When comparing enamel vs porcelain, enamel is the natural, highly mineralized outer layer of human teeth, while dental porcelain is a synthetic ceramic material used to restore damaged teeth. Both share similar optical properties, but porcelain offers superior stain resistance while natural enamel possesses unique self-healing remineralization capabilities.
Clinical Summary:
The clinical distinction between natural tooth enamel and dental porcelain is foundational to modern restorative dentistry. Enamel is a biological tissue composed primarily of hydroxyapatite crystals, offering dynamic protection for the underlying dentin. However, because it is acellular, it cannot regenerate once structurally compromised by decay, trauma, or severe erosion. In contrast, dental porcelain encompasses a range of engineered glass-ceramics designed to biomimetically replace lost tooth structure. While porcelain provides exceptional aesthetic fidelity and superior resistance to staining, its higher hardness requires precise occlusal management to prevent excessive wear on opposing natural teeth. Understanding these biomechanical differences guides clinicians in selecting the appropriate restorative materials, ensuring long-term functional stability and optimal aesthetic integration for the patient.
Key Takeaways:
- Natural enamel is composed of 96% inorganic minerals (hydroxyapatite) and cannot biologically regenerate once fractured or decayed.
- Dental porcelain is a synthetic glass-ceramic engineered to mimic the light-reflecting properties and strength of natural teeth.
- Porcelain is generally harder than natural enamel, necessitating careful bite adjustments to protect opposing natural dentition from wear.
- Unlike natural teeth, porcelain restorations are highly resistant to discoloration from dietary pigments and acids.
- Modern dentistry utilizes various ceramic systems, from traditional metal-fused crowns to advanced high-strength lithium disilicate, tailored to specific clinical needs.
Understanding the Core Differences: Enamel vs Porcelain
Natural tooth enamel provides dynamic biological protection through hydroxyapatite crystals, whereas dental porcelain is an inert, synthetic ceramic engineered to replicate enamel’s strength and aesthetics in clinical restorations.
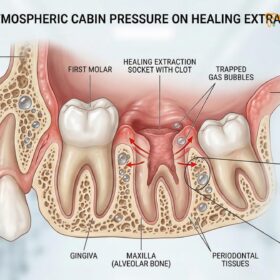
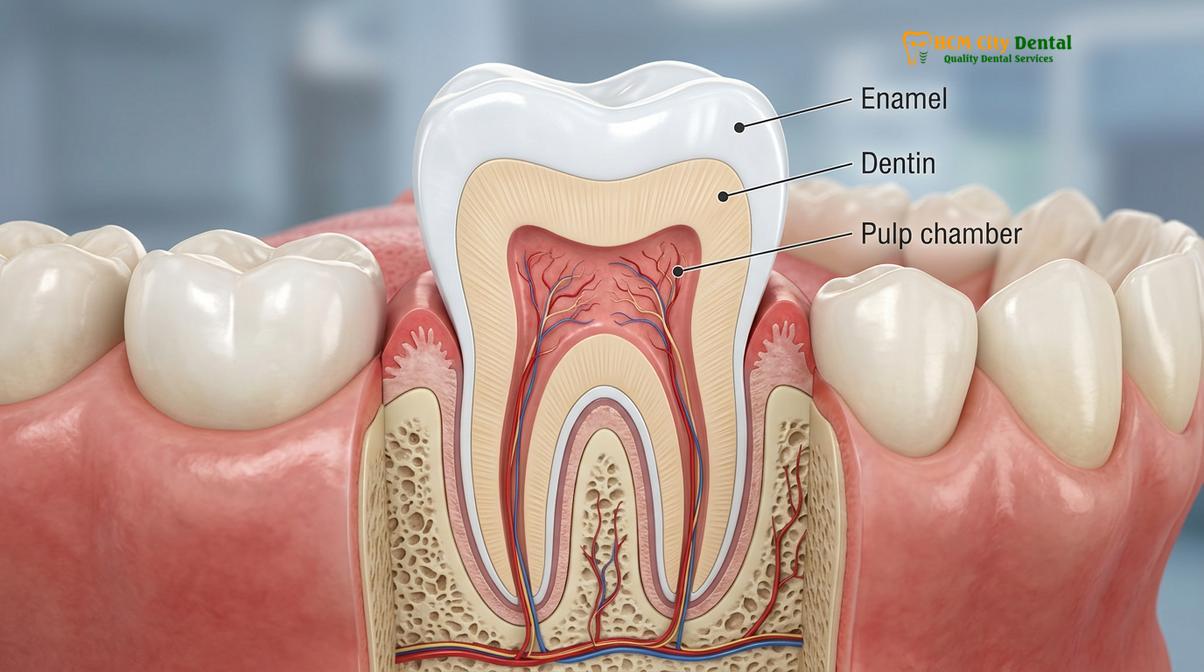
To fully grasp the nuances of restorative dentistry, one must first understand the fundamental differences between the biological tissues we are born with and the synthetic materials used to repair them. The comparison of enamel vs porcelain is essentially a study of nature versus advanced biomimetic engineering. Natural tooth enamel is the hardest substance in the human body. It is a highly mineralized tissue, consisting of approximately 96% inorganic hydroxyapatite crystals, with the remaining 4% composed of water and organic materials[1]. This unique crystalline structure gives enamel its remarkable ability to withstand the immense compressive forces of mastication (chewing) while protecting the sensitive dentin and pulp beneath.
However, enamel has a critical biological limitation: it is acellular. Because the ameloblast cells that form enamel are lost once the tooth erupts into the oral cavity, enamel cannot biologically regenerate or heal itself if it is fractured, severely decayed, or worn away. While minor surface demineralization can be reversed through fluoride uptake from saliva and toothpaste, structural loss is permanent. This is where the field of General Dentistry steps in, utilizing synthetic materials to restore form and function.

When patients ask about the porcelain meaning in a dental context, they are referring to a specific class of dental ceramics. Dental porcelain is an inert, glass-like material primarily composed of feldspar, quartz, and kaolin, which is fired (sintered) at high temperatures to create a hard, durable restoration. It is designed to closely mimic the translucency, hue, and chroma of natural enamel. It is important to distinguish this from the term porcelain enamel, which is frequently used in industrial applications to describe a glass coating fused to metal substrates (like cookware or appliances). In dentistry, while we do fuse porcelain to metal frameworks, the goal is always biomimetic—to replace lost biological enamel with a synthetic equivalent that functions seamlessly within the stomatognathic system.
Dr. Nguyen Van Cuong, a leading restorative specialist, frequently emphasizes to his patients that while we cannot regrow natural enamel, modern dental porcelains allow us to restore a tooth to its original strength and beauty with remarkable precision. The goal is not just to fill a hole, but to recreate the biomechanical harmony of the natural tooth.
Biomechanical Properties and Clinical Performance
While dental porcelain is harder and more stain-resistant than natural enamel, it lacks the biological ability to remineralize, making precise occlusal adjustments critical to prevent wear on opposing teeth.
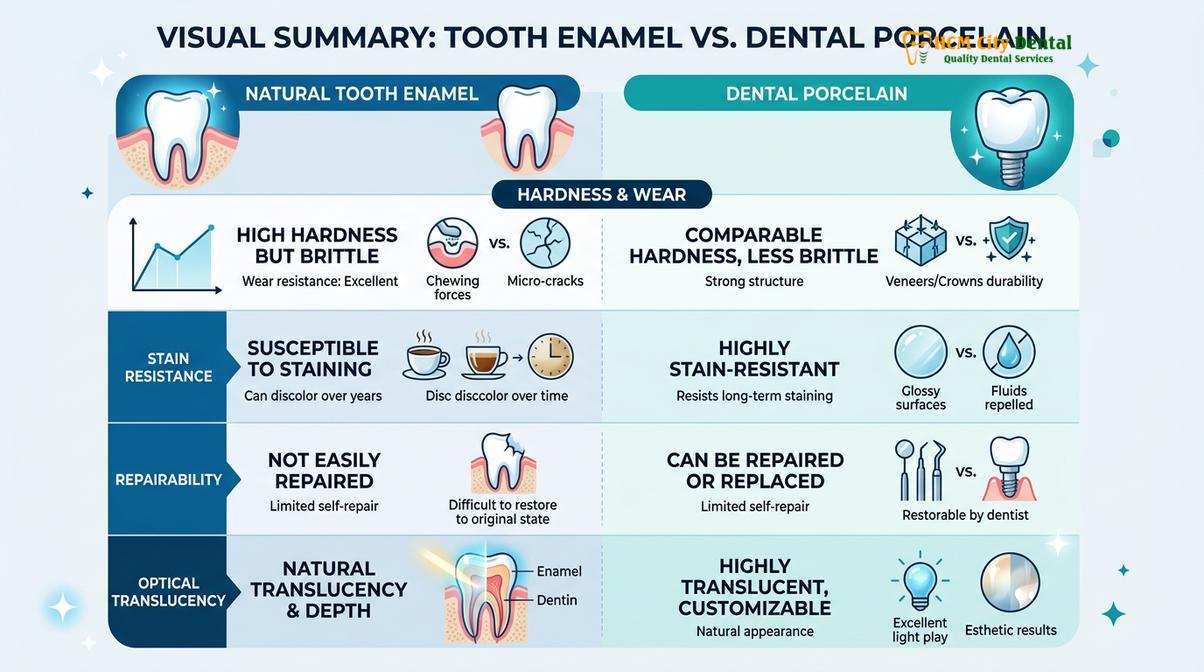
The clinical success of any dental restoration depends heavily on how its biomechanical properties interact with the surrounding natural tissues. When evaluating enamel vs porcelain, clinicians look closely at hardness, fracture toughness, wear resistance, and optical behavior. Natural enamel has a Vickers Hardness Number (VHN) of approximately 300 to 400. It is incredibly hard but also somewhat brittle. Its strength is derived from the resilient dentin layer beneath it, which acts as a shock absorber during chewing[2].
Dental porcelains, depending on their specific composition, often exceed the hardness of natural enamel. Traditional feldspathic porcelains have a VHN of around 400 to 500, while advanced ceramics like lithium disilicate or zirconia can reach VHNs of 1000 or more. This high hardness makes porcelain exceptionally durable and resistant to wear. However, this clinical advantage comes with a caveat: if a highly abrasive porcelain surface is placed against natural enamel, it can cause accelerated wear of the opposing natural tooth over time. Therefore, achieving a highly polished surface and ensuring perfect occlusal (bite) alignment is paramount during the delivery of a porcelain restoration.
Another significant difference lies in their response to the oral environment. Natural enamel is susceptible to acid erosion. Frequent consumption of acidic foods and beverages can lower the pH of the mouth, leading to demineralization (a topic explored deeply in our clinical analysis of how dietary acids affect teeth). Furthermore, enamel is slightly porous, allowing pigments from coffee, tea, and tobacco to cause intrinsic staining over time. Dental porcelain, conversely, is completely non-porous once glazed. It is impervious to acid erosion and highly resistant to staining, ensuring that the restoration maintains its original shade indefinitely.
| Property | Natural Tooth Enamel | Dental Porcelain (Ceramic) |
|---|---|---|
| Composition | 96% Hydroxyapatite (Biological) | Glass-ceramics, Feldspar, Zirconia (Synthetic) |
| Regeneration | Capable of micro-remineralization only | Inert; cannot heal, requires physical repair |
| Stain Resistance | Moderate (porous, absorbs pigments) | Excellent (non-porous, glazed surface) |
| Hardness (Vickers) | ~300 – 400 VHN | ~400 – 1000+ VHN (varies by type) |
| Acid Resistance | Vulnerable to pH drops below 5.5 | Highly resistant to dietary acids |
“The ultimate goal of restorative dentistry is to select a material that not only replaces missing tooth structure but also respects the biomechanical limits of the opposing natural dentition. Porcelain offers unparalleled aesthetics, but its hardness demands absolute precision in occlusal management.”
— Journal of Prosthetic Dentistry
Types of Dental Porcelain Restorations
Modern restorative dentistry utilizes various ceramic systems, ranging from traditional metal-based crowns to advanced high-strength glass ceramics, tailored to the functional and aesthetic demands of each tooth.
When a patient asks, “what is a porcelain crown?”, the answer is multifaceted because “porcelain” is an umbrella term covering several distinct restorative systems. The choice of material depends on the location of the tooth, the functional load it must bear, and the aesthetic expectations of the patient. For decades, the gold standard in restorative dentistry was the pfm porcelain fused metal crown. This restoration consists of a strong metal alloy core over which layers of tooth-colored feldspathic porcelain are baked. While highly durable and excellent for posterior (back) teeth, PFM crowns have aesthetic limitations; the underlying metal can sometimes cast a dark shadow at the gum line, making them less ideal for highly visible areas.
As aesthetic demands have evolved, so has dental materials science. Today, clinicians frequently utilize all-ceramic systems. For instance, emax porcelain crowns (made of lithium disilicate) are renowned for their exceptional translucency and lifelike vitality. Because they do not contain a metal core, light can pass through them much like it does through natural enamel, making them the premier choice for porcelain crowns front teeth. They provide a seamless integration with the surrounding natural dentition, often making it impossible to distinguish the restoration from a natural tooth[3].

For patients requiring maximum strength—such as those who grind their teeth (bruxism) or need long-span dental bridges—a porcelain fused to zirconia crown offers an optimal hybrid solution. Zirconia is a white crystalline oxide of zirconium, known as “ceramic steel” due to its immense fracture toughness. By milling a core out of zirconia and layering aesthetic porcelain on top, clinicians can achieve both the structural integrity needed for heavy chewing forces and the beautiful aesthetics required for a natural smile. This approach is frequently utilized when replacing extracted teeth with implant-supported restorations.
It is also worth noting the distinction between porcelain and composite resin. While porcelain resin hybrid materials and composite bonding are excellent for conservative repairs, they do not possess the same long-term durability or stain resistance as laboratory-fabricated porcelain. Resin composites are applied directly to the tooth and cured in a single visit, whereas porcelain restorations require meticulous laboratory fabrication.
The Clinical Workflow: Restoring Lost Enamel
The transition from damaged natural enamel to a definitive ceramic restoration requires meticulous tooth preparation, precise digital impressions, and specialized adhesive bonding protocols to ensure long-term success.
The process of replacing damaged enamel with a porcelain restoration is a highly technical workflow that requires precision at every step. The journey begins with a comprehensive clinical assessment. Dr. Nguyen Van Cuong notes that successful restorative outcomes rely heavily on accurate diagnostics, ensuring that the underlying tooth structure is healthy enough to support a restoration. If a tooth is severely compromised, foundational treatments such as core build-ups or endodontic therapy may be required before the crown phase begins.
The next critical phase is tooth preparation. The porcelain fused to metal crown preparation differs slightly from an all-ceramic preparation. For a PFM crown, the dentist must remove enough tooth structure to accommodate both the metal substructure and the overlying porcelain (typically 1.5 to 2.0 millimeters of reduction). For high-strength all-ceramic crowns like monolithic zirconia, more conservative preparations are often possible. The clinician carefully shapes the tooth, creating specific margin designs (such as a chamfer or modified shoulder) to ensure the final crown seats perfectly without creating ledges that could harbor plaque[4].
Once the tooth is prepared, highly accurate impressions are taken. At modern facilities like HCMC Dental Clinic in Ho Chi Minh City, traditional messy putty impressions have largely been replaced by digital intraoral scanners. These scanners capture a 3D topographical map of the prepared tooth and the surrounding dentition, which is then transmitted instantly to the dental laboratory. While the permanent porcelain restoration is being custom-crafted by master ceramists, the patient is fitted with a temporary crown to protect the exposed dentin and maintain gingival health.
“The longevity of a ceramic restoration is inextricably linked to the quality of the marginal seal. Meticulous isolation and strict adherence to adhesive bonding protocols are non-negotiable for preventing microleakage and secondary caries.”
— International Journal of Periodontics & Restorative Dentistry
The final delivery involves specialized bonding protocols. Unlike traditional cements that merely fill the space between the tooth and the crown, modern adhesive dentistry creates a micromechanical and chemical bond. The internal surface of the porcelain is often treated with hydrofluoric acid and a silane coupling agent, while the natural tooth is etched with phosphoric acid. A dual-cure resin cement is then used to fuse the synthetic porcelain to the biological tooth structure, creating a unified, structurally sound complex.
Aesthetic Outcomes, Costs, and Patient Expectations
Achieving a seamless integration between artificial porcelain and natural dentition depends on material selection, the technician’s skill, and a comprehensive understanding of the patient’s aesthetic goals and budget.
For many patients, the primary motivation for choosing porcelain over other restorative materials is aesthetics. The ability of dental porcelain to mimic the light-scattering properties, surface texture, and subtle color gradients of natural enamel is unparalleled. When reviewing porcelain crowns before and after clinical photographs, patients are often amazed at how a dark, heavily restored, or fractured tooth can be transformed into a vibrant, natural-looking component of their smile.
Achieving this level of realism requires a deep understanding of color science. A tooth is not simply “white.” It has a specific hue (the basic color), chroma (the intensity of the color), and value (the brightness). Furthermore, natural teeth exhibit varying degrees of translucency, particularly at the incisal edges (the biting surface of front teeth), where there is no underlying opaque dentin. Master ceramists meticulously layer different shades and opacities of porcelain to recreate these complex optical phenomena[5].
Clinical Case Review: Anterior Aesthetic Restoration
A patient presented to HCMC Dental Clinic in Saigon with a fractured central incisor following a sports injury. The natural enamel was severely compromised, exposing the underlying dentin. After a thorough evaluation, an E.max lithium disilicate crown was selected for its superior optical properties. By utilizing digital shade matching and custom laboratory layering, the final restoration seamlessly blended with the adjacent natural teeth, restoring both the patient’s bite function and their confident smile.

When discussing the porcelain crowns price, it is important to understand that the cost reflects not just the raw materials, but the extensive clinical expertise, digital technology, and laboratory artistry required to produce a custom medical device. While composite resin bonding may have a lower initial cost, porcelain restorations offer significantly greater longevity and resistance to wear and staining, often making them a more cost-effective investment over the long term. Patients seeking comprehensive care and transparent treatment planning often consult our comprehensive guide to dental procedures to understand the value of premium restorative materials.
When to See a Doctor for Enamel Restoration
Because natural enamel cannot regenerate, it is crucial to seek professional dental care at the first sign of structural damage. Ignoring early signs of enamel wear or decay can lead to more complex and invasive treatments down the line. You should schedule a clinical evaluation if you experience any of the following symptoms:
- Visible Cracks or Chips: Any physical fracture in the tooth compromises the protective enamel layer, exposing the vulnerable dentin to bacteria and increasing the risk of infection.
- Severe Tooth Sensitivity: A sharp, lingering pain when consuming hot, cold, or sweet foods often indicates that the enamel has worn thin, exposing the microscopic tubules within the dentin.
- Yellowing or Discoloration: While some staining is superficial, significant yellowing can indicate that the white enamel has eroded away, revealing the naturally yellow dentin underneath.
- Changes in Bite Alignment: If you notice your teeth fitting together differently, it may be a sign of severe occlusal wear, often caused by nocturnal teeth grinding (bruxism). This condition can rapidly destroy natural enamel and requires intervention, potentially involving arch evaluation and protective night guards.
Important Clinical Consideration
Over-the-counter dental repair kits or aggressive whitening treatments cannot restore lost enamel and may cause irreversible damage to the tooth pulp. If you suspect your enamel is compromised, a professional radiographic and clinical examination is mandatory to determine the appropriate restorative protocol.
At HCMC Dental Clinic, our approach to restorative dentistry is rooted in biomimetic principles—preserving as much natural tooth structure as possible while utilizing the most advanced ceramic materials available. Whether you require a single conservative veneer or a complex full-mouth rehabilitation, our clinical team is dedicated to providing evidence-based care tailored to your unique anatomical needs. For expats and locals alike seeking top-tier restorative care, comparing options is essential; you can review our insights on the standards of care in District 1 or explore our Thao Dien clinic guide to find the right environment for your treatment.
Frequently Asked Questions
Is dental porcelain stronger than natural tooth enamel?
Yes, most dental porcelains are harder than natural enamel. While enamel has a Vickers hardness of around 300-400, modern dental ceramics and porcelains often exceed this, making them highly durable but requiring careful occlusal adjustment to prevent wearing down opposing natural teeth.
Because of this extreme hardness, clinicians must ensure that the bite is perfectly balanced. If a high spot is left on a porcelain crown, the repetitive force of chewing can cause the opposing natural tooth to wear down prematurely or even fracture.
Can natural enamel be rebuilt instead of using a porcelain crown?
Minor enamel demineralization can be reversed through fluoride treatments, but significant structural loss cannot regenerate. Once enamel is fractured or severely decayed, synthetic materials like composite resin or porcelain restorations are clinically required to restore the tooth’s function and integrity.
Unlike bone or skin, enamel does not contain living cells once the tooth has erupted. Therefore, the concept of “regrowing” enamel is currently biologically impossible, making advanced restorative materials the only viable solution for structural repair.
Do porcelain restorations stain like natural enamel?
No, dental porcelain is highly resistant to staining compared to natural enamel. Because porcelain is a non-porous, glazed ceramic, pigments from coffee, tea, or tobacco cannot easily penetrate its surface, allowing it to maintain its original shade much longer than natural teeth.
However, it is important to note that while the porcelain itself will not stain, the margins where the crown meets the natural tooth root, or the resin cement used to bond the crown, can accumulate plaque and stains if meticulous oral hygiene is not maintained.
How long does a porcelain crown typically last?
A well-maintained porcelain crown can last between 10 to 15 years, and often much longer. Longevity depends heavily on the patient’s oral hygiene, occlusal forces (such as teeth grinding), the specific ceramic material used, and the precision of the initial clinical bonding protocol.
Routine dental check-ups and professional cleanings are essential to monitor the integrity of the crown margins. Patients who suffer from bruxism are often advised to wear a protective occlusal guard at night to prevent excessive stress on the ceramic material.
What is the difference between composite resin and dental porcelain?
Composite resin is a plastic-based material applied directly to the tooth and cured, while porcelain is a glass-ceramic fabricated in a laboratory. Porcelain offers superior aesthetics, greater longevity, and higher stain resistance, whereas composite is more affordable and easier to repair if chipped.
Composite restorations are excellent for small to moderate cavities or minor aesthetic bonding. However, for large structural defects or areas subjected to heavy chewing forces, laboratory-fabricated porcelain remains the superior clinical choice due to its biomechanical stability.
References
- Journal of Prosthetic Dentistry. Biomechanical properties of natural enamel versus dental ceramics. (2021).
- Dental Materials Journal. Wear behavior of human enamel opposing different ceramic restorations. (2020).
- International Journal of Periodontics & Restorative Dentistry. Biomimetic approaches in restorative dentistry. (2019).
- Journal of the American Dental Association. Clinical longevity of porcelain fused to metal and all-ceramic crowns. (2022).
- Clinical Oral Investigations. Optical properties and shade matching of lithium disilicate ceramics. (2018).