

The overbite braces process involves comprehensive diagnostics, bracket placement, and the strategic use of archwires and elastics to gradually retract protruding upper teeth and align the jaw. Treatment typically spans several months to a few years, depending on whether the malocclusion is skeletal or purely dental in nature.
Clinical Summary:
Correcting an overbite—clinically classified as a Class II malocclusion or deep bite—requires a meticulously planned orthodontic workflow. The overbite braces process begins with advanced cephalometric and 3D intraoral diagnostics to differentiate between skeletal jaw discrepancies and dental misalignments. Treatment modalities range from traditional metal and ceramic brackets to advanced clear aligner systems. The active phase utilizes biomechanical forces through archwires, intermaxillary elastics, and bite turbos to intrude anterior teeth, extrude posterior teeth, and flatten the curve of Spee. Because adult patients lack active jaw growth, their treatment relies heavily on precise alveolar bone remodeling. Post-treatment retention is critical to prevent relapse, aiming to ensure long-term occlusal stability, improved masticatory function, and enhanced facial aesthetics.
Key Takeaways:
- Diagnostic Precision: Treatment begins with 3D imaging and cephalometric analysis to determine if the overbite is skeletal (jaw-related) or dental (tooth-related).
- Biomechanical Tools: The process frequently utilizes bite turbos, intrusion arches, and Class II elastics to actively shift the bite into a healthy Class I relationship.
- Treatment Duration: Active orthodontic correction generally requires 18 to 36 months, heavily dependent on patient compliance with elastics and aligners.
- Adult Considerations: While highly effective for adults, severe skeletal overbites in non-growing patients may occasionally necessitate adjunctive orthognathic surgery.
- Mandatory Retention: Lifelong retainer wear (fixed or removable) is essential to stabilize the newly remodeled alveolar bone and prevent anterior relapse.
Understanding the Clinical Mechanics of an Overbite
An overbite is a malocclusion where the upper anterior teeth excessively overlap the lower teeth, requiring precise biomechanical intervention to correct both dental alignment and skeletal discrepancies.
In orthodontic terminology, an overbite refers to the vertical overlap of the maxillary (upper) central incisors over the mandibular (lower) central incisors. While a slight overlap of 1 to 2 millimeters is considered a normal, healthy occlusion, an excessive overlap—often referred to as a “deep bite”—can lead to significant functional and structural complications. When discussing the overbite braces process, it is crucial to differentiate between the vertical dimension (overbite) and the horizontal protrusion (overjet), though the two frequently present simultaneously in what is known as a Class II malocclusion [1].
Orthodontists categorize Class II malocclusions into two distinct divisions, each requiring a tailored biomechanical approach:
- Class II, Division 1: Characterized by protruding upper incisors (excessive overjet) combined with a deep overbite. The patient often presents with a narrow maxillary arch and hyperactive lower lip musculature that rests behind the upper incisors, further exacerbating the protrusion.
- Class II, Division 2: Characterized by retroclined (tilted inward) upper central incisors and flared lateral incisors, accompanied by a very deep overbite. In severe cases, the lower incisors may bite directly into the palatal gingiva (roof of the mouth), causing tissue trauma.

The etiology of a deep overbite is multifactorial. Genetics play a primary role in determining jaw size and skeletal relationships. If the mandible (lower jaw) is underdeveloped or positioned too far back relative to the maxilla (upper jaw), a skeletal overbite occurs. Conversely, a dental overbite arises from the abnormal eruption of teeth, such as the over-eruption of anterior teeth or the under-eruption of posterior teeth. Environmental factors, including prolonged childhood habits like thumb-sucking, pacifier use, or chronic mouth breathing, can also alter the development of the alveolar bone and lead to severe malocclusions [2].
Addressing these complex discrepancies requires more than simply straightening the visible crowns of the teeth; it demands a comprehensive strategy to remodel the underlying bone, adjust the occlusal plane, and establish a harmonious relationship between the temporomandibular joints (TMJ) and the dentition.
The Step-by-Step Overbite Braces Process
The orthodontic workflow progresses through comprehensive diagnostics, appliance bonding, active bite correction using targeted forces, and final detailing to establish a stable, functional occlusion.
The journey to correcting a deep bite is a highly structured medical procedure. The overbite braces process is generally divided into four distinct clinical phases, each designed to achieve specific biomechanical objectives.
Phase 1: Comprehensive Diagnostics and Treatment Planning
Before any appliances are placed, a rigorous diagnostic phase is mandatory. At HCMC Dental Clinic in Ho Chi Minh City, our clinical protocols dictate that every patient undergoes a thorough evaluation to map out the exact vectors of tooth movement required. This phase includes:
- Panoramic Radiographs (OPG): To assess overall bone health, root positioning, and the presence of impacted teeth that might interfere with treatment.
- Lateral Cephalometric X-rays: A critical tool for overbite correction. This imaging allows the orthodontist to measure the exact angles of the jawbones and teeth relative to the cranial base.
- Intraoral 3D Scanning: Digital impressions replace traditional messy molds, providing a highly accurate 3D model of the dentition.
- Photographic Analysis: Extraoral and intraoral photographs are taken to evaluate facial symmetry, lip competence, and the patient’s profile.
Phase 2: Appliance Placement and Initial Leveling
Once the treatment plan is finalized, the active overbite braces process begins with the placement of the orthodontic hardware. The teeth are thoroughly cleaned, etched, and dried. The orthodontist then uses a specialized dental adhesive to bond the brackets to the exact center of each tooth’s clinical crown. The precision of bracket placement is paramount, as the bracket slot contains the built-in angles that will dictate the final position of the tooth.
During the first few months, the primary goal is leveling and aligning. Highly flexible Nickel-Titanium (NiTi) archwires are engaged into the brackets. These wires possess shape-memory properties; as they attempt to return to their original U-shape, they apply continuous, gentle forces to untwist rotated teeth and level the dental arches. While this phase improves the appearance of the teeth, it does not yet correct the deep bite.

Phase 3: Active Bite Correction Mechanics
This is the most critical and time-consuming phase of the overbite braces process. Once the teeth are aligned on heavier, rigid stainless steel archwires, the orthodontist begins the complex work of altering the bite relationship. Correcting a deep overbite typically involves flattening the curve of Spee (the natural upward curve of the lower teeth from back to front). This is achieved through anterior intrusion and posterior extrusion.
To facilitate these movements, several auxiliary devices are frequently employed:
- Bite Turbos (Bite Blocks): Small ramps made of composite resin or metal, temporarily bonded to the lingual side of the upper front teeth or the occlusal surface of the back molars. They prevent the patient from biting down fully, protecting the lower brackets from being sheared off by the upper teeth and allowing the posterior teeth room to extrude [3].
- Intermaxillary Elastics (Rubber Bands): Patients are instructed to wear specific elastics connecting the upper and lower braces. For a Class II overbite, elastics typically run from the upper canines to the lower molars.
- Forsus Springs or Herbst Appliances: In severe cases, especially in growing adolescents, fixed functional appliances may be attached to the braces to apply constant pressure to advance the mandible.
Phase 4: Finishing, Detailing, and Retention
As the bite settles into a healthy Class I relationship, the orthodontist makes minor adjustments to the archwires to ensure the roots are perfectly parallel and the marginal ridges of the teeth align seamlessly. Once the functional and aesthetic goals are met, the braces are removed. However, the overbite braces process does not end here. The retention phase is immediately initiated to prevent the periodontal ligaments from pulling the teeth back to their original positions, ensuring long-term occlusal stability [5].
Orthodontic Modalities for Overbite Correction
Orthodontists utilize various appliances, including traditional metal brackets, aesthetic ceramics, self-ligating systems, and clear aligners, tailored to the severity of the patient’s malocclusion.
Advancements in dental technology have expanded the tools available for correcting deep bites. The choice of appliance depends on the clinical complexity of the case, the patient’s aesthetic preferences, and their lifestyle.
Traditional Metal Braces
Constructed from high-grade stainless steel, traditional metal braces remain the gold standard for treating severe, complex overbites. They offer the orthodontist maximum biomechanical control over root angulation and torque. Metal braces are highly durable and can easily accommodate heavy forces from elastics, springs, and headgear if necessary. For patients seeking cost-effective orthodontic solutions, metal brackets often provide the most predictable and efficient pathway to a corrected bite.
Ceramic (Clear) Braces
Ceramic braces function identically to metal braces but utilize brackets made of translucent or tooth-colored polycrystalline alumina. They are significantly less conspicuous, making them a popular choice for adults and self-conscious teens. While highly effective for overbite correction, ceramic brackets are slightly more brittle than metal and can cause wear on opposing enamel if the upper teeth bite directly onto lower ceramic brackets.
Self-Ligating Braces
Instead of using elastic ties to hold the archwire in place, self-ligating systems utilize a specialized sliding door mechanism built into the bracket. This design reduces friction between the wire and the bracket, potentially allowing for more efficient tooth movement and easier oral hygiene. Self-ligating braces are highly effective at expanding narrow dental arches.
Clear Aligner Therapy
Clear aligners have revolutionized the overbite braces process. Using a series of custom-fabricated, BPA-free plastic trays, aligners gradually shift the teeth. For overbite correction, aligners are engineered with precision cuts to accommodate Class II elastics, and bite ramps are built directly into the lingual surface of the upper aligners to help intrude the lower incisors. While aligners offer superior aesthetics, their success is entirely dependent on the patient wearing them for the mandatory 20-22 hours per day [6].
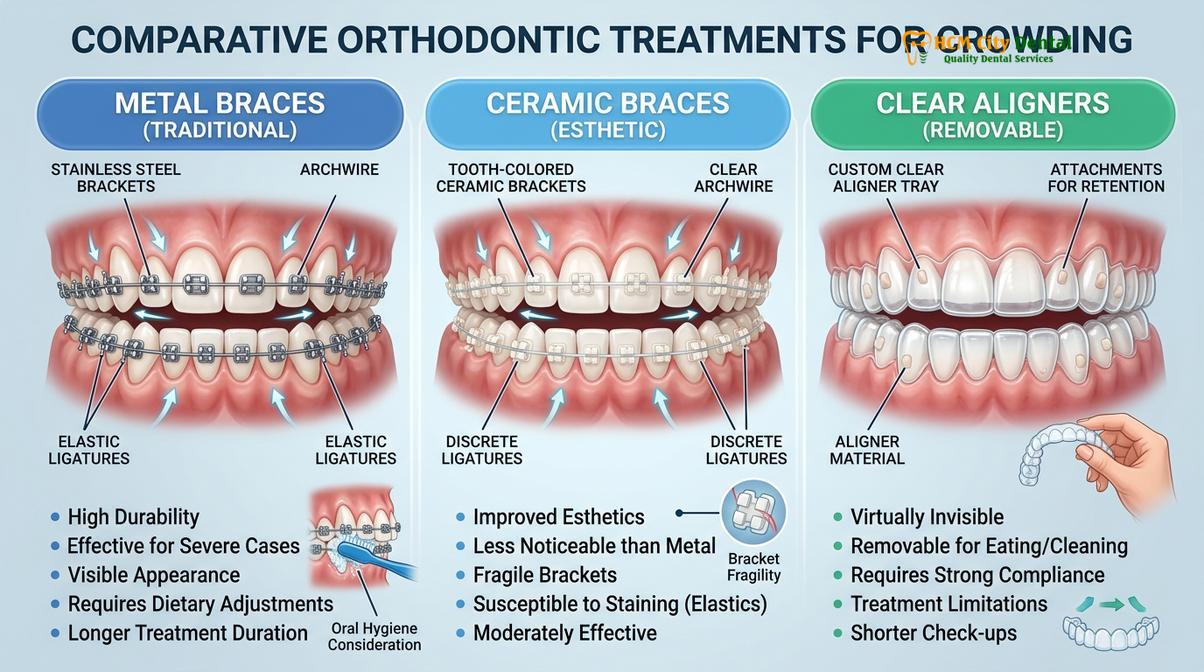
Below is a clinical comparison of the primary modalities used in overbite correction:
| Orthodontic Modality | Biomechanical Control | Aesthetic Profile | Ideal Clinical Application |
|---|---|---|---|
| Traditional Metal Braces | Maximum precision for complex root torque and heavy forces. | Highly visible; customizable with colored ligatures. | Severe skeletal overbites, impacted teeth, and cases requiring surgical orthodontics. |
| Ceramic Braces | Excellent control; functions identically to metal systems. | Discreet, tooth-colored appearance. | Adults and teens with moderate to severe overbites seeking a less visible fixed option. |
| Self-Ligating Braces | Low-friction mechanics; excellent for arch expansion. | Visible (metal) or discreet (clear options available). | Cases requiring significant arch development or correcting crowded dentition alongside the overbite. |
| Clear Aligners | Predictable for mild/moderate intrusion; relies on patient compliance. | Virtually invisible; removable for eating and hygiene. | Mild to moderate dental overbites in highly compliant adult and adolescent patients. |
Biomechanics and the Biological Response to Orthodontic Forces
Orthodontic tooth movement relies on the biological remodeling of the alveolar bone, driven by osteoclastic resorption and osteoblastic deposition in response to sustained mechanical pressure.
To truly understand the overbite braces process, one must look beyond the hardware and examine the cellular biology of tooth movement. Teeth are not rigidly fused to the jawbone; they are suspended in their sockets by a hammock-like network of fibers called the periodontal ligament (PDL). When braces or aligners apply a continuous, controlled force to a tooth, it compresses the PDL on one side of the root and stretches it on the opposite side.
This mechanical stress triggers a complex inflammatory cascade. On the compressed side, specialized cells called osteoclasts are recruited to break down the adjacent alveolar bone, clearing a path for the tooth to move. Simultaneously, on the stretched side, cells called osteoblasts deposit new bone tissue to fill the void left behind. This synchronized process of bone resorption and deposition is what allows orthodontists to safely move teeth through solid bone [4].
“The success of deep overbite correction hinges on the delicate balance of applying light, continuous forces. Excessive force can lead to PDL hyalinization and root resorption, whereas optimal biomechanics stimulate efficient osteoblastic and osteoclastic activity, ensuring safe and predictable alveolar remodeling.”
When correcting a deep overbite, the biological challenge is significant because the orthodontist is often attempting to intrude teeth. Intrusion requires very light, continuous forces to avoid damaging the tooth root. This is why the overbite braces process cannot be rushed. The bone must be given adequate time to remodel safely.
Clinical Case Study: Overbite Correction in Ho Chi Minh City
A structured clinical approach to a severe Class II malocclusion demonstrates the effectiveness of combining self-ligating brackets with targeted intermaxillary elastics.
Consider the case of a 24-year-old patient who presented to HCMC Dental Clinic in Ho Chi Minh City with a severe Class II Division 1 malocclusion. The patient exhibited a 7mm overjet and a 100% deep overbite, where the lower incisors were completely hidden behind the upper incisors upon closing. The primary chief complaint was difficulty in mastication and dissatisfaction with their facial profile.
Dr. Nguyen Van Cuong, a leading orthodontic specialist, emphasizes that precise biomechanical planning is the cornerstone of successful overbite correction. Dr. Cuong routinely utilizes advanced 3D cephalometric analysis to ensure that every patient receives a customized treatment protocol tailored to their specific skeletal and dental needs, often integrating strategies to fix overjet simultaneously to achieve optimal facial harmony.
The treatment plan involved the application of self-ligating metal brackets to facilitate arch expansion and reduce friction during anterior retraction. Bite turbos were immediately placed on the palatal surfaces of the maxillary central incisors to disocclude the posterior teeth, allowing for the extrusion of the premolars and molars. Over a period of 22 months, the patient strictly adhered to wearing Class II intermaxillary elastics. The final clinical transformation revealed a stable Class I occlusion, a normalized overbite of 2mm, and a significantly improved lower facial profile.
When to Consult an Orthodontist for an Overbite
Early diagnosis and intervention are critical for managing severe overbites, preventing excessive tooth wear, and guiding proper jaw development in growing patients.
Recognizing the signs of a problematic overbite early can significantly streamline the overbite braces process. According to clinical standards aligned with the Vietnam Ministry of Health guidelines for odonto-stomatology, early screening is highly recommended to intercept developing malocclusions [7]. Patients or parents should seek an orthodontic consultation if they observe any of the following clinical indicators:
- Severe Tooth Wear: The lower front teeth biting into the roof of the mouth or excessive grinding down of the enamel on the anterior teeth.
- Speech Impediments: Difficulty pronouncing certain consonants (like “s” or “th”) due to the abnormal position of the incisors.
- Masticatory Dysfunction: Pain or difficulty when chewing, often accompanied by clicking or popping in the temporomandibular joint (TMJ).
- Facial Asymmetry: A noticeably receding chin or a disproportionate lower facial third.
“Early orthodontic evaluation allows for the interception of skeletal discrepancies before jaw growth is complete, potentially eliminating the need for complex orthognathic surgery in adulthood and ensuring a more stable, functional occlusion.”

While early intervention is beneficial, it is important to note that adults can also undergo highly successful overbite correction. The biological principles of tooth movement remain the same regardless of age, provided the periodontal tissues are healthy and free of active disease.
References
- American Journal of Orthodontics and Dentofacial Orthopedics. Biomechanics of deep overbite correction. (2021).
- Angle Orthodontist. Skeletal and dental effects of Class II correction modalities. (2020).
- Journal of Clinical Orthodontics. The role of bite turbos and intrusion arches in adult orthodontics. (2019).
- European Journal of Orthodontics. Periodontal tissue response during anterior retraction. (2022).
- International Journal of Dentistry. Long-term stability and retention protocols following deep bite correction. (2018).
- Journal of the American Dental Association. Efficacy of clear aligner therapy in Class II malocclusions. (2023).
- Vietnam Ministry of Health (MOH). National Guidelines on Odonto-Stomatology and Orthodontic Interventions.
If you are experiencing functional difficulties or aesthetic concerns due to a deep bite, professional orthodontic intervention can help restore your oral health. To learn more about the overbite braces process and explore your personalized treatment options, schedule a consultation at HCMC Dental Clinic in Ho Chi Minh City today.



