

To design dental smiles is to integrate comprehensive facial analysis, periodontal health, and advanced prosthodontics to restore oral function and aesthetics. This clinical process utilizes digital imaging, precise material selection, and biomechanical engineering to create harmonious, long-lasting dentition tailored to the individual patient’s anatomy.
Clinical Summary:
The methodology to design dental smiles represents the pinnacle of modern restorative dentistry, merging biological principles with advanced CAD/CAM technology. Clinicians utilize comprehensive diagnostic data—including CBCT scans, intraoral photogrammetry, and dynamic occlusal analysis—to engineer restorations that offer both structural integrity and lifelike aesthetics. Treatment modalities range from ultra-thin lithium disilicate veneers to complex implant-supported prostheses. Success relies heavily on meticulous treatment planning, precise execution of tooth preparation, and the establishment of a stable periodontal foundation. By adhering to biomimetic principles, dental professionals can predictably restore the stomatognathic system, ensuring long-term functional harmony and patient satisfaction.
Key Takeaways:
- Digital smile design utilizes 3D imaging to predict restorative outcomes before irreversible preparation.
- Periodontal health and stable alveolar bone are mandatory prerequisites for aesthetic restorations.
- Material selection (e.g., zirconia vs. lithium disilicate) is dictated by occlusal forces and aesthetic demands.
- Implant-supported prostheses offer biomechanical advantages over traditional tissue-borne or tooth-borne alternatives.
- Long-term success requires rigorous maintenance protocols and management of parafunctional habits.
The Clinical Philosophy Behind Smile Design
Designing a smile requires a multidisciplinary approach that harmonizes the macro-aesthetics of facial proportions with the micro-aesthetics of individual tooth morphology and gingival architecture.
The contemporary approach to aesthetic dentistry transcends the mere replacement of missing or damaged tooth structure. To effectively design dental smiles, clinicians must adopt a holistic view of the patient’s stomatognathic system. This involves a deep understanding of facial symmetry, lip dynamics, phonetic constraints, and the intricate biomechanics of the temporomandibular joint (TMJ). The foundation of true comprehensive oral care relies on establishing a disease-free environment before any cosmetic enhancements are initiated. Active periodontal disease, endodontic pathology, or untreated carious lesions must be resolved to ensure the longevity of subsequent restorations[1].
Achieving optimal dental esthetics is a complex interplay between biology and material science. The gingival tissues serve as the frame for the teeth; therefore, managing the gingival zenith, papilla height, and biologic width is critical. If the restorative margins encroach upon the biologic width, the resulting chronic inflammation will compromise both the aesthetic outcome and the structural integrity of the supporting periodontium. A profound dental passion for continuous education is required for clinicians to master these nuances, ensuring that every preparation respects the delicate balance of the oral ecosystem.
Furthermore, the fabrication of lifelike restorations is an exacting dental craft. Master ceramists work in tandem with prosthodontists to replicate the optical properties of natural enamel and dentin. This includes managing translucency, opalescence, and fluorescence. Dr. Nguyen Van Cuong frequently emphasizes that a successful smile rehabilitation must not only look natural in static photographs but must also function seamlessly during dynamic movements such as speaking and chewing. The ultimate goal is to create natural smiles dental professionals and patients alike recognize as biologically sound and visually harmonious.

Macro and Micro-Aesthetic Parameters
Macro-aesthetics involves the evaluation of the face as a whole. Clinicians assess the interpupillary line, the facial midline, and the commissural line to ensure the proposed dental midline aligns appropriately. The incisal edge position of the maxillary central incisors is arguably the most critical starting point in smile design. It dictates the display of teeth at rest, during a dynamic smile, and plays a vital role in phonetics, particularly in the pronunciation of “F” and “V” sounds.
Micro-aesthetics focuses on the individual characteristics of the teeth. This includes the length-to-width ratio of the central incisors (ideally around 75-80%), the axial inclination of the anterior teeth, and the progression of the incisal embrasures. Surface texture, developmental lobes, and perikymata must be meticulously recreated in the ceramic restorations to scatter light in a manner identical to natural enamel. When discussing these intricate details, patients sometimes playfully ask how to porcelain pronounce specific ceramic classifications, but the clinical priority always remains on the material’s biocompatibility and fracture toughness.
Diagnostic Workflows and Digital Integration
Modern diagnostic workflows utilize intraoral scanners, CBCT imaging, and specialized CAD software to create a virtual patient, allowing for precise, predictable, and minimally invasive treatment planning.
The advent of digital dentistry has revolutionized the predictability of complex rehabilitations. The traditional workflow, which relied heavily on irreversible hydrocolloid impressions and analog facebow transfers, has been largely superseded by digital data acquisition. Intraoral 3D scanners capture the topography of the hard and soft tissues with micron-level accuracy. This digital impression is then merged with Cone Beam Computed Tomography (CBCT) data and high-resolution facial photographs to create a comprehensive “virtual patient.”
Proper dental space management is a prerequisite for any restorative work. Often, patients present with malocclusion, crowding, or uneven spacing that precludes the immediate placement of veneers or crowns. In such cases, pre-prosthetic orthodontic intervention is necessary to distribute the space optimally, ensuring that the final restorations have ideal proportions without requiring aggressive tooth reduction. Efficient clinic operations rely on robust practice management software with reliable open dental support to seamlessly integrate these massive digital files and coordinate multidisciplinary care[2].
“The integration of digital smile design protocols allows clinicians to transition from a reactive, tooth-by-tooth approach to a proactive, comprehensive rehabilitation strategy, significantly reducing the risk of biomechanical failure.”
The Digital Mock-Up and Intraoral Try-In
Once the digital design is finalized, a 3D-printed model of the proposed outcome is fabricated. A silicone matrix is derived from this model and filled with bis-acrylic material, which is then temporarily seated over the patient’s unprepared teeth. This “mock-up” serves as a powerful communication tool, allowing the patient to visualize the final result in their own mouth. More importantly, it allows the clinician to verify phonetics, lip support, and occlusal guidance before a single bur touches the enamel.
Restorative Modalities: Crowns, Bridges, and Implants
Selecting the appropriate restorative modality—whether tooth-borne crowns, fixed partial dentures, or implant-supported prostheses—depends on the structural integrity of the remaining dentition and the patient’s biomechanical needs.
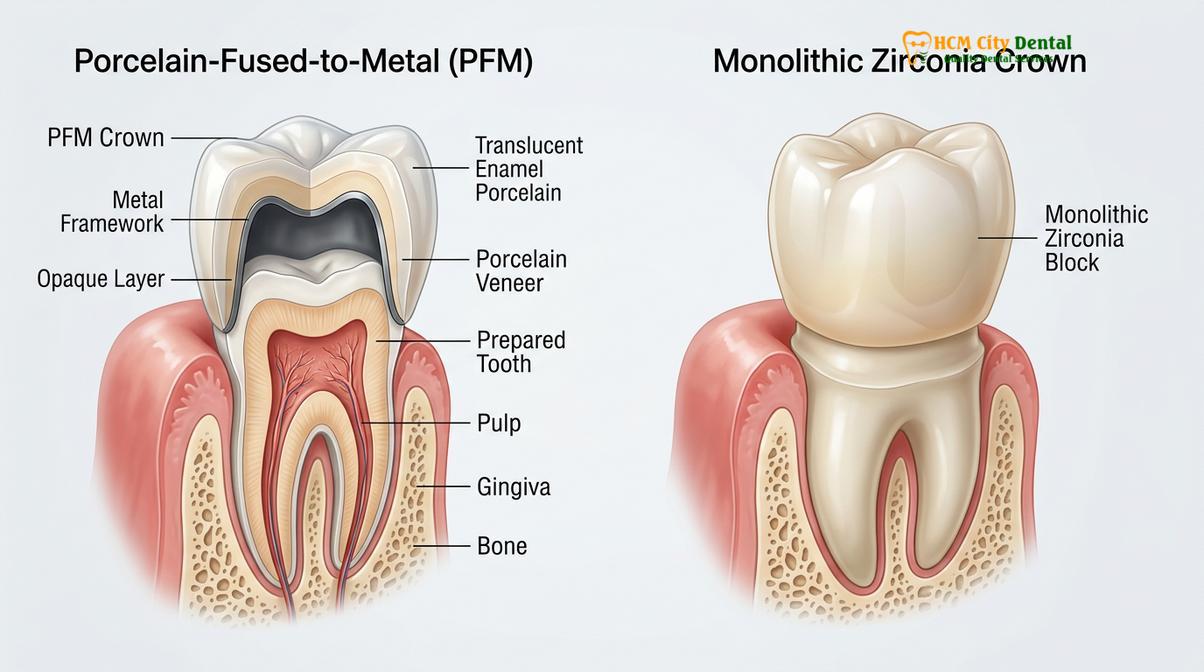
When teeth are heavily broken down, endodontically treated, or exhibit extensive structural compromise, full-coverage restorations are indicated. The design and fabrication of a custom ceramic restoration require meticulous attention to margin placement and occlusal reduction. Historically, PFM—where pfm stands for dental crowns made of Porcelain Fused to Metal—was the gold standard due to its high tensile strength. However, the opaque metal substructure often presented aesthetic challenges, particularly at the gingival margin where a dark line could become visible over time. Today, clinicians frequently transition to monolithic zirconia options or lithium disilicate, which offer superior light transmission while maintaining exceptional flexural strength[3].
For the replacement of missing teeth, clinicians must carefully evaluate the difference between dental bridge and implant therapies. A conventional fixed partial denture (bridge) requires the preparation of adjacent abutment teeth, which involves the irreversible removal of healthy enamel and dentin. Conversely, a dental implant replaces the missing tooth root, preserving the adjacent teeth and providing vital stimulation to the alveolar bone to prevent resorption. Discussing the pros and cons of dental implants vs bridges is a mandatory component of the informed consent process, ensuring patients understand the long-term biological implications of their choice.
Bridge Design and Conservative Alternatives
When a bridge is selected, optimal dental bridge design is critical for long-term success. The pontic (the artificial tooth) must be designed to allow for adequate oral hygiene while mimicking the natural emergence profile from the gingiva. Modified ridge lap or ovate pontics are clinically preferred as they create the illusion that the tooth is growing directly out of the gum tissue. For patients seeking conservative anterior replacements, they frequently inquire about the maryland bridge dental cost. A Maryland bridge utilizes resin-bonded wings attached to the lingual surfaces of adjacent teeth, minimizing preparation. However, clinicians must weigh the financial benefit against the statistically lower retention rates compared to conventional fixed prostheses.
| Modality | Primary Indication | Biomechanical Advantage | Clinical Limitation |
|---|---|---|---|
| Lithium Disilicate Veneers | Anterior aesthetic enhancement, minor shape/color correction | Maximum preservation of enamel, superior optical properties | Contraindicated for severe bruxism or heavily discolored substrates |
| Monolithic Zirconia Crowns | Posterior restorations, heavy occlusal load areas | Exceptional flexural strength, no metal substructure | Can be highly opaque if not properly characterized |
| Conventional Fixed Bridge | Short edentulous spans where adjacent teeth need crowns | Rapid restoration of function, predictable aesthetics | Requires irreversible preparation of adjacent abutment teeth |
| Endosseous Dental Implants | Single or multiple missing teeth, full-arch edentulism | Preserves adjacent teeth, maintains alveolar bone volume | Requires adequate bone volume and longer treatment time |
Navigating Implantology and Advanced Prosthetics
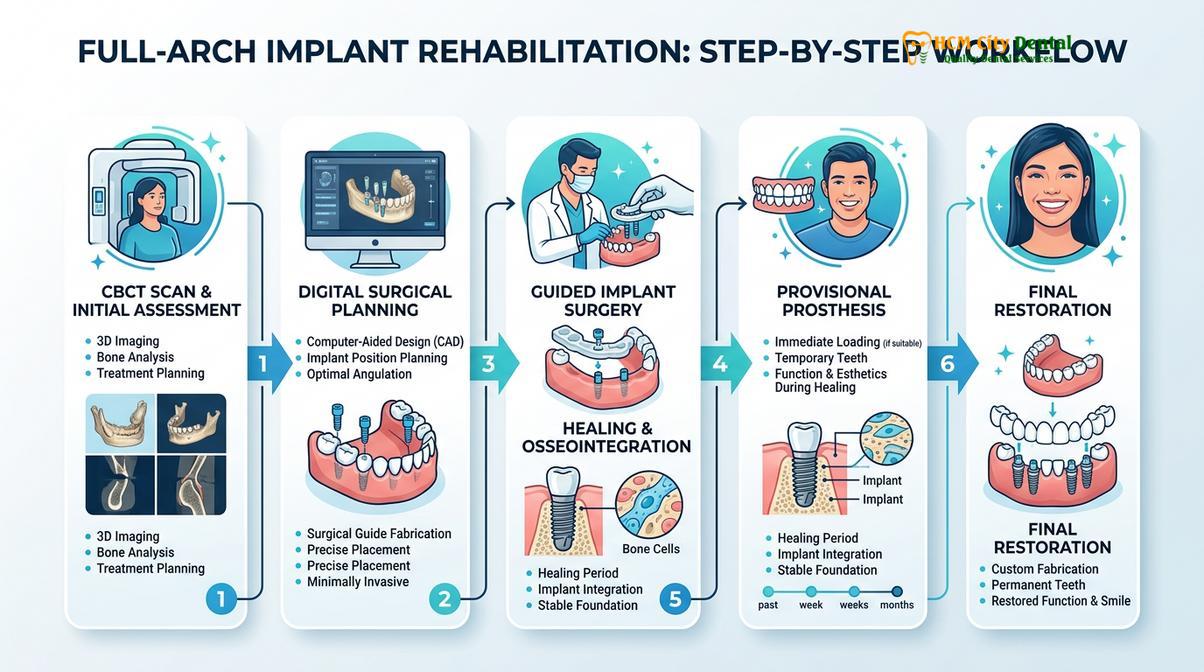
Implant dentistry provides the most biologically sound method for replacing missing teeth, requiring precise surgical planning to ensure optimal 3D positioning and long-term osseointegration.
The integration of dental implants into smile design has fundamentally shifted the paradigm of restorative dentistry. However, implantology is highly technique-sensitive. Inadequate surgical planning, poor 3D positioning, or failure to respect the biological width can lead to bad dental implants, characterized by crestal bone loss, peri-implantitis, or catastrophic mechanical failure. To mitigate these risks, clinicians utilize computer-guided surgery, where surgical stents dictate the exact angulation and depth of the osteotomy based on the pre-operative CBCT data.
For patients requiring full-arch rehabilitation, the options can be overwhelming. Some patients initially seek out corporate centers offering clear choice dental implants, drawn by the promise of immediate function. While these models advertise a standardized clear choice dental implants cost, individualized treatment planning in a private prosthodontic setting often yields superior aesthetic customization and long-term follow-up care. Geographic location also heavily influences treatment accessibility; for instance, the cost of dental implants in maryland or other Western regions often drives patients to seek high-quality medical tourism options, receiving advanced restorative protocols at specialized clinics in Southeast Asia[4].

Implant-Supported Bridges and Biomechanics
When multiple adjacent teeth are missing, an implant supported dental bridge offers excellent stability and biomechanical distribution of occlusal forces. Unlike natural teeth, which possess a periodontal ligament (PDL) that acts as a shock absorber, dental implants are ankylosed directly to the bone. This lack of proprioception means that occlusal forces are transmitted directly to the implant-bone interface. Therefore, the restorative material and occlusal scheme must be meticulously designed to prevent overloading. The use of multi-unit abutments and passive fit frameworks is essential to ensure the longevity of the prosthesis.
Achieving Natural Aesthetics and Function
The ultimate success of a smile design is measured by its ability to seamlessly integrate with the patient’s natural biology while withstanding the rigorous demands of daily mastication.
Aesthetic dentistry is not merely an exercise in creating white teeth; it is the pursuit of biomimicry. The optical properties of the final restorations must replicate the complex light dynamics of natural dentition. This requires a deep understanding of color science, including hue, chroma, and value. Value (the relative lightness or darkness) is the most critical dimension of color in dentistry; an incorrect value will make a restoration look artificial regardless of the hue. Clinicians must also consider the underlying substrate color, especially when utilizing translucent materials. In cases of severe tetracycline staining, comparing different ceramic materials is crucial, as highly opaque zirconia may be required to mask the discoloration before layering translucent porcelain on the facial surface.
The bonding protocol is equally critical. The use of specialized bonding agents ensures a micromechanical and chemical lock between the ceramic and the tooth structure. This adhesive integration not only provides retention but also reinforces the remaining tooth structure, distributing stress across the entire complex. To ensure reliable, daily smiles dental function, the restorative material must withstand maximum intercuspal forces without fracturing or causing excessive wear to the opposing natural dentition.
Clinical Case Study: Comprehensive Smile Rehabilitation
A 45-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City with severe occlusal wear, generalized attrition, and a collapsed vertical dimension of occlusion (VDO). The clinical workflow began with a digital smile design to determine the ideal incisal edge position and establish a new, functional VDO. Following periodontal optimization, a combination of monolithic zirconia crowns for the posterior segments and layered lithium disilicate veneers for the anterior sextant was utilized. The precise execution of adhesive protocols and occlusal equilibration resulted in a highly aesthetic, biomechanically stable rehabilitation that restored both function and confidence.
Maintenance, Hygiene, and Long-Term Care
The longevity of aesthetic restorations is heavily dependent on the patient’s commitment to rigorous home care and adherence to a professional maintenance schedule.
Even the most exquisitely designed dental smiles are susceptible to failure if not properly maintained. Patients must understand that ceramic restorations, while impervious to decay themselves, are attached to biological tissues that remain vulnerable to bacterial plaque. Recurrent caries at the restorative margin and periodontal inflammation are the primary causes of late-stage failure. When advising patients on maintenance, the debate of water flosser vs dental floss often arises. Clinical evidence suggests that while traditional string floss is excellent for tight interproximal contacts, water irrigation devices are highly effective for flushing out subgingival plaque, particularly under the pontics of fixed bridges and around implant abutments.
Because the cost to open a dental practice equipped with state-of-the-art CBCT, intraoral scanners, and milling technology is immense, clinics must maintain exceptionally high clinical standards to justify the investment and ensure patient outcomes. This includes providing comprehensive post-operative instructions and emphasizing the longevity of these restorations through proper care. Patients with a history of bruxism or clenching must be fitted with a hard acrylic occlusal guard to protect the ceramics from catastrophic fracture during sleep[5].
Clinical Warning: Aesthetic restorations do not eliminate the risk of biological disease. Failure to maintain meticulous oral hygiene or attend regular professional cleanings can lead to marginal leakage, secondary caries, and peri-implantitis, potentially resulting in the complete loss of the restorations and supporting bone.
“The true measure of a successful smile design is not how it looks on the day of insertion, but how it functions and integrates biologically a decade later. Maintenance is the unsung hero of restorative dentistry.”
When to See a Doctor for Smile Restoration
Patients should seek a professional consultation when they experience functional limitations, such as difficulty chewing, temporomandibular joint discomfort, or phonetic challenges related to missing or misaligned teeth. Additionally, signs of structural failure in existing restorations—such as chipping, marginal discoloration, or persistent gingival bleeding around crowns—warrant immediate clinical evaluation. Dr. Nguyen Van Cuong advises that early intervention is crucial; delaying treatment often leads to further deterioration of the alveolar bone and adjacent tooth structure, complicating future restorative efforts.
A comprehensive assessment at a specialized facility, such as HCMC Dental Clinic, allows for the early detection of occlusal disharmony and periodontal instability. Patients presenting with severe tooth wear, multiple missing teeth, or dissatisfaction with their current dental aesthetics should schedule a diagnostic appointment. The clinical team will utilize advanced 3D imaging and digital smile design protocols to formulate a personalized, evidence-based treatment plan that addresses both biological health and aesthetic desires.

Frequently Asked Questions
Clear, evidence-based answers to common patient inquiries regarding the clinical processes, material science, and long-term expectations of comprehensive smile design.
What is the clinical process to design dental smiles?
The clinical process involves digital facial analysis, periodontal assessment, and 3D CAD/CAM modeling to create a customized restorative plan. Dentists evaluate the patient’s dynamic occlusion, gingival architecture, and phonetics to ensure the final ceramic or composite restorations function harmoniously within the stomatognathic system. This meticulous planning phase prevents biomechanical errors and ensures predictable aesthetic outcomes.
How do dentists determine the correct restorative material for a smile makeover?
Material selection is based on the patient’s occlusal forces, parafunctional habits, and aesthetic requirements. Clinicians may choose lithium disilicate for highly aesthetic anterior veneers, while monolithic zirconia is often preferred for posterior crowns or implant-supported bridges due to its superior flexural strength. The underlying tooth color and the required thickness of the restoration also heavily influence the final material choice.
Can digital smile design predict the final outcome accurately?
Yes, modern digital smile design utilizes intraoral scanners and specialized software to provide highly accurate predictive models. Patients can preview their proposed restorations through digital mock-ups and temporary bis-acrylic intraoral try-ins before any irreversible tooth preparation occurs. This allows for adjustments in tooth length, shape, and phonetics, ensuring patient satisfaction prior to final fabrication.
What role does periodontal health play in aesthetic dentistry?
Periodontal health is the absolute foundation of any aesthetic dental procedure. Without healthy, inflammation-free gingival tissues and adequate alveolar bone support, restorations are prone to marginal leakage, aesthetic failure, and biological complications such as peri-implantitis or recurrent caries. Establishing a stable periodontal baseline is mandatory before initiating any definitive restorative work.
How long do comprehensive smile restorations typically last?
With meticulous oral hygiene and routine professional maintenance, high-quality ceramic restorations can last over a decade. Longevity depends heavily on the patient’s adherence to home care protocols, the use of occlusal guards if bruxism is present, and the biomechanical precision of the initial treatment. Regular clinical evaluations are necessary to monitor marginal integrity and occlusal stability over time.
References
- Journal of Prosthetic Dentistry. Digital workflows in comprehensive aesthetic dentistry and smile design. (2021).
- International Journal of Periodontics & Restorative Dentistry. Biologic width and gingival margin placement in restorative dentistry. (2020).
- Clinical Oral Implants Research. Long-term survival rates of implant-supported fixed partial dentures. (2019).
- Journal of Esthetic and Restorative Dentistry. Material selection for anterior ceramic veneers and crowns. (2022).
- Journal of the American Dental Association. Biomechanical considerations in the design of fixed prosthodontics. (2018).



