Daily Oral Hygiene Guide: Best Practices for Brushing & Flossing

Master your daily oral hygiene guide at HCMC Dental Clinic. Dr. Cuong explains correct brushing and flossing techniques for healthy teeth. Free consultation.
True oral health extends far beyond having white teeth; it is rooted in maintaining a balanced oral microbiome and mastering the daily mechanical disruption of dental plaque. Improper brushing and flossing techniques are the leading causes of preventable dental diseases, including caries (cavities), gingivitis, and severe periodontitis. This guide provides an evidence-based masterclass in daily oral hygiene protocols, shifting the focus from simply “cleaning teeth” to actively managing oral biology.
1. Introduction: The Oral Microbiome
The human mouth is one of the most complex microbial ecosystems in the body, hosting over 700 distinct species of bacteria, fungi, and viruses. This ecosystem, known as the oral microbiome, is not inherently harmful. In fact, many resident bacteria are commensal or beneficial—they help pre-digest food, synthesize essential vitamins, and actively defend the mouth against external, highly virulent pathogens.
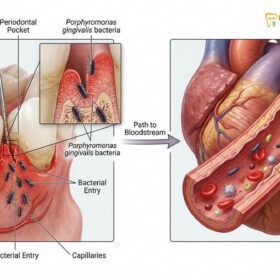
Oral diseases occur when there is an ecological shift, known as “dysbiosis.” This shift is typically triggered by a high-sugar diet, inadequate salivary flow (dry mouth), or poor mechanical hygiene. When dysbiosis occurs, aciduric (acid-loving) bacteria like Streptococcus mutans multiply rapidly, leading to enamel demineralization (cavities). Simultaneously, anaerobic bacteria like Porphyromonas gingivalis thrive below the gumline, triggering the inflammatory cascade of periodontal disease. The primary goal of daily oral hygiene is not to sterilize the mouth, but to manage the biofilm and maintain a healthy, balanced microbiome.
2. Plaque & Calculus: The Biological Mechanisms
The progression from a clean tooth to severe dental disease is driven by the maturation of the dental biofilm.
The Formation of the Pellicle and Biofilm
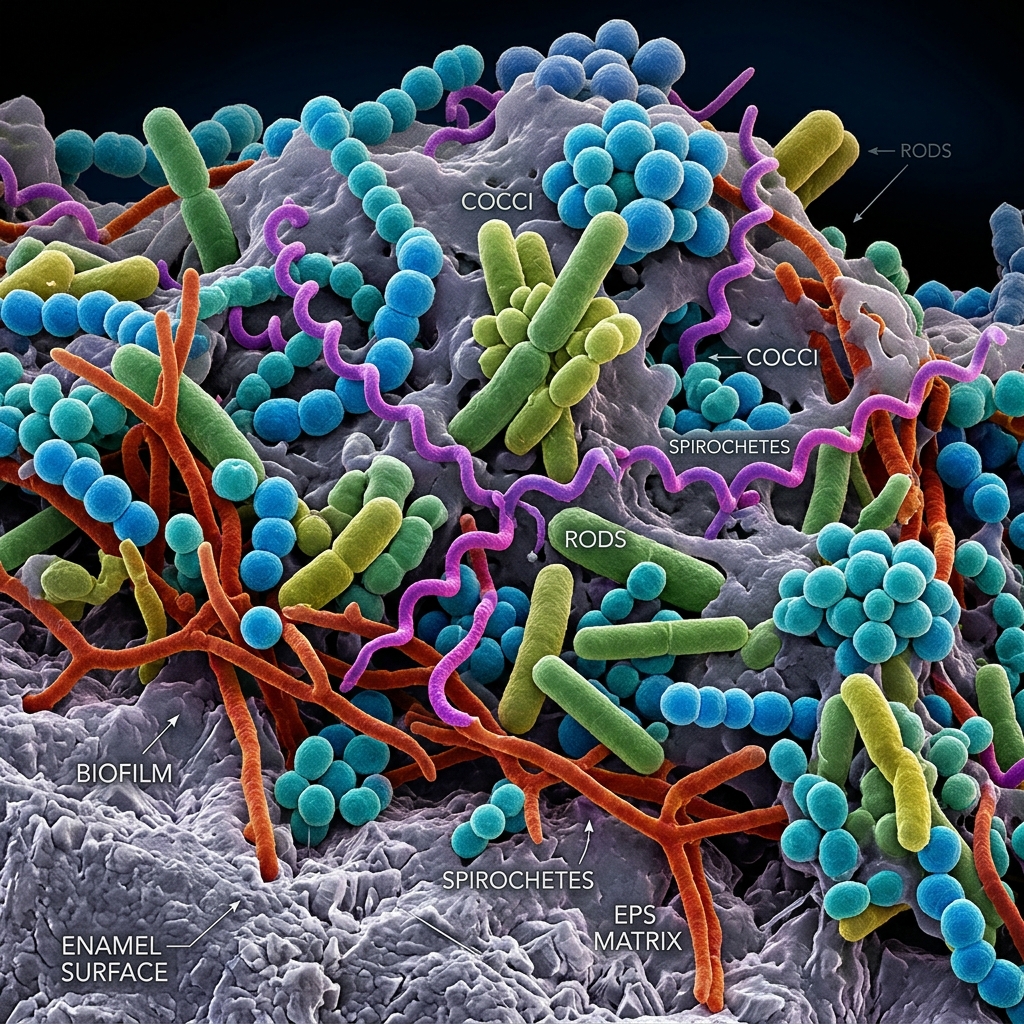
Within minutes of brushing your teeth, salivary proteins naturally coat the clean enamel, forming a microscopic layer called the “acquired pellicle.” This pellicle acts like double-sided tape. Within hours, pioneer bacteria attach to this layer and begin multiplying, creating a sticky, pale-yellow matrix known as dental plaque (biofilm).
In its early stages (0-24 hours), plaque is soft, loosely attached, and highly susceptible to disruption by a toothbrush or floss. However, if left undisturbed for 48 to 72 hours, the biofilm matures. The bacterial colonies organize into complex architectural structures, building protective extracellular slime layers that make them highly resistant to antibacterial mouthwashes.

Calculus (Tartar) Formation
As the biofilm ages, it begins to absorb calcium and phosphate ions naturally present in your saliva and gingival crevicular fluid. This mineralization process hardens the soft plaque into dental calculus (tartar). Calculus is rock-hard and bonds aggressively to the microscopic irregularities of the tooth enamel and root cementum. Once calculus has formed, it is impossible to remove with home care tools; it requires professional ultrasonic scaling.
3. Brushing Masterclass: Methods & Tools
Most individuals brush their teeth every day, yet many still suffer from cavities and gum disease. The discrepancy lies entirely in the technique. A quick, aggressive scrubbing motion across the chewing surfaces completely misses the critical zones where disease begins: the gumline and the interproximal spaces.
3.1. The Modified Bass Method
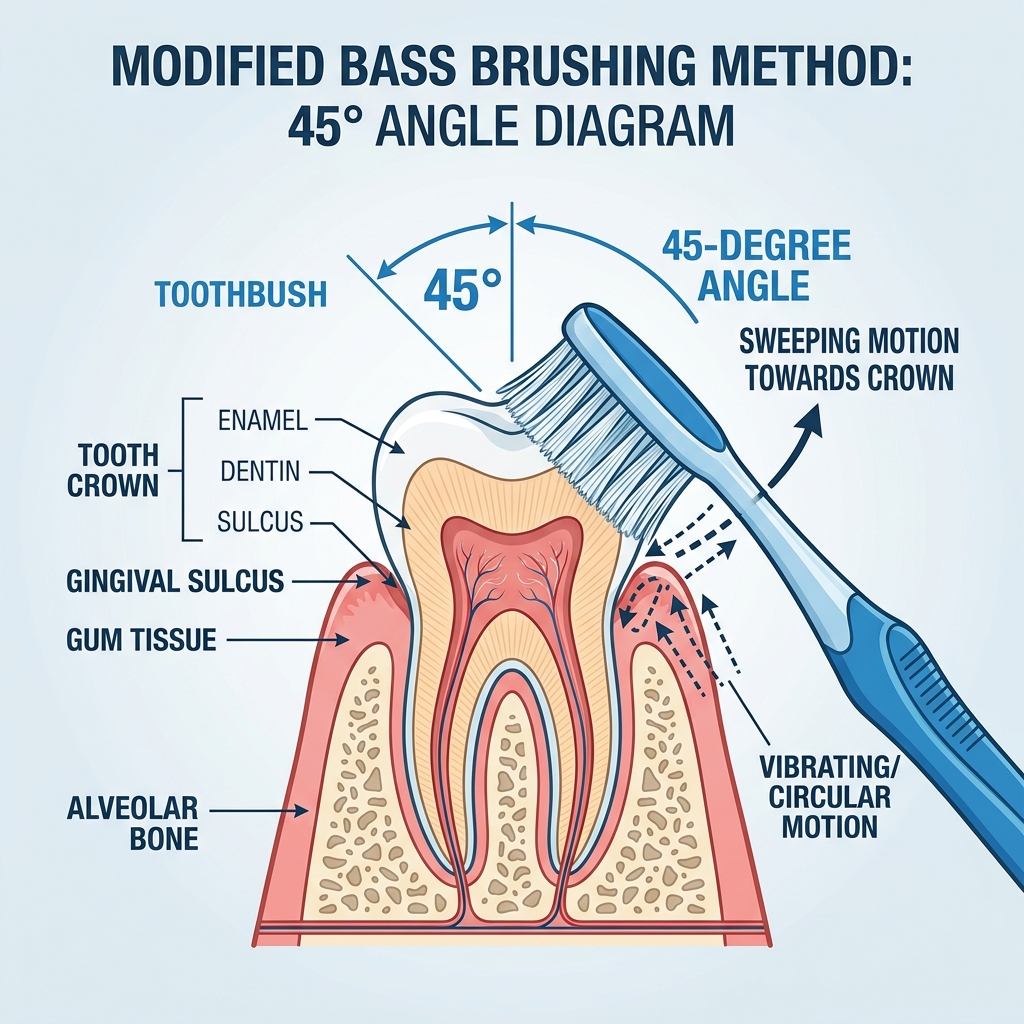
The Modified Bass Method is universally recognized by periodontists as the most effective manual brushing technique. Its primary objective is to clean the gingival sulcus—the shallow crevice between the tooth and the gum.
- The Angle: Hold a soft-bristled toothbrush so the bristles are angled at exactly 45 degrees toward the gumline.
- The Motion: Apply very gentle pressure so the bristles slightly enter the sulcus. Use tiny, rapid vibratory or circular motions in place for 10-15 seconds per area. Do not scrub back and forth, as this causes gum recession and enamel abrasion (toothbrush abrasion).
- The Sweep: After vibrating the bristles at the gumline, employ a sweeping motion (the “modified” aspect) to drag the bristles away from the gums toward the chewing surface of the tooth.
- Duration: A thorough cleaning requires a full two minutes.
3.2. Electric vs. Manual Brushing
While a manual toothbrush can be highly effective when used with perfect technique, electric toothbrushes offer a significant clinical advantage by removing the variable of human error. They deliver thousands of micro-movements per minute compared to the few hundred achievable by hand.
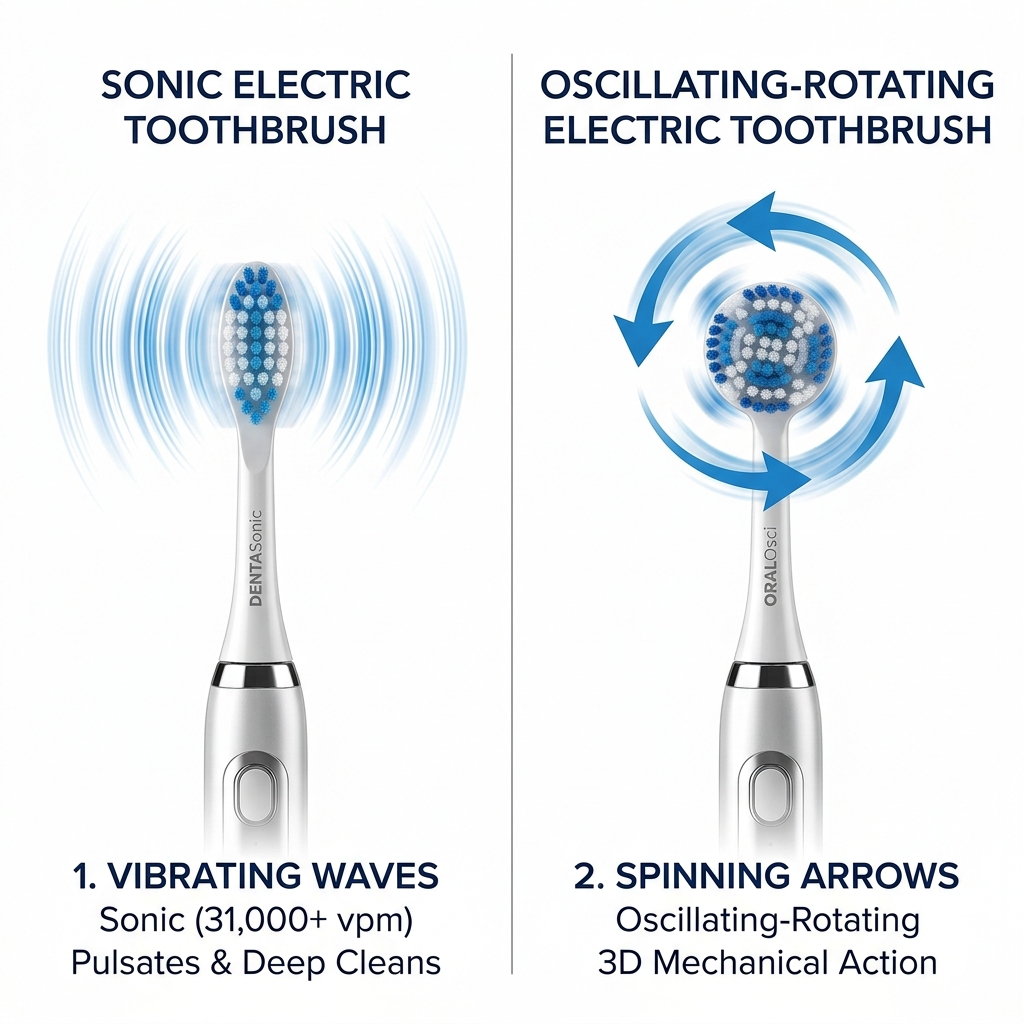
- Oscillating-Rotating (e.g., Oral-B): These feature small, round heads that cup each tooth, oscillating back and forth while pulsating to break up the biofilm. Clinical studies consistently show they are marginally superior at plaque removal compared to manual brushes.
- Sonic (e.g., Philips Sonicare): These vibrate at ultra-high speeds (up to 62,000 movements per minute). This rapid vibration creates “fluid dynamics”—microbubbles that are forcefully driven deep between teeth and below the gumline to disrupt bacteria beyond where the physical bristles reach.
3.3. The Role of Saliva in Oral Biology
Many patients overlook the biological significance of saliva, viewing it merely as a lubricant. In reality, saliva is your mouth’s most powerful natural defense mechanism. It is a highly complex bio-fluid containing 99% water and a 1% concentration of electrolytes, immunoglobulins, and proteins.
Salivary Protective Mechanisms:
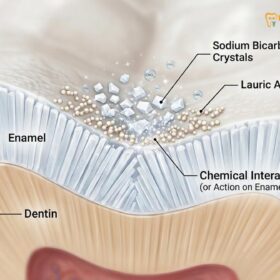
- Acid Buffering: Saliva contains high levels of bicarbonate and phosphate ions. When bacteria ferment food sugars and release cavity-causing acids, these chemical buffers neutralize the acid, rapidly raising the oral pH back toward a safe, neutral level (above 6.5) to halt enamel demineralization.
- Enamel Remineralization: Saliva is naturally supersaturated with calcium and phosphate ions. When the oral pH neutralizes, saliva actively deposits these minerals back into the porous enamel matrix, reversing early microscopic decay.
- Immunological Defense: Saliva contains secretory IgA antibodies, lysozymes, and lactoferrin. These proteins actively inhibit bacterial cell wall synthesis, prevent bacterial aggregation, and restrict iron availability, starving pathogenic strains.
Patients suffering from dry mouth (xerostomia)—often caused by prescription medications, salivary gland pathology, or chronic mouth breathing—lack these critical defenses. Without the continuous flushing and buffering action of saliva, plaque accumulates rapidly, and cavities can spread across the teeth within a matter of months, necessitating aggressive clinical interventions like custom fluoride trays.
4. Flossing & Interdental Protocols
A toothbrush, no matter how advanced, cannot clean the contact points where teeth touch, nor can it effectively reach into the interproximal sulcus. Skipping interdental cleaning leaves roughly 35% of the tooth surface completely uncleaned, which is why the vast majority of cavities and periodontal pockets develop between the teeth.

Fig 5. Interdental Arsenal: Traditional string floss, water flossers, and various sizes of interdental brushes.
4.1. String Floss & Water Flossing
- The C-Shape String Floss Technique: Simply snapping the floss straight down between the teeth is ineffective and can traumatize the interdental papilla (the triangle of gum between teeth). Proper technique requires curving the floss into a tight “C” shape around the side of the tooth, sliding it gently below the gumline, and wiping up and down 3-4 times. You must repeat this for the adjacent tooth before removing the floss.
- Water Flossers (Oral Irrigators): Devices like a Waterpik use a pulsating stream of pressurized water to flush out loose plaque and food debris from deep pockets (up to 6mm deep). While highly recommended as an adjunct—especially for patients with dental implants, bridges, or braces—they do not replace the mechanical wiping action of string floss or interdental brushes against sticky biofilm.
4.2. Selecting and Using Interdental Brushes
For patients with slight gum recession, wide interdental spaces, periodontal disease history, orthodontic appliances, or dental implants, interdental brushes (e.g., TeTe or Curaprox) are clinically superior to string floss. String floss is designed for tight contacts, but fails to clean the concave surfaces of teeth roots in wider spaces, leaving biofilm behind. Interdental brushes use tiny, soft bristles wrapped around a central wire to act like a bottle brush, scrubbing these concave root recesses clean.
Selecting the correct size is critical. Using a brush that is too small will not clean effectively, while forcing a brush that is too large can scratch the root surface and traumatize the gingival papilla. Clinicians utilize the ISO Standard Sizing (ISO 0 to ISO 8), which matches brushes to the specific width of the interdental gap (passage hole diameter):
| ISO Size | Passage Hole Diameter (mm) | Common Color Code (TePe) | Clinical Indication / Best Fit |
|---|---|---|---|
| ISO 0 | 0.4 mm | Pink | Extremely tight spaces, healthy young gums, anterior teeth |
| ISO 1 | 0.45 mm | Orange | Very tight interdental contacts, general cleaning |
| ISO 2 | 0.5 mm | Red | Standard spaces between anterior/premolar teeth |
| ISO 3 | 0.6 mm | Blue | Mild gum recession, post-orthodontic spaces |
| ISO 4 | 0.7 mm | Yellow | Premolar and molar teeth, moderate gum recession |
| ISO 5 | 0.8 mm | Green | Wide molar gaps, under bridges, dental implants |
| ISO 6+ | 0.9 mm to 2.2 mm | Purple / Grey / Black | Severe gum recession, “black triangles”, orthodontic brackets |
Correct Insertion Technique:
- Choose the appropriate ISO size. Most patients require 2-3 different sizes for different areas of their mouth.
- Hold the handle between your thumb and index finger. Align the brush head at a 90-degree angle to the axis of the teeth.
- Gently insert the tip at the base of the teeth (where the gum triangle sits). Never force the brush. If you feel hard resistance, step down to a smaller ISO size.
- For lower teeth, angle the brush slightly upwards; for upper teeth, angle it slightly downwards. Gently push the brush completely through the space until the bristles emerge on the tongue/lingual side.
- Pull the brush back out. Do this 2-3 times per interdental space. Do not use toothpaste on the interdental brush unless specifically prescribed.
- Rinse the brush bristles under running water after cleaning each tooth gap, and replace the brush weekly or when the bristles splay.
5. Chemical Agents: Toothpaste & Mouthwash Science
Mechanical disruption is the primary weapon against plaque, but chemical agents in toothpastes (dentifrices) and mouthwashes provide critical therapeutic benefits, particularly for enamel remineralization and anti-inflammatory action.
5.1. Fluoride vs. Nano-hydroxyapatite (nHAp)
Every time you consume fermentable carbohydrates, the bacteria in your plaque produce acid. This acid leaches calcium and phosphate out of your enamel, a process called demineralization. To prevent cavities, the enamel must be constantly remineralized.
Two primary active agents are utilized in modern dentistry to drive remineralization: Fluoride and Nano-hydroxyapatite (nHAp).
Fluoride acts by diffusing into the dental biofilm and tooth surface. When bacteria produce acids, the presence of Fluoride causes calcium and phosphate ions to co-precipitate, forming Fluorapatite [Ca10(PO4)6F2] instead of natural hydroxyapatite. Fluorapatite has a highly stable crystalline structure that is much harder and more acid-resistant. While natural enamel starts dissolving at a critical pH of 5.5, Fluorapatite remains stable down to a highly acidic pH of 4.5. This makes the tooth surface highly resistant to future acid attacks.
Nano-hydroxyapatite (nHAp) is a synthetic mineral compound that is chemically identical to natural hydroxyapatite, which constitutes 97% of human tooth enamel. Because nHAp particles are synthesized at the nanoscale (typically 20-50 nm), they have a high surface-area-to-volume ratio, allowing them to bind directly to demineralized enamel pores and open dentinal tubules. Instead of relying on saliva to supply minerals, nHAp acts as a direct, bio-compatible filler. It deposits a new layer of synthetic enamel to seal exposed dentinal tubules, providing rapid and profound relief for dentin hypersensitivity, while restoring the natural smooth luster of the teeth.
| Feature / Property | Fluoride (Sodium/Stannous Fluoride) | Nano-hydroxyapatite (nHAp) | Clinical Takeaway |
|---|---|---|---|
| Chemical Formula | Fluoride Ion (F-) | Calcium Phosphate Crystal [Ca10(PO4)6(OH)2] | Fluoride alters minerals; nHAp supplies natural minerals. |
| Mechanism of Action | Catalyzes saliva minerals to form Fluorapatite | Directly binds and deposits mineral crystals in micro-cracks | Fluoride is catalytic; nHAp is a direct biomimetic filler. |
| Critical pH Threshold | pH 4.5 (Highly acid resistant) | pH 5.5 (Standard enamel resistance) | Fluoride-formed enamel is harder and resists acid better. |
| Sensitivity Relief | Indirect (gradual mineral buildup) | Direct occlusion (seals dentin tubules immediately) | nHAp is significantly faster at stopping tooth sensitivity. |
| Toxicity Profile | Risk of Fluorosis if swallowed (toxic in high doses) | 100% Non-toxic, biocompatible, safe to swallow | nHAp is ideal for children, pregnant women, and fluoride-free preferences. |
| Aesthetic Benefit | None (prevents decay only) | Restores enamel smoothness, white luster, and gloss | nHAp provides mild biomimetic whitening and smooth texture. |

Fig 6. Enamel Remineralization: Fluoride recruits salivary minerals to construct Fluorapatite, while nHAp directly fills microscopic enamel pores.
5.2. Active Mouthwash Ingredients
Cosmetic mouthwashes merely mask bad breath. Therapeutic mouthwashes contain active ingredients designed to manage the microbiome.
- Chlorhexidine Gluconate (0.12%): A prescription-strength, broad-spectrum antiseptic. It is highly substantive, meaning it binds to oral tissues and slowly releases over 12 hours. It is prescribed strictly for short-term use (1-2 weeks) after oral surgery or for acute gingivitis, as long-term use can cause significant tooth staining and alter taste perception.
- Essential Oils (e.g., Listerine): Formulations containing thymol, eucalyptol, menthol, and methyl salicylate have proven efficacy in penetrating the plaque biofilm and reducing gingival inflammation without the staining side effects of chlorhexidine.
- Cetylpyridinium Chloride (CPC): An antimicrobial agent that interacts with the bacterial cell membrane, causing it to rupture. It is effective in reducing plaque and gingivitis and is commonly found in alcohol-free mouthwashes, making it ideal for patients with dry mouth (xerostomia).
5.3. Alcohol-Free Mouthwash vs. Alcohol-Containing Formulations
When selecting a mouthwash, the presence of alcohol (usually ethanol, added as a solvent for active ingredients) is a major clinical variable. Historically, most mouthwashes contained up to 20% alcohol. Modern clinical guidelines, however, heavily favor alcohol-free formulations for the following reasons:
- Mucosal Dehydration: Alcohol is a powerful drying agent. It dehydrates the oral mucosa, reducing salivary flow. As detailed in Section 3.3, a drop in saliva compromises the mouth’s natural defense, promoting dysbiosis and actually worsening chronic bad breath (halitosis) once the temporary mint flavor fades.
- Mucosal Irritation & Ulceration: Alcohol-based mouthwashes cause a burning sensation during swishing. This chemical irritation can damage sensitive tissues, exacerbate aphthous ulcers (canker sores), and lead to sloughing of the oral epithelium.
- Biocompatibility with Restorations: Chronic exposure to high concentrations of ethanol can soften composite resin fillings and accelerate the dissolution of dental cements used for crowns and veneers.
At HCMC Dental, we recommend that patients utilize alcohol-free mouthwashes containing active CPC or essential oils for daily microbiome management, reserving alcohol-containing antiseptics strictly for targeted, short-term clinical indications.
6. Professional Scaling & Maintenance
Despite the most meticulous home care routine, everyone misses trace amounts of plaque. Given that plaque begins calcifying into immovable calculus within 48 hours, professional intervention is an unavoidable component of oral hygiene.
A standard prophylaxis (cleaning) appointment every 6 months is generally sufficient for individuals with a healthy periodontium. During this visit, a hygienist or dentist utilizes ultrasonic scalers to vibrate away supragingival (above the gumline) and subgingival calculus. The teeth are then polished using a mildly abrasive prophylaxis paste to remove extrinsic stains (from coffee, tea, or tobacco) and smooth the enamel surface, making it harder for new bacteria to attach.
Patients with a history of periodontal disease, however, require a “periodontal maintenance” schedule. Because aggressive periodontal pathogens can repopulate a deepened pocket in just 9 to 12 weeks, these patients must undergo professional debridement every 3 to 4 months to prevent the reactivation of bone-destroying inflammation.

7. Frequently Asked Questions (FAQ)
Should I brush before or after breakfast?
It is generally better to brush before breakfast. While you sleep, saliva production drops, allowing bacteria to multiply. Brushing immediately upon waking removes this bacterial load and coats the teeth in protective fluoride before the acid attack of breakfast. If you prefer brushing after eating, you must wait at least 30 minutes, especially if you consumed acidic items like orange juice or coffee, as brushing immediately can abrade the temporarily softened enamel.
Should I rinse with water after brushing my teeth?
No. “Spit, don’t rinse.” Rinsing with water immediately after brushing washes away the active ingredients (like fluoride or nHAp) in your toothpaste. To maximize remineralization, simply spit out the excess foam and allow the residual paste to remain on your teeth.
Is it better to floss before or after brushing?
Clinical consensus favors flossing before brushing. Flossing dislodges the plaque and debris from between the teeth, allowing the fluoride from your toothpaste to deeply penetrate the freshly cleaned interproximal spaces during brushing.
Can brushing too hard damage my teeth?
Yes. Aggressive horizontal scrubbing with a hard-bristled brush leads to “toothbrush abrasion”—the physical wearing away of the protective enamel, often resulting in notch-like lesions near the gumline. It also causes the gums to permanently recede. Always use a soft-bristled brush and gentle pressure.
Are charcoal toothpastes safe to use every day?
No. Activated charcoal toothpastes are highly abrasive. While they may temporarily remove surface stains, daily use acts like sandpaper, permanently scratching the enamel. This roughened surface actually attracts more plaque and stains in the long run. Furthermore, most charcoal pastes lack fluoride, increasing your risk of cavities.
How often should I replace my toothbrush?
You should replace your manual toothbrush or electric brush head every 3 months, or sooner if the bristles begin to fray or splay outwards. Frayed bristles are completely ineffective at penetrating the gingival sulcus and disrupting plaque.
Does chewing sugar-free gum help clean my teeth?
Yes, as an adjunct when you cannot brush. Chewing sugar-free gum, particularly gum sweetened with Xylitol, stimulates a massive flow of saliva. This saliva washes away food debris, neutralizes plaque acids, and delivers calcium and phosphate to remineralize the enamel. Furthermore, Xylitol actively inhibits the growth of the cavity-causing bacteria Streptococcus mutans.
I have dental implants. Do they require special flossing?
Yes. Implants are attached differently to the gums than natural teeth, lacking the protective periodontal ligament. Plaque accumulation around an implant can quickly lead to peri-implantitis and bone loss. Use specific “implant-safe” floss, interdental brushes with coated wire (to prevent scratching the titanium), and a water flosser on a low setting to ensure meticulous plaque removal.
What should patients know about bad dental hygiene?
In clinical practice, bad dental hygiene is an essential factor in maintaining long-term oral health and preventing decay. Regular scaling, routine examinations, and personalized treatment plans are key to managing this aspect effectively.