

Dental veneer adhesive is a specialized resin-based cement used to permanently bond porcelain or composite laminates to the natural tooth structure. This clinical-grade bonding agent ensures optimal marginal seal, structural durability, and aesthetic integration while preventing microleakage and bacterial infiltration beneath the restoration.
Clinical Summary:
The success of aesthetic restorations relies heavily on the quality and application of the dental veneer adhesive. Modern bonding protocols utilize light-cured or dual-cured resin cements that chemically and mechanically lock the ceramic to the etched enamel. Proper isolation, minimal tooth preparation (0.3mm – 0.5mm), and precise digital or physical impressions are critical for a seamless fit. At facilities like HCMC Dental Clinic, advanced Digital Smile Design (DSD) and premium materials like Swiss e.max ensure high success rates and long-lasting cosmetic outcomes.
Key Takeaways:
- Veneer adhesives are advanced resin cements requiring strict moisture control for optimal bond strength.
- Minimal tooth preparation of 0.3mm to 0.5mm preserves enamel, which is crucial for secure adhesion.
- Light-cured cements offer superior color stability, making them ideal for highly translucent anterior restorations.
- Accurate digital scanning or physical impressions dictate the marginal fit and long-term success of the bonding interface.
- Post-treatment care, including the use of protective night guards, prevents mechanical failure of the adhesive bond.
The Clinical Science Behind Dental Veneer Adhesive
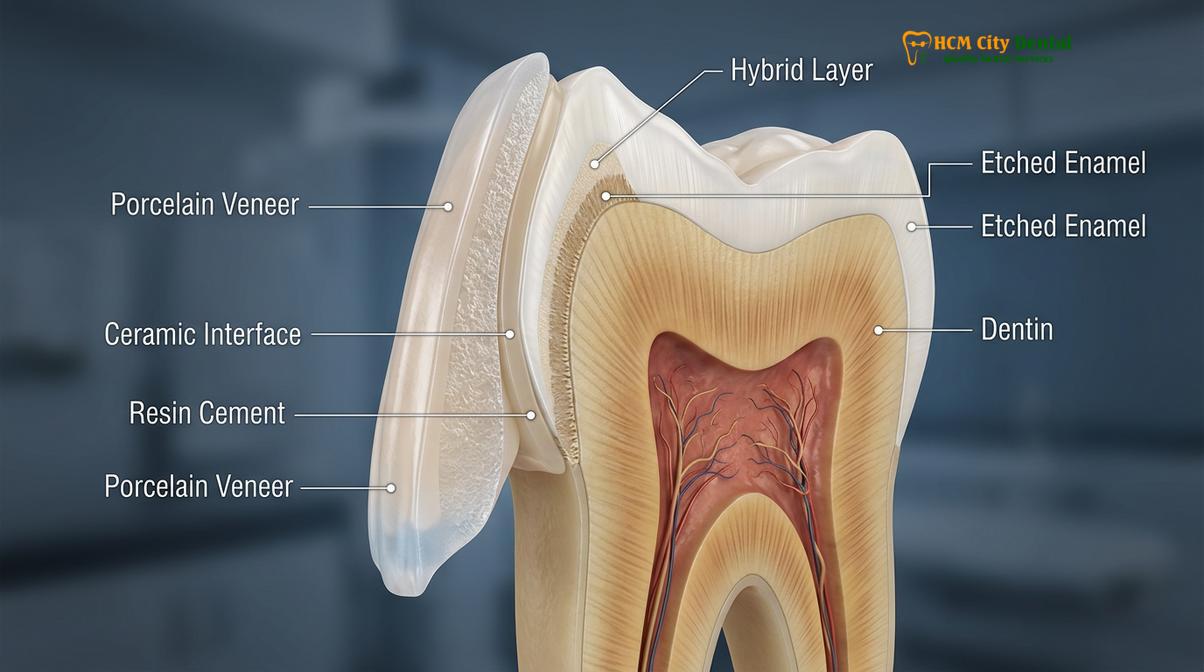
Dental veneer adhesives are sophisticated resin-based cements designed to create a micromechanical and chemical bond between the ceramic restoration and the natural tooth enamel.
The foundation of modern cosmetic dentistry rests upon the predictable and durable adhesion of restorative materials to the natural tooth structure. A high-quality dental veneer adhesive is not merely a “glue”; it is a complex biomaterial engineered to bridge the gap between organic tooth tissue and inorganic ceramic. The primary mechanism of this adhesion relies on the creation of a hybrid layer. When the tooth enamel is treated with phosphoric acid, microscopic porosities are formed. The fluid resin adhesive penetrates these porosities, and upon polymerization via a curing light, it forms resin tags that mechanically lock the restoration in place[1].

In clinical practice, dentists primarily utilize light-cured resin cements for anterior veneers. Unlike dual-cured cements, which contain chemical initiators that can degrade and cause yellowing over time, purely light-cured adhesives offer exceptional long-term color stability. This is paramount when placing highly translucent lithium disilicate restorations, where any underlying discoloration would be visible through the ceramic. During the initial consultation, clinicians must thoroughly discuss the dental veneers pros and cons, explaining how the choice of adhesive directly impacts both the aesthetic longevity and the structural integrity of the smile.
The biochemical composition of these adhesives typically includes a matrix of Bis-GMA or TEGDMA monomers, combined with inorganic filler particles that enhance compressive strength and reduce polymerization shrinkage. Furthermore, the use of a silane coupling agent on the intaglio (inner) surface of the porcelain is a critical step. Silane acts as a chemical bridge, featuring a silanol group that bonds to the silica in the porcelain and a methacrylate group that copolymerizes with the resin cement. This dual-action bonding protocol ensures that the veneer functions as a unified structural component of the tooth.
Preparation and Impression Workflows for Veneer Bonding
Achieving a flawless adhesive bond requires conservative tooth preparation and highly accurate replication of the dental arch through digital or traditional impression techniques.
The longevity of a dental veneer adhesive bond is intrinsically linked to the quality of the tooth preparation. Contemporary protocols emphasize minimal intervention dentistry, typically requiring only 0.3mm to 0.5mm of enamel reduction. Because the bond strength of resin cement to enamel is significantly higher and more predictable than its bond to dentin, preserving the enamel layer is a primary clinical objective. This conservative approach not only maximizes adhesive retention but also minimizes post-operative sensitivity and preserves the biomechanical vitality of the tooth.
Once the teeth are meticulously prepared, capturing their exact geometry is the next critical phase. The traditional method of making dental impressions using polyvinyl siloxane (PVS) materials has long been the gold standard. However, this process requires meticulous technique to avoid voids, pulls, or distortions. Modern impressions dental care protocols emphasize the transition toward digital intraoral scanning. Utilizing leading edge dental technology, clinicians can capture highly accurate 3D models of the prepared teeth in real-time. This digital workflow eliminates the discomfort often associated with traditional impression trays and provides the dental laboratory with a flawless dataset for milling or pressing the restorations.
The process of taking dental impressions has evolved significantly at advanced facilities. For instance, Dr. Nguyen Van Cuong at HCMC Dental Clinic utilizes state-of-the-art intraoral scanners integrated with Digital Smile Design (DSD) software. This allows for unparalleled precision in capturing the preparation margins. A precise margin ensures that the dental veneer adhesive forms a microscopic, flush seal between the ceramic and the tooth, preventing the ingress of bacteria and subsequent secondary caries[2]. Whether utilizing digital or analog methods, the accuracy of the impression directly dictates the passive fit of the veneer, which in turn dictates the stress placed on the adhesive layer.
Material Selection: E.max vs. Zirconia Veneers in Saigon
The choice between lithium disilicate and monolithic zirconia dictates the specific adhesive protocol required to achieve maximum retention and aesthetic vitality.
When planning aesthetic restorations, the selection of the ceramic material is a pivotal decision that influences the entire adhesive workflow. In Ho Chi Minh City, patients have access to world-class materials at highly competitive rates. According to the latest clinic fee schedules, premium Swiss e.max (pressed lithium disilicate) veneers typically range from $250 to $400 per tooth, while highly durable Zirconia veneers range from $300 to $450 per tooth. Facilities like HCMC Dental Clinic often provide comprehensive packages, including a 3-year clinic bonding warranty, ISO certification standards, and manufacturer authenticity cards. Furthermore, international patients utilizing WhatsApp pre-bookings can often access specialized promotional rates, sometimes up to a 40% discount on extensive smile makeovers.
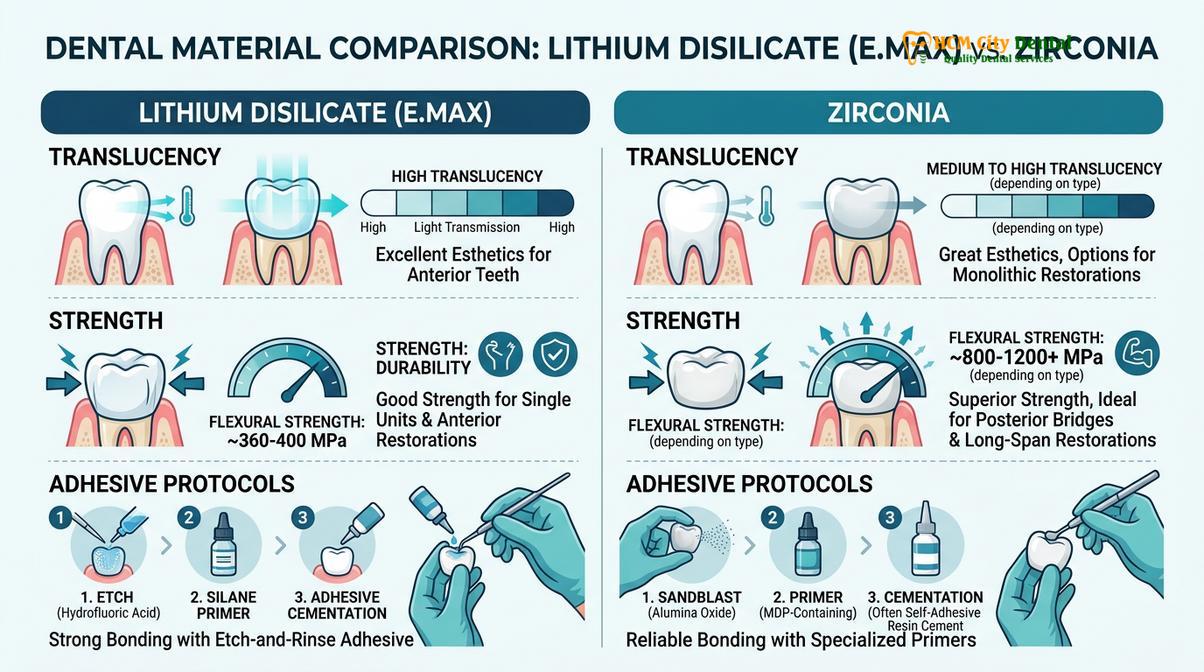
The clinical distinction between these materials lies in their optical properties and their interaction with dental veneer adhesive. Lithium disilicate (e.max) is a glass-ceramic renowned for its lifelike translucency and opalescence. Because it contains a high silica content, it can be etched with hydrofluoric acid, creating a highly retentive micro-topography. When combined with a silane primer and a light-cured resin cement, e.max achieves an exceptionally strong micromechanical and chemical bond. This makes it the premier choice for anterior teeth where achieving a seamless edge dental margin and natural light transmission are paramount.

Conversely, zirconia is a polycrystalline ceramic devoid of silica. It cannot be etched with hydrofluoric acid. To bond zirconia veneers, clinicians must employ air-particle abrasion (sandblasting) to roughen the surface, followed by the application of a specialized primer containing 10-Methacryloyloxydecyl dihydrogen phosphate (MDP). The MDP monomer chemically bonds to the metal oxides within the zirconia. While zirconia offers superior flexural strength, its higher opacity and complex bonding requirements mean it is often reserved for patients with heavy occlusal forces or those requiring masking of severely discolored underlying dentin[3].
| Material Type | Aesthetic Profile | Adhesive Protocol | Estimated Cost (Saigon) | Primary Indication |
|---|---|---|---|---|
| Lithium Disilicate (e.max) | High translucency, natural opalescence | HF Acid Etch + Silane + Light-Cure Resin | $250 – $400 / tooth | Anterior smile makeovers, minimal prep |
| Monolithic Zirconia | High strength, moderate to high opacity | Sandblasting + MDP Primer + Dual-Cure Resin | $300 – $450 / tooth | Bruxism cases, masking dark stumps |
| Composite Resin | Moderate aesthetics, susceptible to staining | Direct bonding, no laboratory fabrication | Variable | Temporary solutions, minor edge repairs |
Understanding these material science principles is essential for patients seeking General & Preventive Dentistry and advanced cosmetic rehabilitation. The correct pairing of material and adhesive ensures that the restoration not only looks beautiful but withstands the rigorous demands of the oral environment.
The Step-by-Step Adhesive Veneer Placement Protocol
The clinical bonding sequence involves meticulous isolation, acid etching, silane application, and controlled light polymerization to ensure a durable and microleakage-free restoration.
The final placement of porcelain veneers is one of the most technique-sensitive procedures in restorative dentistry. A single misstep in moisture control or chemical application can compromise the entire dental veneer adhesive bond. The protocol begins with the removal of any provisional restorations and the thorough cleaning of the prepared teeth using a non-fluoridated pumice slurry. This removes temporary cement residue and biofilm, ensuring a pristine substrate for bonding.
Try-In and Shade Verification
Before any permanent adhesive is applied, the clinician must verify the fit, marginal adaptation, and aesthetic integration of the veneers. Because the final color of a translucent veneer is influenced by the underlying tooth, the ceramic, and the cement, dentists utilize water-soluble try-in pastes. These pastes mimic the exact shade of the final cured resin cement. Once the patient and clinician approve the aesthetics, the veneers are removed, thoroughly rinsed, and prepared for the final bonding sequence.
Surface Treatment and Isolation
Meticulous isolation is non-negotiable. The use of a rubber dam or advanced lip-and-cheek retractors (such as Optragate) combined with high-volume suction is mandatory to prevent saliva or crevicular fluid from contaminating the bonding surfaces. The intaglio surface of the e.max veneer is etched with 5% to 9% hydrofluoric acid for 20 seconds, rinsed, and dried. A silane coupling agent is then applied and allowed to volatilize, rendering the ceramic surface reactive to the resin cement.
“The longevity of a bonded ceramic restoration is directly proportional to the rigor of the isolation protocol. Even microscopic moisture contamination during the application of the dental veneer adhesive can lead to premature debonding, marginal staining, and secondary caries.”
Etching, Bonding, and Polymerization
Simultaneously, the natural tooth structure is treated. The enamel is etched with 37% phosphoric acid for 15 to 30 seconds, creating the necessary microporosities. After thorough rinsing and gentle drying (avoiding desiccation of any exposed dentin), a universal bonding agent is applied and air-thinned to evaporate the solvent. The chosen light-cured resin cement is then loaded into the veneer, which is gently seated onto the tooth.
Excess cement is carefully removed from the margins using a microbrush or explorer. A brief “tack cure” of 1 to 2 seconds is often performed to gel the cement, allowing for easier removal of interproximal excess using dental floss. Finally, a glycerin gel is applied over the margins to prevent the formation of an oxygen inhibition layer, and the restoration is fully polymerized using a high-intensity LED curing light for 20 to 40 seconds per surface[4]. This comprehensive workflow ensures a robust, long-lasting integration of the advanced dental crown restorations and veneers.
Biomechanical Considerations and Managing Complications
Long-term adhesive success depends on strict adherence to clinical protocols, proper occlusal management, and patient compliance with post-operative care instructions.
While modern dental veneer adhesives exhibit extraordinary bond strengths, they are not impervious to biomechanical failure if subjected to excessive or misdirected forces. The oral cavity is a dynamic environment where restorations face constant thermal cycling, pH fluctuations, and immense masticatory pressures. Understanding the biomechanics of occlusion is critical. If a patient has an unbalanced bite or anterior interferences, the shearing forces can exceed the tensile strength of the adhesive, leading to cohesive failure of the ceramic or adhesive debonding.
Clinical Warning: Patients with severe, unmanaged bruxism (teeth grinding) or clenching habits are at a significantly higher risk of veneer fracture and adhesive failure. In such cases, comprehensive occlusal equilibration and the fabrication of a protective night guard are mandatory prerequisites to aesthetic treatment.
Patients with parafunctional habits are routinely prescribed a custom dental gum shield (occlusal splint) to protect their investment during sleep. This appliance absorbs and redistributes the forces of bruxism, safeguarding the delicate ceramic margins and the underlying adhesive bond. Furthermore, patients must be educated on proper maintenance. While the porcelain itself will not decay, the underlying tooth structure remains vulnerable. Meticulous oral hygiene and regular professional cleanings are essential to prevent gingival recession and root caries, which can undermine the restoration.
Clinical Case Review: A 34-year-old patient presented to HCMC Dental Clinic in Ho Chi Minh City with a history of recurrent debonding of composite veneers placed at a different facility. Dr. Nguyen Van Cuong conducted a comprehensive diagnostic evaluation, identifying inadequate enamel preparation and heavy anterior guidance as the root causes. The treatment plan involved conservative re-preparation, digital scanning, and the fabrication of six maxillary e.max veneers. Utilizing a strict rubber dam isolation protocol and a premium light-cured dental veneer adhesive, the new restorations were bonded seamlessly. A custom occlusal splint was provided post-operatively. At the two-year follow-up, the margins remained pristine with zero signs of microleakage or debonding.
In cases where a restoration suffers trauma, clinicians must evaluate whether the damage is a cohesive fracture of the porcelain or an adhesive failure at the tooth interface. Minor chips can sometimes be polished or repaired using specialized protocols, as detailed in guides on managing chipped restorations. However, catastrophic debonding usually requires complete removal of the residual cement, re-preparation, and fabrication of a new veneer.
“Aesthetic dentistry is as much about functional harmony as it is about visual beauty. The most advanced dental veneer adhesive cannot compensate for poor treatment planning or a hostile occlusal environment. Comprehensive diagnostics are the bedrock of longevity.”
For patients considering extensive rehabilitations, understanding the lifespan of dental restorations and the factors that influence their durability is crucial. Facilities that prioritize supreme dental care standards will always emphasize the importance of the adhesive protocol as the critical link between the laboratory’s artistry and the patient’s clinical reality.
When to See a Doctor for Veneer Complications
While professionally bonded veneers have a high success rate, patients should remain vigilant for signs of adhesive degradation or structural compromise. Early intervention can often prevent the complete failure of the restoration and protect the underlying tooth from decay.

You should schedule a clinical evaluation if you experience any of the following symptoms:
- Thermal Sensitivity: Sudden or prolonged sensitivity to hot or cold temperatures may indicate microleakage, where the dental veneer adhesive seal has been breached, allowing fluids to reach the dentinal tubules.
- Marginal Discoloration: A dark line or brown staining appearing at the junction between the veneer and the gum line suggests that the adhesive is degrading or that secondary decay is forming beneath the ceramic.
- Mobility or Shifting: If a veneer feels loose, clicks when you bite, or shifts slightly, the adhesive bond has failed. Do not attempt to wiggle it, as this can fracture the porcelain.
- Gingival Inflammation: Persistent redness, swelling, or bleeding of the gums around a specific veneer can indicate an overhang of excess cement that was not properly removed, or a biological width violation requiring professional correction.
- Trauma or Chipping: Any physical impact that results in a visible crack or chip in the veneer requires immediate assessment to determine if the structural integrity of the restoration has been compromised.
If a veneer completely detaches, keep it in a safe, dry container and contact your dental provider immediately. Never use household glues or over-the-counter adhesives to reattach it, as these substances are toxic, will ruin the fit of the veneer, and can cause irreversible damage to the tooth pulp[5]. For expert evaluation and advanced aesthetic solutions, patients can consult the specialists at HCMC Dental Clinic to ensure their smile remains healthy and structurally sound.
Frequently Asked Questions
How long does dental veneer adhesive take to fully set?
Dental veneer adhesive sets almost instantly upon exposure to a specialized curing light, though the chemical bond continues to mature over 24 hours. Clinicians use a high-intensity LED curing light to polymerize the resin cement, ensuring immediate stability before the patient leaves the clinic. Patients can typically resume normal eating and drinking shortly after the appointment, though it is advisable to avoid extremely hard or sticky foods for the first day.
Can veneer adhesive fail or wash out over time?
While modern resin adhesives are highly durable and insoluble in oral fluids, failure can occur due to poor isolation during placement or excessive occlusal forces. Regular dental checkups and proper oral hygiene are essential to maintain the integrity of the marginal seal. If the initial bonding protocol was compromised by moisture, the adhesive may degrade, leading to microleakage and eventual debonding.
Is the bonding process for e.max different from zirconia?
Yes, the bonding protocol differs significantly between materials. Lithium disilicate (e.max) requires hydrofluoric acid etching and silane application, whereas zirconia requires sandblasting and a specialized primer containing MDP monomers to achieve a strong chemical bond. Because zirconia lacks the silica matrix found in e.max, it relies heavily on this chemical primer and dual-cured resin cements for optimal retention.
Does the adhesive affect the final color of the veneer?
Yes, the shade and opacity of the dental veneer adhesive can subtly alter the final appearance of highly translucent porcelain. Dentists often use water-soluble try-in pastes to preview the color before committing to the final light-cured cement. This allows the clinician to warm up or cool down the final shade, ensuring a perfect match with the adjacent natural teeth.
What should I do if a veneer debonds or falls off?
If a veneer debonds, keep the restoration safe and contact your dentist immediately for an evaluation. Do not attempt to reattach it with over-the-counter glues, as this can damage the porcelain and the underlying tooth structure, complicating professional rebonding. The dentist will need to clean the residual cement from both the tooth and the veneer, re-treat the surfaces, and apply a fresh layer of clinical adhesive.
References
- Journal of Prosthetic Dentistry. Adhesion to silica-based ceramics and zirconia. (2021).
- Dental Materials. Clinical performance of light-cured resin cements. (2020).
- International Journal of Esthetic Dentistry. Minimal intervention dentistry and veneer preparations. (2019).
- Journal of Clinical Pediatric Dentistry. Managing dental anxiety during restorative procedures. (2022).
- Clinical Oral Investigations. Long-term survival of lithium disilicate veneers. (2018).



