

A dental hygiene session is a comprehensive clinical procedure focused on removing bacterial plaque, calculus, and surface stains from the teeth and gingival margins. Conducted by a dental professional, this preventive therapy halts periodontal disease progression, preserves enamel integrity, and establishes a foundation for long-term oral health.
Clinical Summary:
A professional dental hygiene session is a critical component of preventive and therapeutic dentistry, designed to manage the oral microbiome and prevent the onset of caries and periodontal disease. The clinical workflow typically involves a thorough periodontal assessment, mechanical debridement using ultrasonic and hand instruments, surface polishing, and targeted remineralization therapies. By disrupting pathogenic biofilms and removing calcified deposits (tartar) that cannot be eliminated through domestic oral care, these sessions mitigate localized gingival inflammation and reduce the risk of systemic health complications. Regular hygiene appointments are essential for maintaining the longevity of natural dentition and ensuring the success of restorative and cosmetic dental treatments.
Key Takeaways:
- Professional hygiene sessions disrupt pathogenic biofilms and remove calcified calculus that brushing alone cannot eliminate.
- The clinical workflow includes periodontal probing, ultrasonic scaling, hand instrumentation, and prophylaxis polishing.
- Advanced modalities like Air-Flow therapy offer superior interdental cleaning and stain removal with minimal abrasion.
- Optimal gingival health achieved through routine cleanings is a mandatory prerequisite for successful restorative procedures.
- Untreated calculus accumulation leads to gingivitis, periodontitis, and potential systemic health complications.
The Microbiology of Dental Biofilm and Calculus Formation
Understanding the pathogenesis of oral diseases begins with recognizing how acquired pellicle evolves into pathogenic biofilm and eventually calcifies into calculus, necessitating professional intervention.
The oral cavity is a complex, dynamic ecosystem harboring hundreds of distinct microbial species. Within minutes of brushing, a glycoprotein-rich layer known as the acquired pellicle forms over the enamel. While this pellicle acts as a protective barrier against acid attacks, it also serves as the primary attachment site for early bacterial colonizers, predominantly Gram-positive cocci such as Streptococcus mutans. If left undisturbed, this initial colonization rapidly evolves into a highly organized, three-dimensional microbial community known as dental plaque or biofilm.
As the biofilm matures, the microbial composition shifts toward more pathogenic, Gram-negative anaerobic bacteria, including Porphyromonas gingivalis and Treponema denticola. These microorganisms thrive in the oxygen-depleted environment of the gingival sulcus (the shallow crevice between the tooth and the gum). They produce metabolic byproducts, endotoxins, and enzymes that directly irritate the gingival tissues, triggering a localized inflammatory immune response known as gingivitis. Clinically, this manifests as erythema (redness), edema (swelling), and bleeding upon probing or brushing.
When bacterial biofilm is not adequately removed through daily mechanical oral hygiene, it undergoes a process of mineralization. Calcium and phosphate ions naturally present in saliva precipitate into the plaque matrix, transforming the soft biofilm into a hard, porous substance known as calculus (tartar)[1]. Calculus provides an ideal, rough surface for further bacterial adhesion, creating a vicious cycle of plaque accumulation and mineralization. Because calculus is firmly bonded to the tooth structure, it cannot be removed by a toothbrush or dental floss. Its eradication requires the specialized instruments and clinical expertise utilized during a professional dental hygiene session.

The Clinical Objectives of a Dental Hygiene Session
The primary goal of a dental hygiene session is to disrupt pathogenic biofilms, eliminate calcified deposits, and reverse early signs of gingival inflammation to prevent systemic oral diseases.
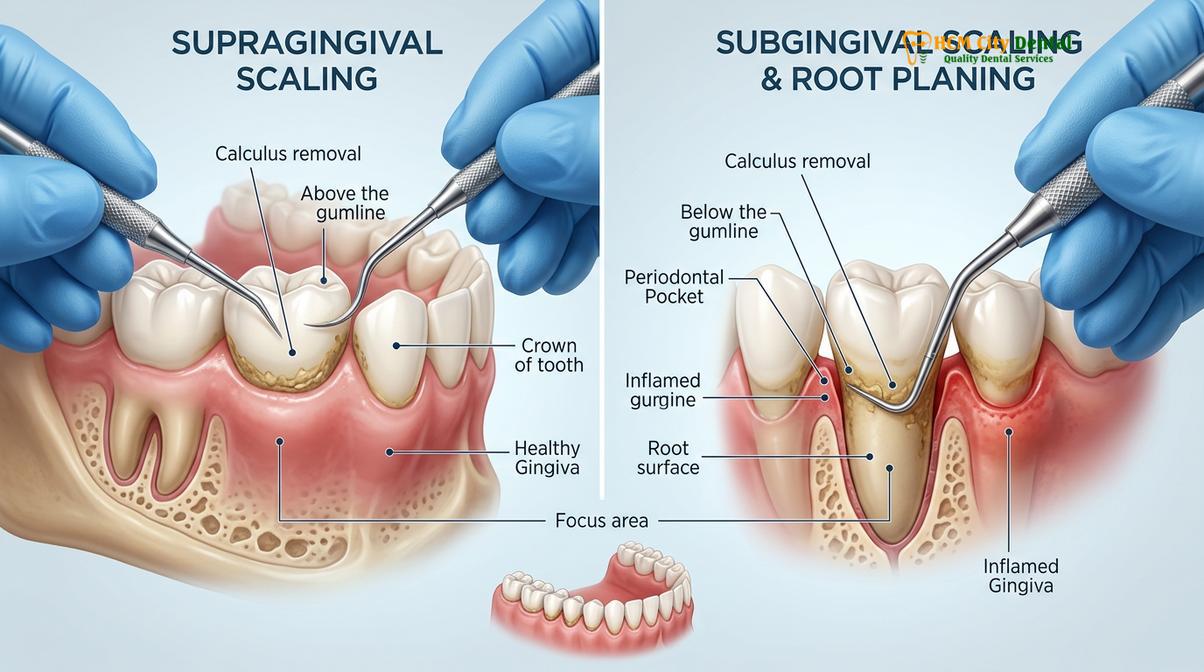
A professional dental hygiene session is far more than a cosmetic procedure designed to brighten a smile; it is a fundamental medical intervention aimed at disease prevention and tissue preservation. The clinical objectives encompass several critical aspects of oral health management. First and foremost is the complete mechanical debridement of supragingival (above the gumline) and shallow subgingival (below the gumline) calculus and plaque. By removing these local irritants, the dental professional eliminates the primary etiologic factors responsible for gingival inflammation and periodontal attachment loss.
Another vital objective is the early detection of oral pathologies. During the session, the clinician conducts a meticulous examination of the hard and soft tissues. This includes screening for carious lesions (tooth decay), assessing the integrity of existing restorations, and performing an oral cancer screening. By identifying these issues in their nascent stages, clinicians can implement conservative treatment strategies, thereby avoiding more invasive and costly procedures in the future.
Furthermore, a dental hygiene session serves as a critical educational touchpoint. The clinician evaluates the patient’s current home care efficacy and provides personalized instruction on proper brushing techniques, interdental cleaning methods, and dietary modifications. This collaborative approach empowers the patient to maintain the clinical results achieved during the appointment and fosters a proactive attitude toward long-term oral health. Understanding the various aspects dental professionals evaluate during these sessions highlights the comprehensive nature of preventive care.
Step-by-Step Workflow of a Professional Cleaning
A standard hygiene appointment follows a strict clinical protocol encompassing diagnostic assessment, mechanical debridement, surface polishing, and targeted remineralization therapies.
The execution of a professional dental hygiene session follows a systematic, evidence-based workflow designed to maximize clinical efficacy while ensuring patient comfort. The procedure is typically divided into several distinct phases, each utilizing specific instruments and techniques.
Phase 1: Comprehensive Periodontal Assessment
Before any mechanical cleaning begins, the clinician performs a thorough assessment of the patient’s periodontal status. This involves using a calibrated periodontal probe to measure the depth of the gingival sulcus around each tooth. Healthy sulcus depths generally range from 1 to 3 millimeters. Depths of 4 millimeters or greater may indicate the presence of periodontal pockets, signifying attachment loss and underlying bone resorption. The clinician also assesses for bleeding on probing (BOP), gingival recession, and tooth mobility. This diagnostic data dictates the specific approach and intensity of the subsequent cleaning phases.
Phase 2: Ultrasonic Debridement
The primary heavy lifting of calculus removal is achieved using an ultrasonic scaler. This sophisticated device utilizes high-frequency vibrations (typically between 25,000 and 30,000 cycles per second) to shatter and dislodge calcified deposits from the tooth surface. The ultrasonic tip is continuously cooled by a stream of water, which serves a dual purpose: it prevents thermal damage to the tooth pulp and creates a phenomenon known as cavitation. The rapid formation and collapse of microscopic water bubbles generate acoustic microstreaming, which effectively disrupts bacterial cell walls and flushes debris from the gingival sulcus[2].
Phase 3: Hand Instrumentation (Scaling)
Following ultrasonic debridement, the clinician utilizes specialized hand instruments, such as curettes and scalers, to perform fine detailing. These instruments are meticulously adapted to the complex contours of the tooth anatomy to remove any residual calculus, particularly in tight interproximal spaces and along the cementoenamel junction (CEJ). Hand instrumentation requires a high degree of tactile sensitivity and clinical skill to ensure complete deposit removal without causing iatrogenic damage to the root surface or surrounding soft tissues.
Phase 4: Prophylaxis Polishing
Once all hard deposits are removed, the teeth undergo a polishing phase. Using a slow-speed rotary handpiece equipped with a soft rubber cup or bristle brush, the clinician applies a specialized prophylaxis paste. This paste contains mild abrasives that gently remove extrinsic surface stains caused by dietary chromogens (such as coffee, tea, and red wine) and tobacco use. The goal is to achieve a perfectly polished dental surface, which not only enhances the aesthetic appearance of the smile but also creates a smooth topography that is less conducive to future bacterial adhesion.
Phase 5: Fluoride Therapy and Remineralization
The final step in many hygiene sessions involves the application of a topical fluoride treatment, typically in the form of a varnish or gel. Fluoride ions interact with the hydroxyapatite crystals in the tooth enamel, converting them into fluorapatite. This newly formed compound is significantly more resistant to acid dissolution caused by cariogenic bacteria. Fluoride therapy is particularly beneficial for patients with a high caries risk, exposed root surfaces, or dentin hypersensitivity, providing an essential layer of chemical protection.

Advanced Modalities: Air-Flow Therapy and Subgingival Debridement
For patients with heavy staining, orthodontic appliances, or active periodontal disease, advanced techniques like Air-Flow therapy and subgingival scaling provide superior bacterial eradication.
While traditional scaling and polishing are highly effective for routine maintenance, modern dentistry offers advanced modalities to address more complex clinical scenarios. One such innovation is Air-Flow therapy, a minimally invasive technology that utilizes a controlled stream of compressed air, warm water, and fine powder particles (such as erythritol or glycine) to eradicate biofilm and extrinsic stains. Unlike traditional rubber cup polishing, which relies on friction, Air-Flow utilizes kinetic energy to gently and efficiently clean the tooth surfaces, including deep pits, fissures, and complex interproximal areas.
Air-Flow therapy is particularly advantageous for patients undergoing orthodontic treatment, as it can easily navigate around brackets and wires without causing damage. It is also highly effective for cleaning around dental implants, where traditional metal instruments are contraindicated due to the risk of scratching the delicate titanium surface. The use of low-abrasion powders ensures that the enamel and restorative materials remain intact while achieving a superior level of cleanliness[3].
For patients diagnosed with active periodontitis, a standard prophylaxis is insufficient. These individuals require a therapeutic intervention known as Scaling and Root Planing (SRP), often referred to as a “deep cleaning.” SRP involves the meticulous removal of subgingival calculus and necrotic cementum from the root surfaces within deep periodontal pockets. The objective is to create a biologically acceptable, smooth root surface that facilitates the reattachment of the gingival tissues and reduces pocket depths. This procedure is typically performed under local anesthesia to ensure patient comfort and may require multiple visits to complete.
| Modality | Primary Indication | Mechanism of Action | Clinical Outcome |
|---|---|---|---|
| Standard Prophylaxis | Routine maintenance, gingivitis prevention | Ultrasonic & hand scaling, rubber cup polishing | Removal of supragingival calculus and surface stains |
| Air-Flow Therapy | Heavy staining, orthodontics, implant maintenance | Kinetic energy with air, water, and micro-powder | Superior biofilm eradication with minimal abrasion |
| Scaling & Root Planing (SRP) | Active periodontitis, deep pocketing | Subgingival instrumentation under local anesthesia | Removal of deep calculus, root smoothing, tissue reattachment |
“The transition from traditional mechanical scraping to advanced biofilm management utilizing kinetic air-polishing represents a paradigm shift in preventive dentistry. It allows us to achieve profound clinical cleanliness while preserving the microscopic integrity of the enamel and delicate restorative margins.”
— Clinical Perspective on Modern Hygiene Protocols
Integrating Hygiene with Restorative and Cosmetic Dentistry
Optimal gingival health achieved through professional hygiene is a mandatory prerequisite for the success of restorative procedures, including crowns, veneers, and composite bonding.
A pristine oral environment is the foundation upon which all successful restorative and cosmetic dental procedures are built. Prior to initiating any major dental repair, such as the placement of a dental crown or porcelain veneers, a comprehensive dental hygiene session is clinically mandatory. Inflamed, bleeding, or hypertrophic gingival tissues compromise the clinician’s ability to capture accurate digital or physical impressions, leading to poorly fitting restorations. Furthermore, the presence of moisture and blood from inflamed gums severely interferes with the adhesive bonding protocols required for modern restorative materials.
Patients frequently ask how long does dental bonding last; the answer is heavily dependent on the patient’s commitment to routine professional hygiene. Composite resin bonding and porcelain margins are highly susceptible to plaque accumulation. If biofilm is allowed to stagnate at the restorative margins, it creates an acidic environment that degrades the adhesive bond, leading to microleakage, recurrent decay, and premature failure of the restoration. Regular professional cleanings ensure that these critical margins remain free of destructive bacteria, significantly extending the lifespan of the restorative work.
For patients considering comprehensive aesthetic enhancements, understanding Who Can Get Veneers? Clinical Candidacy & Health Guidelines is crucial. Active periodontal disease is an absolute contraindication for elective cosmetic procedures. The underlying infection must be resolved, and the gingival architecture stabilized through targeted hygiene therapies before proceeding. This ensures that the final restorations are framed by healthy, stippled, pink gingiva, maximizing the aesthetic outcome.
At HCMC Dental Clinic in Ho Chi Minh City, our approach to General Dentistry emphasizes the seamless integration of preventive hygiene with advanced restorative care. Whether a patient is preparing for a single restoration or a complete Smile Makeover Vietnam: Clinical Costs, DSD & Veneer Packages, establishing optimal periodontal health is always the first step in our clinical workflow. This rigorous standard of care is particularly important for international patients navigating Veneers Abroad Safety: Clinical Guide & Verification Checklist, as it ensures long-term predictability and success.
The Oral-Systemic Connection: Why Hygiene Impacts Overall Health
Professional dental hygiene sessions are critical not only for preserving dentition but also for mitigating systemic inflammation linked to cardiovascular disease, diabetes, and adverse pregnancy outcomes.
The oral cavity is not an isolated system; it is the primary gateway to the rest of the body. Extensive medical research has established a profound bidirectional relationship between periodontal health and systemic well-being, commonly referred to as the oral-systemic connection. The pathogenic bacteria responsible for periodontitis, along with the inflammatory mediators (such as C-reactive protein and interleukins) produced by the body’s immune response, can enter the systemic bloodstream through ulcerated gingival tissues.
Once in the systemic circulation, these inflammatory markers can exacerbate various chronic conditions. For instance, there is a well-documented association between severe periodontal disease and an increased risk of cardiovascular events, including atherosclerosis, myocardial infarction, and stroke. The systemic inflammation originating from the oral cavity contributes to endothelial dysfunction and the formation of arterial plaques[4].
Furthermore, the relationship between periodontal disease and diabetes mellitus is highly synergistic. Patients with poorly controlled diabetes are significantly more susceptible to severe periodontitis due to impaired immune function and altered collagen metabolism. Conversely, the chronic inflammation associated with untreated periodontal disease increases insulin resistance, making it more difficult for diabetic patients to achieve glycemic control. Routine dental hygiene sessions play a crucial role in breaking this cycle by reducing the systemic inflammatory burden.
When to See a Doctor: Clinical Red Flags
While routine dental hygiene sessions are scheduled at regular intervals, certain clinical symptoms warrant immediate professional evaluation. Patients should not wait for their next scheduled appointment if they experience any of the following red flags. Spontaneous gingival bleeding—bleeding that occurs without provocation or during gentle brushing—is a clear indicator of acute inflammation or underlying pathology. Similarly, the presence of purulent exudate (pus) expressing from the gingival margins signifies an active, localized infection that requires urgent intervention.
Persistent halitosis (bad breath) that does not resolve with domestic oral hygiene is often a symptom of deep subgingival bacterial putrefaction associated with periodontal pockets. Additionally, any noticeable increase in tooth mobility, shifting of teeth, or changes in the way the upper and lower teeth occlude (bite together) suggests significant loss of the supporting alveolar bone. These symptoms require a comprehensive diagnostic evaluation, including radiographic imaging, to determine the extent of the disease and formulate an appropriate treatment plan.
Important Clinical Warning: Ignoring signs of gingival bleeding, persistent bad breath, or tooth mobility can lead to irreversible bone loss and eventual tooth extraction. Early intervention through professional periodontal therapy is critical to halting disease progression and preserving natural dentition. Always consult a qualified dental professional for an accurate diagnosis.
Patient Case Study: Periodontal Stabilization and Maintenance
Clinical case studies demonstrate how routine hygiene interventions can halt aggressive periodontal attachment loss and restore gingival architecture.
Clinical Case: Comprehensive Periodontal Management
Patient Profile: A 45-year-old male presented to HCMC Dental Clinic in Ho Chi Minh City with complaints of chronic gingival bleeding, halitosis, and generalized tooth sensitivity. He had previously relied on sporadic visits to a basic corner dental practice and had not received a professional cleaning in over three years.
Clinical Assessment: Dr. Nguyen Van Cuong conducted a comprehensive periodontal examination, revealing generalized moderate to severe calculus accumulation, significant gingival erythema, and localized periodontal pockets measuring 5-6mm in the posterior quadrants. Radiographs confirmed early crestal bone loss.
Treatment Protocol: The patient underwent a phased treatment plan beginning with full-mouth Scaling and Root Planing (SRP) under local anesthesia to remove deep subgingival deposits. This was followed by Air-Flow therapy to eradicate residual biofilm and a targeted chlorhexidine irrigation. The patient was placed on a strict 3-month periodontal maintenance recall schedule.
Outcome: After six months of rigorous professional maintenance and improved home care, the patient’s gingival tissues exhibited a return to a healthy, stippled appearance. Bleeding on probing was reduced to less than 5%, and pocket depths stabilized at 2-3mm. The case highlights the critical importance of transitioning from a traditional corner dental setup to a specialized clinical environment for effective disease management.
Post-Session Care and Long-Term Maintenance
Sustaining the clinical results of a hygiene session requires rigorous at-home mechanical plaque control and adherence to a personalized recall schedule.
The clinical success achieved during a professional dental hygiene session is transient if not supported by meticulous domestic oral care. The rapid recolonization of bacterial biofilm means that patients must actively manage their oral hygiene on a daily basis. The foundation of home care is the mechanical disruption of plaque through brushing. Clinicians generally recommend the Modified Bass technique, which involves angling the toothbrush bristles at a 45-degree angle toward the gingival margin and using short, vibratory strokes to clean the sulcus effectively.
However, brushing alone only cleans approximately 60% of the tooth surface. The interproximal areas—the spaces between the teeth—are highly susceptible to plaque accumulation and require specific tools for adequate cleaning. Depending on the patient’s interdental anatomy, the clinician may recommend traditional dental floss, interdental brushes, or water flossers. Interdental brushes are particularly effective for patients with wider embrasure spaces or mild gingival recession, as they physically sweep away biofilm from the concave root surfaces.
In addition to mechanical cleaning, the use of adjunctive chemical agents can enhance biofilm control. Fluoridated toothpaste is universally recommended to promote continuous enamel remineralization[5]. For patients with a high risk of gingivitis, a therapeutic mouthrinse containing essential oils or cetylpyridinium chloride (CPC) may be prescribed to reduce bacterial load. It is crucial to follow the specific product recommendations provided by the dental professional, as indiscriminate use of certain antimicrobial rinses can disrupt the natural balance of the oral microbiome.
Finally, adherence to a personalized recall schedule is paramount. While the standard recommendation is a hygiene session every six months, this interval is not universally applicable. Patients with a history of periodontal disease, high caries susceptibility, or systemic risk factors may require maintenance visits every three to four months. Dr. Nguyen Van Cuong emphasizes that these customized recall intervals are based on clinical diagnostics and are essential for intercepting disease recurrence before irreversible damage occurs.
“The true value of a dental hygiene session extends far beyond the clinic chair. It is a collaborative partnership between the clinician and the patient, where professional intervention resets the biological baseline, and diligent home care sustains it.”
— Dr. Nguyen Van Cuong, HCMC Dental Clinic

For patients seeking comprehensive preventive care or preparing for advanced restorative treatments, establishing a foundation of optimal periodontal health is essential. To learn more about our clinical protocols or to schedule a comprehensive evaluation, explore our Smile Makeover Guide: Clinical Steps, Costs & Veneer Options and discover the standard of care at HCMC Dental Clinic.
Frequently Asked Questions
How often should I schedule a professional dental hygiene session?
Most patients benefit from a dental hygiene session every six months. However, individuals with a history of periodontal disease, heavy calculus accumulation, or systemic conditions like diabetes may require a customized recall interval of three to four months to maintain optimal gingival health. Your clinician will determine the appropriate frequency based on a comprehensive assessment of your specific risk factors and clinical presentation.
Is a dental hygiene session painful?
A standard dental hygiene session is generally well-tolerated and should not cause severe pain. Patients with dentin hypersensitivity or active gingival inflammation may experience mild discomfort, which can be effectively managed with topical anesthetics or adjustments to the ultrasonic scaler settings. Open communication with your hygienist ensures that the procedure is adjusted to maximize your comfort throughout the appointment.
Can a hygiene session remove deep intrinsic tooth stains?
A hygiene session effectively removes extrinsic surface stains caused by coffee, tea, or tobacco. However, deep intrinsic stains located within the dentin or enamel structure require professional chemical teeth whitening or restorative solutions like veneers to alter the underlying tooth color. During your session, the clinician can evaluate the nature of your discoloration and recommend the most appropriate aesthetic treatment.
What is the difference between a standard cleaning and deep cleaning?
A standard cleaning focuses on the supragingival (above the gumline) removal of plaque and calculus for preventive maintenance. A deep cleaning, or scaling and root planing, is a therapeutic procedure that removes subgingival deposits and smooths root surfaces to treat active periodontal disease. Deep cleanings are typically performed under local anesthesia and are essential for halting the progression of bone loss associated with periodontitis.
Why do my gums bleed during a dental hygiene session?
Gingival bleeding during a cleaning is a clinical indicator of localized inflammation, known as gingivitis, caused by bacterial biofilm irritating the soft tissues. As the pathogenic plaque and calculus are removed, the inflammation subsides, and the bleeding typically resolves within a few days. Consistent professional cleanings and improved home care are necessary to eliminate the underlying infection and restore tissue health.
References
- Journal of Clinical Periodontology. The role of professional mechanical plaque removal in periodontal maintenance. (2021).
- American Dental Association (ADA). Evidence-based clinical practice guideline on the nonsurgical treatment of chronic periodontitis. (2015).
- International Journal of Dental Hygiene. Efficacy of air-polishing devices in biofilm removal and surface alteration. (2020).
- Periodontology 2000. The oral-systemic connection: Periodontal disease and systemic health. (2019).
- Journal of Dental Research. Mechanisms of fluoride action in caries prevention and enamel remineralization. (2022).



