s natural shade. Within two weeks, the final prosthesis was permanently cemented. The patient reported an immediate restoration of chewing efficiency and was highly satisfied with the seamless aesthetic integration of the new bridge.
When to Consult a Prosthodontist: Important Clinical Notes
Recognizing the signs of a failing restoration or underlying dental disease is crucial for timely intervention. Patients should seek professional evaluation if they experience pain, mobility, or structural damage to their dental bridge.
Maintaining a full dental bridge requires ongoing vigilance. According to the Vietnam Ministry of Health (MOH) guidelines on prosthodontic rehabilitation, regular clinical monitoring is essential to detect early signs of marginal leakage or periodontal breakdown[6]. Patients should schedule an evaluation if they notice any of the following symptoms:
- Sensitivity or Pain: Sharp pain when biting down or lingering sensitivity to hot and cold temperatures may indicate recurrent decay under the abutment crowns or pulpal inflammation.
- Mobility: A bridge that feels loose or shifts during mastication is a critical warning sign. This mobility could stem from cement failure, abutment tooth fracture, or severe periodontal bone loss.
- Gingival Inflammation: Persistent redness, swelling, or bleeding around the margins of the bridge often points to inadequate plaque control or an allergic reaction to the restorative materials.
- Visible Damage: Any chipping, cracking, or fracture of the porcelain or zirconia requires immediate assessment to prevent further structural compromise.
“Early detection of marginal discrepancies or occlusal trauma can often save an abutment tooth from extraction. Patients must prioritize their routine dental visits to ensure the longevity of their fixed prostheses.”

Understanding how often you should go to the dentist is a fundamental aspect of protecting your investment in restorative dentistry. Professional cleanings and periodic radiographic examinations allow the clinical team to evaluate the integrity of the cement seal and the health of the supporting bone, ensuring the bridge continues to function optimally for years to come.
References
- Journal of Prosthetic Dentistry. Biomechanical considerations and longevity of fixed partial dentures.
- International Journal of Prosthodontics. Clinical evaluation of monolithic zirconia bridges in posterior regions.
- Journal of Clinical Periodontology. Periodontal response to subgingival crown margins in fixed prosthodontics.
- Dental Materials. Fracture toughness and phase transformation of yttria-stabilized zirconia.
- Journal of the American Dental Association. Comparative outcomes of implant-supported single crowns versus fixed dental prostheses.
- Vietnam Ministry of Health (MOH). National Guidelines on Prosthodontic Rehabilitation and Oral Health Standards.
Are you considering a full dental bridge to restore your smile and chewing function? Contact the specialists at HCMC Dental Clinic in Ho Chi Minh City today to schedule a comprehensive prosthodontic consultation and explore your personalized treatment options.