

Using dental wax for a chipped tooth provides immediate, temporary relief by covering sharp enamel edges and preventing painful lacerations to the tongue and buccal mucosa. While it effectively shields soft tissues and reduces temperature sensitivity, it is not a permanent structural repair and requires prompt professional clinical evaluation.
Clinical Summary:
Dental wax serves as a crucial first-aid material in the management of acute dental trauma, specifically for uncomplicated crown fractures. Composed of non-toxic, thermoplastic materials like paraffin and beeswax, it acts as a physical barrier over jagged enamel and exposed dentinal tubules. This temporary measure mitigates soft tissue trauma and reduces dentinal hypersensitivity driven by fluid dynamics. However, dental wax lacks structural integrity and marginal sealing capabilities, making it unsuitable for prolonged use. Definitive treatment requires clinical assessment to rule out pulpal involvement, followed by permanent restorative procedures such as composite bonding, porcelain veneers, or full-coverage crowns. Patients experiencing dental trauma should utilize wax solely as a palliative bridge while immediately seeking professional emergency dental care to prevent bacterial microleakage and irreversible pulpal damage.
Key Takeaways:
- Dental wax acts as a non-toxic physical barrier, shielding the tongue and oral mucosa from sharp, fractured enamel edges.
- It provides temporary relief from thermal sensitivity by covering exposed dentinal tubules but does not restore structural integrity.
- Successful application requires isolating the tooth and thoroughly drying the enamel surface to ensure optimal wax adhesion.
- Prolonged reliance on wax without professional intervention increases the risk of cariogenic bacterial microleakage and pulpal inflammation.
- Permanent clinical solutions range from direct composite resin bonding to indirect restorations like a dental tooth cap.
The Clinical Role of Dental Wax in Dental Emergencies
Dental wax functions as an essential emergency barrier in dental traumatology, protecting the oral soft tissues from lacerations caused by jagged enamel while temporarily reducing dentinal hypersensitivity.
When a patient experiences a traumatic impact or bites down on a hard object, the resulting mechanical stress can exceed the tensile strength of enamel, leading to a fracture. In the immediate aftermath of such an event, the primary clinical concerns are the prevention of soft tissue injury and the mitigation of pain. The tongue, lips, and buccal mucosa are highly vascular and sensitive; constant friction against a sharp, newly fractured enamel margin can rapidly cause painful ulcerations and lacerations. In these acute scenarios, applying dental wax for a chipped tooth is a highly effective, conservative first-aid measure.[1]
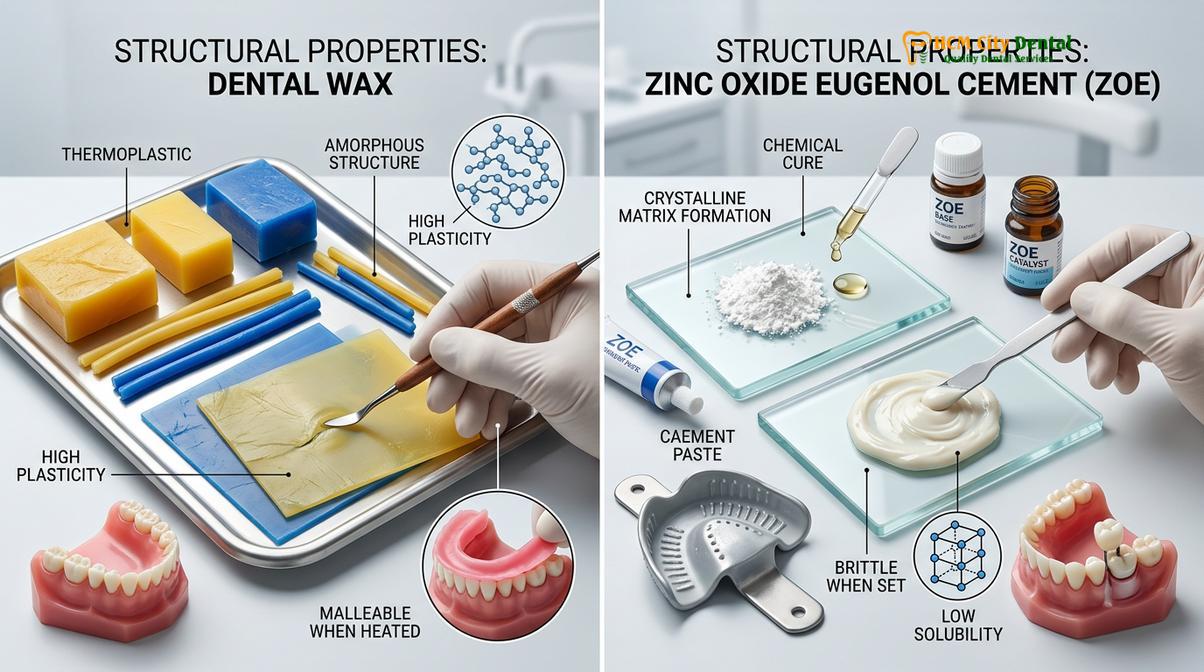
From a material science perspective, medical-grade dental wax is a thermoplastic blend, typically comprising paraffin, beeswax, and carnauba wax. This specific composition gives the material a unique rheological property: it remains solid at room temperature but becomes highly malleable and moldable when exposed to the natural warmth of human hands and the oral cavity.[2] Because it is entirely non-toxic and biocompatible, it poses no systemic risk if a small fragment is inadvertently swallowed during use.

Beyond soft tissue protection, dental wax plays a secondary role in managing dentinal hypersensitivity. According to Brännström’s hydrodynamic theory, when the protective enamel layer is sheared away, the underlying dentinal tubules are exposed to the oral environment. Changes in temperature (from hot or cold beverages) or osmotic pressure (from sweet foods) cause the fluid within these microscopic tubules to expand or contract rapidly. This fluid movement stimulates the mechanoreceptors of the odontoblasts and the A-delta nerve fibers within the pulp, registering as a sharp, piercing pain. By placing a dense layer of wax over the exposed dentin, the patient effectively creates a temporary thermal and physical insulator, halting the rapid fluid shifts and providing palliative relief until they can access emergency dental care.[3]
Step-by-Step Guide: How to Apply Dental Wax for a Chipped Tooth
Proper application of dental wax requires isolating the fractured tooth, thoroughly drying the enamel surface, and molding a warmed, pea-sized amount of wax securely over the sharp margins.
Achieving a secure and effective seal with dental wax requires a specific application protocol. Because dental wax is inherently hydrophobic (water-repellent), it will not adhere to a tooth surface that is coated in saliva. Patients attempting to apply wax at home must carefully prepare the site to ensure the material remains in place and provides adequate protection.
Step 1: Oral Debridement and Assessment
Before applying any material to a traumatized tooth, the oral cavity must be gently cleansed. The patient should rinse with warm water or a mild saline solution to remove any loose enamel fragments, food debris, or blood. During this step, it is crucial to visually inspect the fracture. If there is active bleeding originating from the center of the tooth (the pulp chamber), wax should not be applied, as this indicates a complicated fracture requiring immediate endodontic triage.
Step 2: Isolation and Moisture Control
Moisture control is the most critical step for successful wax adhesion. The patient should use clean cotton rolls, sterile gauze, or a clean tissue to isolate the chipped tooth from the tongue and cheeks. The fractured surface must be patted completely dry. Even a microscopic layer of salivary pellicle can prevent the wax from gripping the micro-undercuts of the fractured enamel.
Clinical Warning: Do not attempt to apply dental wax if the fractured tooth segment is highly mobile or if the patient is experiencing severe, spontaneous throbbing pain. These are signs of severe periodontal ligament trauma or irreversible pulpitis, and placing pressure on the tooth during wax application may exacerbate the injury or pose an aspiration risk.
Step 3: Preparation of the Wax
Pinch off a small piece of dental wax, approximately the size of a small pea or a popcorn kernel. Using clean fingers, roll the wax into a sphere. The mechanical friction and body heat will soften the wax, transitioning it from a rigid state to a pliable, putty-like consistency. This thermoplastic softening is essential for adapting the wax to the complex topography of the broken tooth.
Step 4: Application and Adaptation
Press the softened wax directly over the sharp edge of the chipped tooth. Using the pad of the index finger, gently mold the edges of the wax so that it tapers smoothly onto the remaining intact enamel. This tapering creates a mechanical lock, preventing the wax from easily rolling off during normal speech and minimal oral function. Once applied, the patient should avoid chewing on that side of the mouth and refrain from consuming hot liquids, which will rapidly melt the protective barrier.

Comparing Temporary Relief: Dental Wax vs. OTC Repair Kits
While dental wax offers excellent soft tissue protection, over-the-counter repair kits provide a more durable temporary structural seal using zinc oxide-based cements for emergency management.
When patients suffer a dental fracture outside of normal clinical hours, they often face a choice between using orthodontic dental wax or purchasing an over-the-counter (OTC) temporary tooth repair kit. Understanding the biomechanical differences between these materials is vital for appropriate emergency self-care.
Dental wax is purely a palliative physical barrier. It has zero compressive strength and will deform immediately under occlusal loading (biting forces). Its primary indication is for small to moderate enamel fractures where the main complaint is soft tissue irritation. Conversely, OTC temporary repair kits typically contain a form of Zinc Oxide Eugenol (ZOE) or a moisture-activated temporary cement. These materials undergo an actual chemical setting reaction when exposed to saliva, hardening into a chalk-like substance.
Eugenol, derived from clove oil, has a well-documented obtundent (soothing) effect on the dental pulp, making ZOE-based temporary cements highly effective for deeper fractures that expose significant dentin. However, temporary cements are much more difficult for a patient to apply correctly at home. If the cement is left high in the bite, it can cause severe trauma to the periodontal ligament when the patient closes their jaw. Therefore, for patients who simply need to cover a sharp edge until morning, wax remains the safest and most foolproof option.
| Material Type | Primary Clinical Indication | Advantages | Limitations |
|---|---|---|---|
| Orthodontic Dental Wax | Sharp enamel edges, minor chips, soft tissue protection. | Non-toxic, easy to apply, easily removable, zero risk of altering the bite. | No structural strength, melts with heat, must be removed before eating. |
| OTC Temporary Cement (ZOE) | Deep fractures, lost fillings, exposed dentin with sensitivity. | Hardens in saliva, provides a temporary marginal seal, soothing to the pulp. | Difficult to apply smoothly, risk of creating a high bite, harder to remove. |
| Sugar-Free Gum (Emergency) | Absolute last resort when wax or cement is unavailable. | Readily available, moldable. | High risk of introducing bacteria, poor adhesion, easily dislodged. |
Regardless of the temporary material chosen, neither serves as a substitute for professional restorative dentistry. Patients who use these materials must still seek definitive care, such as replacing a lost filling or repairing the fracture, as soon as possible.
Clinical Limitations and Risks of Prolonged Wax Usage
Relying on dental wax beyond a few days traps cariogenic bacteria against exposed dentin, accelerating decay and significantly increasing the risk of irreversible pulpal inflammation.
A common clinical error made by patients is assuming that because the dental wax has eliminated their pain and protected their tongue, the dental emergency is resolved. This misconception can lead to severe, sometimes irreversible, dental complications. Dental wax is strictly a provisional measure designed to bridge the gap between the time of injury and the time of professional clinical intervention.
The primary limitation of dental wax is its inability to create a hermetic (airtight and watertight) marginal seal. At a microscopic level, the interface between the tooth structure and the wax is highly porous. The oral cavity is a complex microbiome containing billions of bacteria, including cariogenic species like Streptococcus mutans. When wax is left on a tooth for extended periods, saliva carrying these bacteria seeps under the wax layer. The wax then acts as an incubator, trapping the bacteria directly against the exposed, vulnerable dentin. Because dentin is significantly less mineralized than enamel, bacterial acids can demineralize it rapidly, leading to aggressive secondary caries.[4]
“Dental wax is an excellent immediate palliative measure for acute trauma, but it lacks the marginal seal necessary to protect the dentinal tubules from bacterial invasion. Prolonged use without professional disinfection and sealing inevitably leads to microleakage and deep pulpal pathology.”
— Dr. Nguyen Van Cuong, Lead Clinician
Furthermore, if the fracture extends near the gingival margin, a bulky piece of wax can impinge on the biologic width of the periodontal tissues. Constant pressure and plaque accumulation at the gumline will quickly induce localized gingivitis, characterized by bleeding, swelling, and further discomfort. Therefore, patients must view wax strictly as a 24-to-48-hour solution.
Transitioning from Temporary Wax to Permanent Restorations
Definitive treatment for a chipped tooth involves replacing the lost structure through direct composite resin bonding, porcelain veneers, or full-coverage indirect restorations.
Once the patient arrives at the clinic, the temporary wax is removed, and a comprehensive diagnostic evaluation is performed. This includes vitality testing (cold tests and electric pulp testing) and periapical radiography to ensure the root and pulp are intact. Based on the extent of the missing tooth structure, the dentist will recommend a definitive restorative protocol.
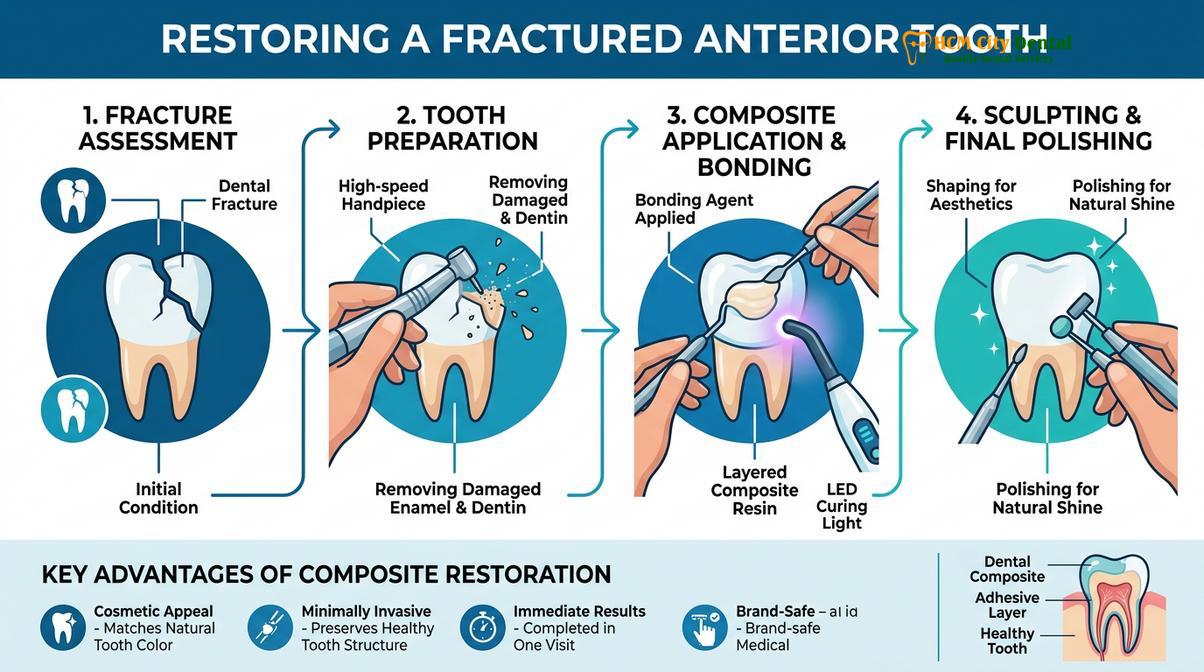
For minor to moderate enamel-dentin fractures (Ellis Class I and II), direct composite resin bonding is the standard of care. This highly conservative procedure involves isolating the tooth, etching the enamel and dentin with 37% phosphoric acid, and applying a bonding agent. The dentist then layers light-cured composite resin, sculpting it to match the exact anatomical contours and shade of the natural tooth. This process restores both the structural integrity and the aesthetic appearance of the tooth in a single visit.
If the fracture is extensive, involves a large portion of the incisal edge, or compromises the structural stability of the tooth, a more robust indirect restoration is required. In these cases, the dentist may recommend a full-coverage dental restorations, commonly referred to as a dental tooth cap. Preparing a tooth for a crown involves reducing the remaining structure to create a stable foundation. The clinician will then take a highly accurate digital or physical impression.
Modern dentistry offers various materials for these indirect restorations. For anterior teeth where aesthetics are paramount, comparing zirconia and porcelain materials is a standard part of the treatment planning process. Monolithic zirconia offers exceptional flexural strength, while layered porcelain provides superior optical translucency that mimics natural enamel. In cases where the fracture has exposed the pulp (Ellis Class III), endodontic therapy (root canal) must be completed before the final crown is cemented to ensure the tooth remains infection-free. Patients seeking advanced restorative dentistry can expect these permanent solutions to last for many years with proper oral hygiene.
Case Study: Managing an Acute Enamel Fracture
A clinical presentation of an acute incisor fracture demonstrates how immediate wax application prevents mucosal laceration prior to definitive composite restoration.
To illustrate the proper workflow from emergency trauma to definitive care, consider a recent clinical case managed at our facility.
Patient Presentation: A 28-year-old male patient contacted HCMC Dental Clinic in Ho Chi Minh City after sustaining trauma to his upper right central incisor (Tooth #11) from a sports-related impact. The patient reported no spontaneous pain but experienced severe sharpness against his lower lip and mild sensitivity to cold air. Unsure of what to do, he initially searched for a “super dentist near me” before contacting our emergency triage line.
Immediate Management: Over the phone, our clinical team instructed the patient to gently rinse the area, dry the tooth, and apply orthodontic dental wax over the jagged edge to protect his lip overnight. He was scheduled for the first available morning appointment.
Clinical Intervention: Upon presentation, the wax was removed. Clinical examination and radiographs confirmed an uncomplicated crown fracture (Ellis Class II) with no pulpal exposure or root fracture. Dr. Nguyen Van Cuong performed a direct composite restoration. The fractured margins were beveled to increase the surface area for bonding, and a highly aesthetic nano-hybrid composite was layered and polished. The patient left the clinic with full function and aesthetics restored, demonstrating the successful transition from emergency wax palliation to permanent clinical repair.
When to See a Doctor: Red Flags in Dental Trauma
While dental wax is a highly useful tool for managing minor chips, certain clinical signs indicate severe dental trauma that requires immediate, emergency intervention. Delaying care in the presence of these red flags can result in the loss of the tooth or the spread of severe odontogenic infection.
Patients must seek immediate professional evaluation if they observe any of the following symptoms after chipping a tooth:
- Visible Pink or Red Spot: If a small pink or bleeding spot is visible in the center of the fractured dentin, this indicates a direct pulpal exposure. The nerve is open to the oral environment, and endodontic therapy is required immediately to save the tooth.
- Severe, Spontaneous Pain: Pain that occurs without any stimulus (like hot or cold) and throbs continuously suggests irreversible pulpitis or acute periapical inflammation.
- Tooth Mobility: If the chipped tooth feels loose or moves within the socket when touched, the trauma has likely damaged the periodontal ligament or fractured the alveolar bone.
- Displacement: If the tooth has been pushed backward, forward, or deeper into the gum line (luxation or intrusion), it requires immediate repositioning and splinting by a dentist.
“Any dental trauma resulting in a visible pink spot within the fracture line indicates direct pulpal exposure, necessitating immediate endodontic evaluation rather than palliative wax application. Time is of the essence in preserving pulp vitality.”[5]
— Clinical Guidelines on Dental Traumatology
If you have suffered a dental injury, do not rely on temporary measures indefinitely. A prompt clinical examination is essential to accurately diagnose the extent of the trauma and implement a definitive treatment plan, whether that involves simple bonding or managing a loose dental crown that may have been damaged during the impact.

Frequently Asked Questions
Can I eat or drink while wearing dental wax on a chipped tooth?
You should remove dental wax before eating or drinking to prevent accidental ingestion and dislodgment. Chewing forces and hot beverages will quickly melt or deform the wax, compromising its protective seal over the fractured enamel. Always reapply a fresh, clean piece of wax after you have finished your meal and gently brushed the area.
How long can I safely leave dental wax on a broken tooth?
Dental wax should only be used for a few days as a temporary emergency measure. Prolonged use without professional clinical evaluation increases the risk of bacterial accumulation, dentinal hypersensitivity, and progressive pulpal inflammation. It is a bridge to professional care, not a substitute for a permanent dental restoration.
Is it safe if I accidentally swallow orthodontic dental wax?
Yes, accidentally swallowing a small amount of dental wax is generally harmless. Medical-grade dental wax is non-toxic and formulated from natural substances like beeswax and paraffin, allowing it to pass safely through the digestive system without causing systemic toxicity or gastrointestinal blockages.
Will dental wax stop the pain from an exposed nerve?
Dental wax cannot effectively treat or stop the severe pain associated with an exposed dental nerve. While it may slightly reduce thermal sensitivity by covering dentin, true pulpal exposure requires immediate endodontic intervention by a dentist to remove the inflamed tissue and prevent severe infection.
Can I use regular candle wax instead of dental wax in an emergency?
You must never use candle wax or non-medical waxes in the oral cavity. These products contain toxic synthetic dyes, artificial fragrances, and unsafe chemicals that can cause severe mucosal irritation, allergic reactions, and systemic toxicity. Only use medical-grade orthodontic or dental wax designed specifically for intraoral use.
References
- Journal of Endodontics. Management of traumatic dental injuries and enamel-dentin fractures. (2021).
- Dental Materials. Thermoplastic properties and clinical efficacy of orthodontic and protective waxes. (2020).
- International Endodontic Journal. The hydrodynamic theory of dentinal hypersensitivity and barrier protection. (2019).
- American Association of Endodontists. Guidelines for the evaluation and treatment of traumatic dental injuries. (2022).
- Journal of Prosthetic Dentistry. Transitioning from provisional emergency care to definitive composite and ceramic restorations. (2018).



